
Abstract
Background:
The ownership and sharing of patient medical data is an increasingly contentious subject in medicine generally but also within the field of Parkinson’s disease (PD). Despite being the providers of the medical data, patients are rarely consulted as to its usage.
Objective:
The objective of this paper is to establish patient attitudes to ownership of their own medical data and the sharing thereof.
Methods:
We report here the results of an online survey of people with Parkinson’s. A total of 310 people took part in the ‘sharing data’ component of the survey, answering some or all of the questions for which they were eligible.
Results:
Most respondents (208/306) were aged between 55 and 74 years. 55% of the sample were female and the mean number of years diagnosed was 7.1. Although 93% of respondents were willing to share data, only 41% were currently doing so and a further 8% did not know whether they were sharing any information in this way. There was a significant association between age and data sharing (p = 0.006). However, no clear relationship was found between data sharing and the number of years diagnosed, sex, medication class or health confidence. There was also no consensus among patients on ownership of, access to and usage of their research data.
Conclusion:
The lack of consensus on data ownership and general absence of clear demographic predictors of data sharing implies impaired communication pathways. We suggest that strategies directed towards improved communication may help to clarify data ownership and promote data sharing.
INTRODUCTION
The increasing complexity of modern medical data, and its linkage with disease conditions, makes the ownership of data and medical information a key issue [1]. Complex medical data in general poses ethical dilemmas previously unknown to medicine. At the same time, digitisation of data provides opportunities and threats. On the one hand digitisation facilitates large-scale data comparisons and forms the bedrock of so-called big data [2]. On the other hand digitisation lends itself much more readily to data piracy or theft [3].
The vending of casually acquired medical data to insurers by websites raised the spectre of medical data being routinely accessible to insurance companies [4]. This in turn has flagged up the question of data ownership with a number of stakeholders expressing interest.
Chief among these are often patient advocacy groups and, in the context of long-term illness, these seek to promote the centrality of the patient among stakeholders and often to establish the primacy of patient claims to ownership of data.
This paper reports the results of a survey of people with Parkinson’s intended to establish patient attitudes to their own medical data and the ownership and sharing thereof.
METHOD
A thirty-seven question online survey (using Survey Monkey) was developed by Parkinson’s Movement (PM: www.parkinsonsmovement.com), an international patient-driven action group created by The Cure Parkinson’s Trust (CPT: www.cureparkinsons.org.uk), a UK-based research charity. The survey was shaped with input from a small patient advisory group, broadly representative of the study sample demographic (see results).
A link to the survey was posted on the CPT website and other social media. We also included a link in the regular CPT electronic newsletter and asked other Parkinson’s charities (for example, The Michael J Fox Foundation, National Parkinson’s Foundation, Davis Phinney Foundation, Northwest Parkinson’s Association and Parkinson’s UK) to do the same. Finally, the survey was also circulated to those attending the Rallying to the Challenge conference in Grand Rapids, Michigan, USA organised by the Van Andel Research Institute (VARI). Collectively these amounted to a reach of about 28,000 people. The survey was not incentivised and was active from 09/06/2016 to 13/09/2016.
The survey comprised 4 broad sections: Background information (questions 1–7) Health confidence (questions 8–18) Sharing data (questions 19–35) Future correspondence (questions 36 & 37)
Section 1 gathered general background information including year of diagnosis, sex, age category, frequency of Parkinson’s healthcare appointments and living arrangements. Section 2 examined health confidence [5] and medication management. Section 3 related to sharing data; what information is the most useful to collect for research purposes, how such information could improve care and research, motivations for sharing data, the most useful tools to collect data, willingness to share information for research purposes and whether people were currently sharing. If people were sharing information for research purposes they were asked further questions regarding issues of how they were sharing their data, anonymisation, ownership, access and communication about data usage. Section 4 refers to willingness to take part in future research.
The results reported here are those pertaining to potential factors (age, health confidence, number of years diagnosed, sex and current medication classes) influencing data sharing. We further examine patient attitudes to data collection, ownership and sharing.
Questions were a mixture of YES/NO, multiple choice and free text (See Appendix 1 for the full survey). All multiple choice questions had an ‘other-please specify’ option. Questions marked with an asterisk required an answer. For the remainder, respondents could continue without answering. Statistical analysis was carried out using the Pearson’s chi-square (χ2) test (IBM SPSS v23.0).
RESULTS
Demographics
A total of 394 people with Parkinson’s took part in the survey. Of these, 310 people addressed the ‘Sharing data’ section (questions 19 –35), answering most or all of the questions for which they were eligible. These form the basis of the analysis presented here.
There was a roughly even split between male and female respondents (45% and 55% respectively, n = 306). Respondents (n = 306) were predominantly UK (31%), USA (27%) and Canada (21%) based but, in total, responses covered 20 countries and 5 continents, the majority of which were English speaking. Most respondents (208/306) were aged between 55 and 74 years and the mean number of years diagnosed was 7.1 (range 0–25 years, dating between 1991 and 2016 [n = 310]). 83% lived with someone, mostly with a spouse (256/309) and the majority lived in a house (221/308) or a single floored dwelling (75/308), for example a flat, apartment or bungalow. 55% (170/309) of respondents reported that they see their neurologist once or twice a year but see other healthcare professionals (for example, physiotherapist, Parkinson’s nurse, and speech therapist) more regularly.
Sharing data
In response to the question ‘if people with Parkinson’s come together to share their data for research purposes, what information do you think would be the most useful to collect?’ respondents reported that information about non-motor (79%, 245/310) and motor symptoms (76%, 237/310), followed by medical history (44%, 136/310) and genetic information (41%, 127/310) would be the most useful information to collect. 84% (259/310) of respondents reported that collecting such data could improve research by providing a better understanding of Parkinson’s and the possible non-motor subtypes and 62% (192/310) thought it would provide a means for monitoring the disease remotely during clinical trials. It was also reported that by collecting such data, care would be improved by allowing personalised treatment plans (72%, 224/310), by helping them understand their individual experience with Parkinson’s (68%, 212/310), by helping their healthcare team understand their type of Parkinson’s (67%, 207/310) and by allowing monitoring of fluctuations and progression of the disease (63%, 194/310). Very few respondents (4%, 13/310) stated that this information would improve neither research nor care.
Although 93% of respondents (288/310) were willing to share information/data about their Parkinson’s for research purposes, only 41% (128/310) were currently doing so and a further 8% (25/310) did not know whether they were sharing any information in this way.
A Pearson’s chi-square analysis revealed a significant relationship between data sharing status and age (χ2(12) = 27.99, p = 0.006). Figure 1 shows the proportion of respondents sharing, not sharing or unaware of whether they were sharing data for research purposes as a function of age. Further individual age group comparisons showed significant differences between the 75 and over age group and those in the 35–44 (χ2(2) = 12.86, p = 0.002), 45–54 (χ2(2) = 10.81, p = 0.004), 55–64 (χ2(2) = 16.09, p < 0.001) and 65–74 (χ2(2) = 19.75, p < 0.001) categories. No other age group comparisons showed significant differences.
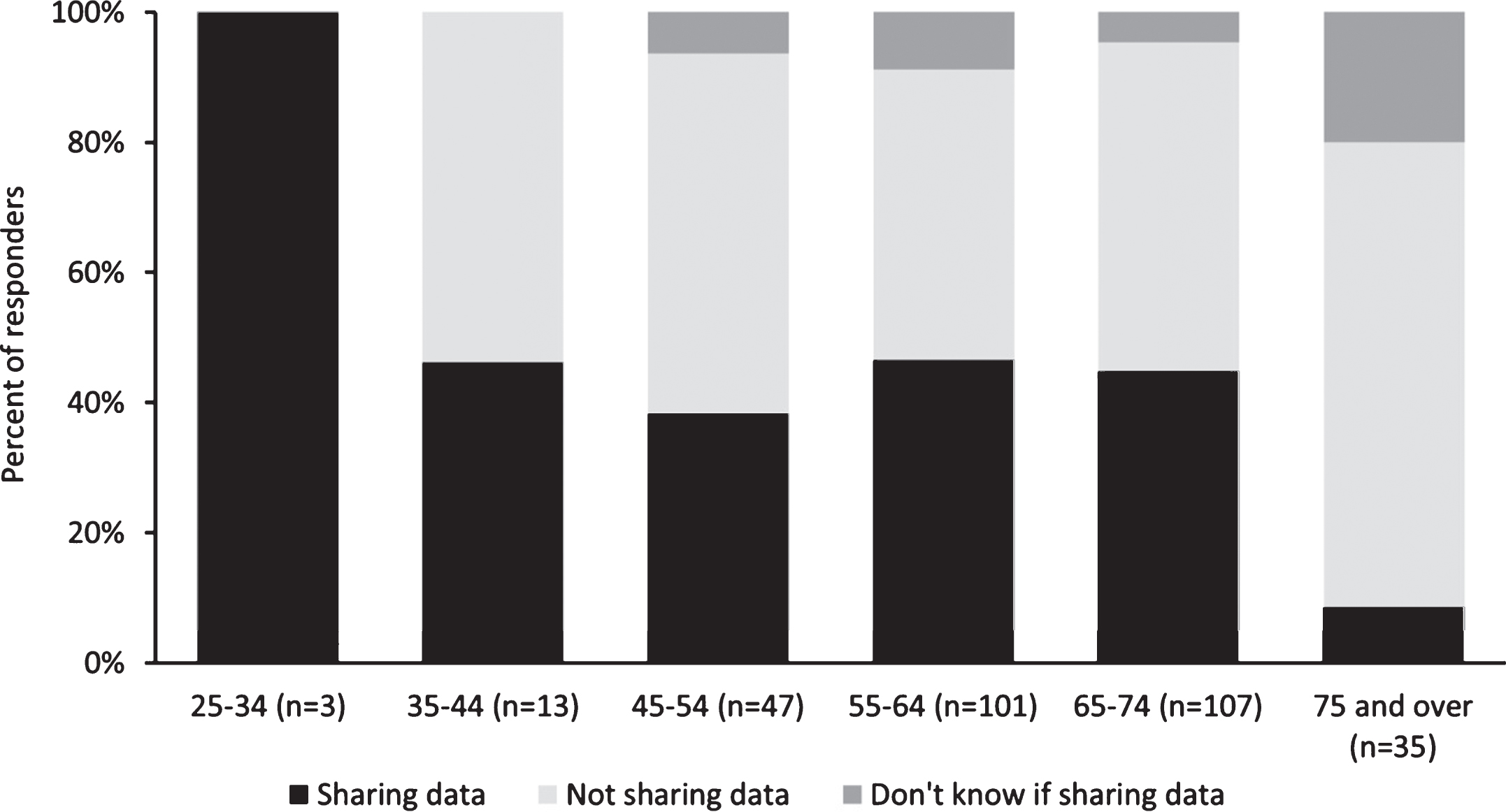
Percentage of respondents in each age category who are sharing data, not sharing data and do not know if they are sharing data for research purposes.
Figure 2 shows the proportion of respondents sharing, not sharing or unaware of whether they were sharing data for research purposes as a function of health confidence scores. Pearson’s chi-square analysis revealed a significant relationship between data sharing status and health confidence scores (χ2(20) = 33.84, p = 0.027). Comparison of high health confidence scores (7–10) with the remainder according to the classification of Wasson & Coleman [5] revealed no significant difference (χ2(2) = 2.02, p = 0.364).
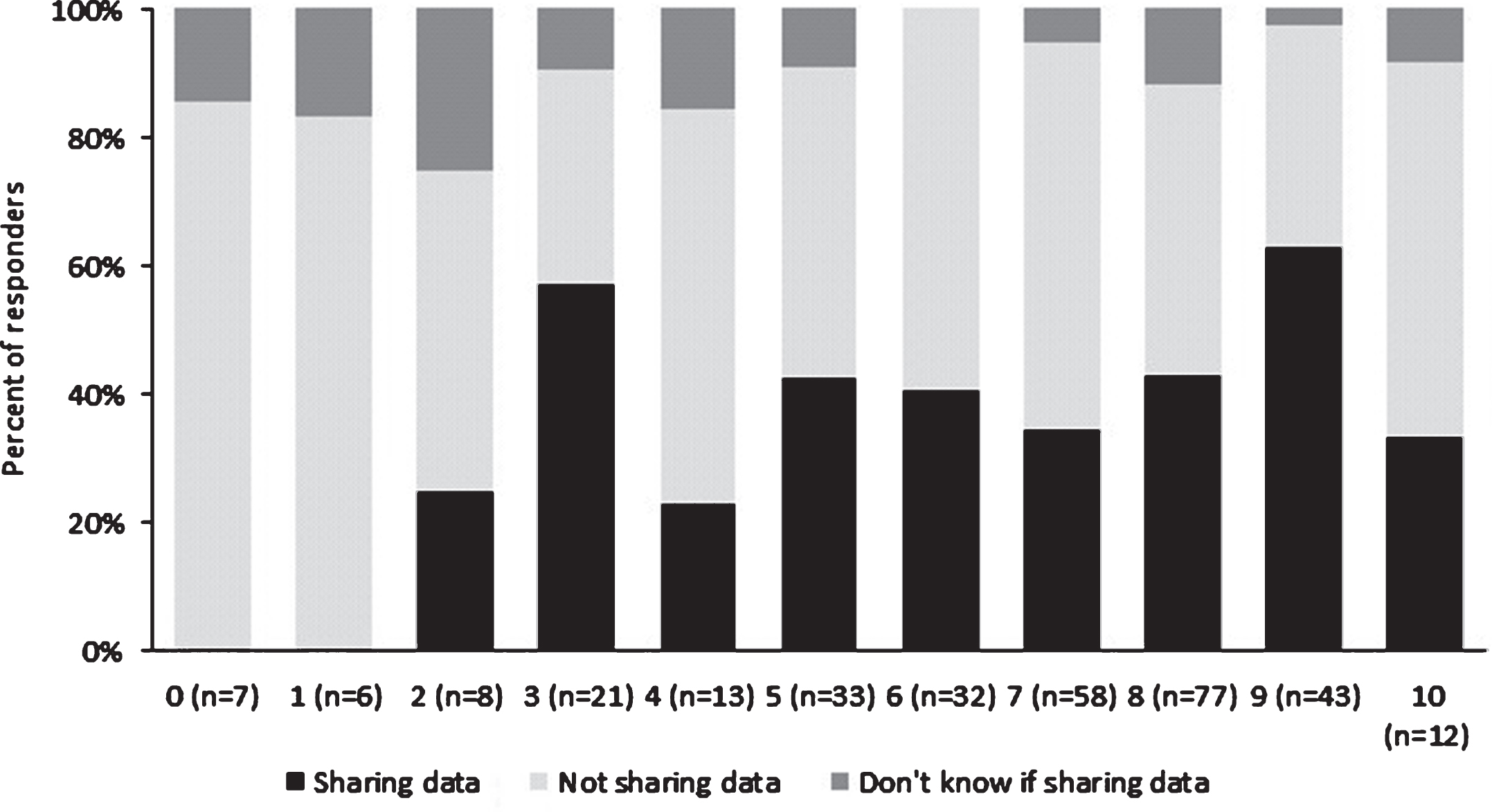
Percentage of respondents actively sharing data for research purposes as a function of health confidence.
We compared data sharing status in patients who were either taking or not taking several medication classes used in Parkinson’s. None of the following medication groups were significantly associated with data sharing status: dopamine agonists (χ2(2) = 4.05, p = 0.132), MAO-B inhibitors (χ2(2) = 3.58, p = 0.167), anti-cholinergics (χ2(2) = 1.24, p = 0.537), COMT inhibitors (χ2(2) = 0.29, p = 0.866), L-dopa combinations (χ2(2) = 1.16, p = 0.560) and amantadine (χ2(2) = 3.51, p = 0.173). Nor was there any significant relationship between data sharing status and the number of years diagnosed (χ2(4) = 46.00, p = 0.555) or sex (χ2(2) = 1.44, p = 0.488).
Of the 51% (157) of respondents who were not sharing their data for research purposes, 78% (119) had never been asked to. However, gaining personal insights from the data (68%, 107/157), understanding exactly how the data will be used (57%, 90/157), assured anonymity of the data shared (48%, 75/157) and knowing exactly who will access the data (38%, 59/157) would motivate respondents to share their data in the future.
Of the 41% of respondents currently sharing data, 39% (49/125) shared via personal technology such as a smartphone. 60% (74/123) felt their data was fully anonymised but 30% (37/123) did not know whether it was anonymised or not. In response to the questions ‘who do you think owns your data?’ and ‘who do you think should be able to access it?’ there were mixed views (Fig. 3). However, the majority (67%, 84/126) believed they should be informed when their data is used, most conveniently via email (83%, 70/84).
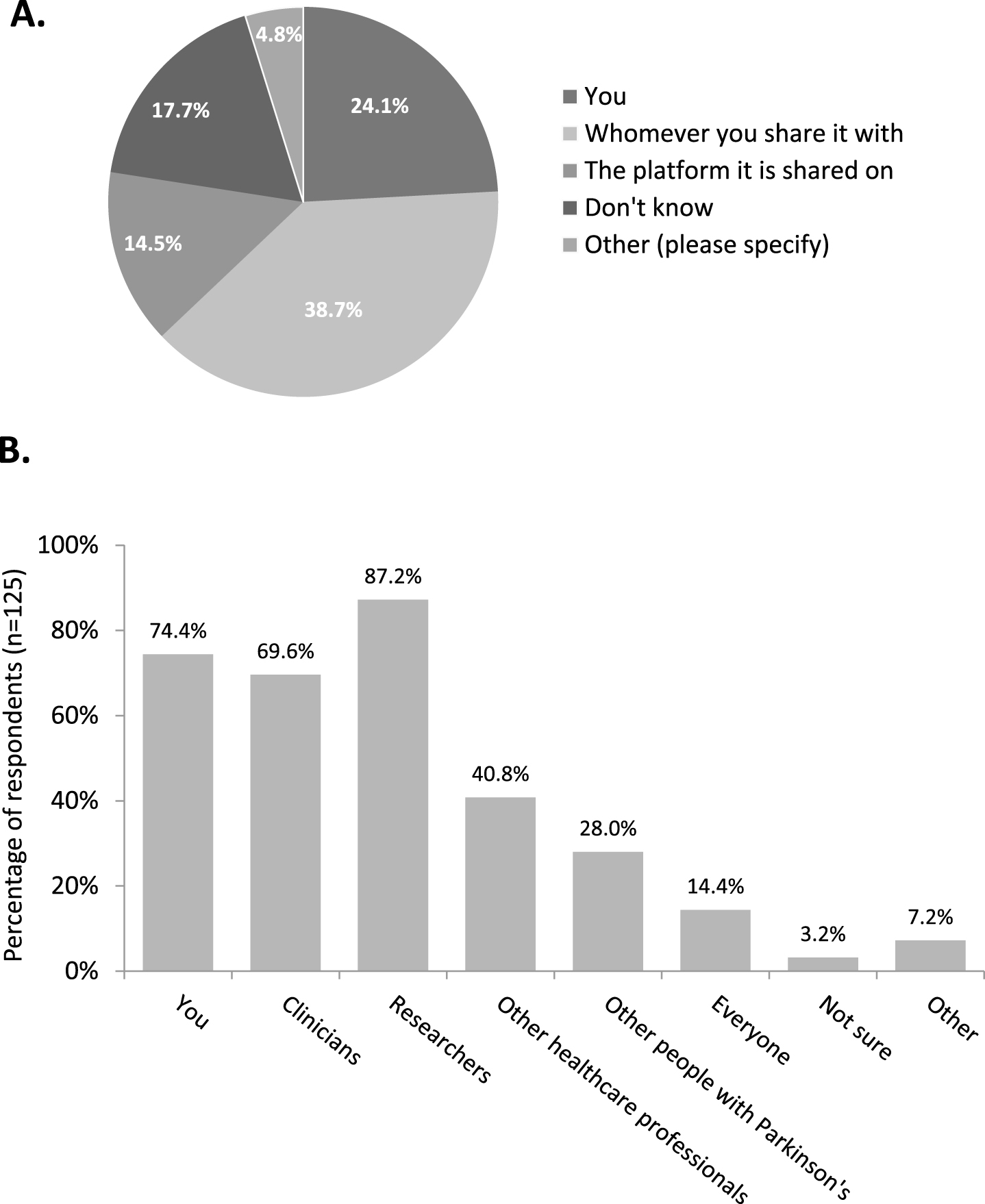
Responses to the questions who do you think owns your data (n = 124) (A) and who do you think should be able to access your data (n = 125) (B).
DISCUSSION
Data sharing is an increasingly important issue in medical research. Ownership of data and of products derived therefrom is likely to dominate medical research going forward. This report examines the attitudes and understanding of Parkinson’s patients of data collection and sharing.
Firstly, in connection with data collection to improve research, the focus was very much on symptoms, both non-motor and motor, as opposed to general health information, personal information, genetic information and medical history. The vast majority felt that collecting data could improve research by providing better understanding of Parkinson’s in relation to possible non-motor subtypes.
Perhaps a logical correlate of data collection is the utilisation of the information gathered. Despite 93% being willing to share information, fewer than half of these actually did. Moreover nearly one in ten of those willing to share data did not know whether they were. This dissociation between volition and act is, at first sight, perplexing. One would anticipate that the desire to share should translate into action. We therefore examined some of the possible reasons why patients might or might not share their information for research purposes.
One factor significantly associated with data sharing was age. Patients aged 75 and above were less likely to share data than the younger groups (Fig. 1). This may reflect a generally more conservative outlook and reticence to adopt technology [6].
The situation with respect to health confidence was more complex. Health confidence is considered to reflect patient engagement [5, 8]. The relationship between data sharing status and health confidence was equivocal. Initial analysis using individual scores appeared to reveal a significant relationship between data sharing status and health confidence. However, when the health confidence scores were grouped into high (7–10) and low (0–6) health confidence according to the classification of Wasson & Coleman [5], there was no significant difference. Figure 2 illustrates that none of the patients with negligible health confidence shared their data and this may have biased the individual score analysis. That said, it could be argued that data sharing needs some threshold level of health confidence.
Several other factors examined (sex, number of years post-diagnosis and medication classes) were not significantly associated with data sharing status.
Looking more closely at those who did not share their data (just over half), the principal finding is that the substantial majority either were not asked to share their data or could not recollect being asked. Coupled with the 8% who did not know whether or not they were sharing data, this suggests a failure of communication. Either research organisers failed to make it clear the data would be shared or failed to ensure adequate patient comprehension. Nevertheless, whether this is a transmission or reception issue, the outcome is nonetheless the same.
This may be partly due to confusion over perceived ownership of data. When patients who were sharing their data were asked who they felt owned the data, there was a broad range of opinion (Fig. 3A) with around one in four believing the data was owned by the patients themselves. Around a third felt that ownership resided with whomsoever they had chosen to share it with, while a seventh attributed ownership to the platform upon which it was shared.
This is an important point. Establishment of ownership of data is or should be a key part of the consenting procedure for patients participating in research. In this regard, failure to ensure adequate understanding on behalf of the patient can, at worst, amount to an unsafe consent.
In this context, patients felt that clinicians, researchers and the patients themselves had the strongest claims to access the data. Key issues motivating respondents to share data were personal insights to be gained, how the data was to be used and accessed and, not surprisingly, the reassurance of anonymity.
The vast majority of respondents were keen in principle to share their data for research purposes. However considerably fewer (41%) were actually sharing. Coupled with the lack of consensus on data ownership and general absence of clear demographic predictors of data sharing, the picture is one of confusion, possibly engendered by communication failures. Communication is central to all clinical practice and research and the absence of effective communication and understanding has implications for the safety and viability of research and clinical management. On the positive side, this suggests that strategies directed towards improved communication may help to clarify data ownership and promote data sharing.
Finally and by way of caveat, we should add that there are legitimate concerns that all online surveys may be subject to selection bias. Without knowing exactly how many people could access the survey, it is impossible to calculate the response rate and therefore how representative this sample is of the Parkinson’s population. Typically online response rates range from 20–47% [9].
Furthermore, the number that completed the ‘Sharing data’ section of the survey (310) is lower than the number that started the survey overall (394). Of the 84 ‘dropouts’ on questions 1–18 the majority (67/84) dropped out of the survey on reaching mandatory continuation points (i.e. questions that had to be answered in order to continue).
It is a reasonable supposition that those who respond to surveys are, almost by definition, willing to share personal information. Thus it is unsurprising that 93% of respondents were in principle willing to share information for research purposes. More surprising is that even these patients are not.
CONFLICT OF INTEREST
The authors confirm that no financial or material support was provided in the production of this paper and there are no commercial or other conflicts of interest in connections with its submission.