
Abstract
Objective:
This study aimed to validate the single breath count test (SBCT) against volitional measures of respiratory muscle function in healthy subjects and people with neuromuscular disorders (NMD; n = 100 per group).
Methods:
Testing comprised upright and supine SBCT, forced vital capacity (FVC), maximum inspiratory pressure (MIP), and sniff nasal inspiratory pressure (SNIP). Predictability of FVC by SBCT was assessed using logarithmic regression analysis. Receiver operating characteristics curves were used to identify SBCT thresholds for lung restriction (FVC < 80% predicted), inspiratory muscle weakness (MIP < 60 cmH2O), and indication for non-invasive ventilation (NIV) in NMD patients.
Results:
In both groups, SBCT showed moderate correlation with FVC. In patients, SBCT values were also correlated with MIP and SNIP. Strength of correlations was similar with supine and upright SBCT which accounted for 23.7% of FVC variance in healthy individuals (44.5% in patients). Predictive thresholds of upright SBCT were < 27 for MIP < 60 cmH2O (sensitivity 0.61/specificity 0.86), <39 for NIV indication (0.92/0.46), and <41 for FVC < 80% predicted (0.89/0.62).
Conclusion:
The SBCT is positively correlated with spirometry. It predicts both lung restriction and NIV indication in NMD patients. The SBCT allows for remote monitoring and may substitute for spirometry/manometry if appropriate devices are unavailable.
Keywords
HIGHLIGHTS
The single breath count test (SBCT) is a simple tool to assess inspiratory capacity. Upright and supine SBCT are positively related to spirometry in healthy subjects. In NMD patients, SBCT relates to spirometry and maximum inspiratory pressure. In patients, SBCT predicts lung restriction and the need for mechanical ventilation.
LIST OF ABBREVIATIONS
Amyotrophic lateral sclerosis
American Thoracic Society
Deutsche Gesellschaft für Muskelkranke
Forced expiratory volume in one second
Functional residual capacity
Forced vital capacity
Maximum inspiratory pressure
Non-invasive ventilation
Peak expiratory flow
Residual volume
Sniff nasal inspiratory pressure
INTRODUCTION
Respiratory muscle weakness is a prominent feature in numerous neuromuscular disorders (NMD) including amyotrophic lateral sclerosis (ALS), spinal muscular atrophy, poliomyelitis, Guillain-Barré syndrome, and various distinct myopathies and muscular dystrophies [1]. In a disease continuum, respiratory muscle involvement advances from sleep-related hypoventilation to type II respiratory failure [2]. Associated clinical symptoms may comprise insomnia, non-restorative sleep, fatigue, dyspnea, exercise intolerance, and impaired cough [3]. In many conditions, respiratory muscle weakness substantially adds to the burden of disease and is a major cause of premature death [4, 5]. As mechanical ventilation is known to alleviate clinical symptoms and improve long-term prognosis [6, 7] respiratory muscle strength testing is crucial to identify the need for diagnostic sleep studies and ventilatory support. For this purpose, vital capacity and maximum mouth occlusion pressures are widely established tests and may easily be performed using handheld devices [8]. As an even more simple bedside measure of inspiratory capacity, the single breath count test (SBCT) has been applied in healthy subjects and people with distinct NMD [9–13]. With slight variations, SBCT protocols require that probands or patients take a maximum deep breath and count in their normal voice as far as possible without inhaling again and at a given rate.
In the light of the COVID-19 pandemic the SBCT might be particularly useful for telephone or video assessment of inspiratory capacity in patients unable or reluctant to undergo on-site pulmonary function testing. In previous studies, validation of the SBCT was mostly performed against one external parameter only, such as forced vital capacity (FVC), forced expiratory volume in one second (FEV1), or peak expiratory flow (PEF). These are global measures of lung function that do not directly reflect inspiratory muscle strength, and correlation of the SBCT with maximum inspiratory pressure has been performed in one study only [14]. Moreover, in previous studies that applied the SBCT in patients with NMD sample size was small with only few conditions taken into account [12, 15]. Only in ALS, the SBCT has been shown to predict severe lung restriction and the need for mechanical ventilation which was defined as FVC < 50% predicted [13]. Thus, it is still unknown whether the SBCT is suitable for monitoring of respiratory function in people with various NMD, including prediction of nocturnal hypoventilation that indicates the need for non-invasive ventilation (NIV) before respiratory failure has fully developed [16]. The present study aimed to comprehensively evaluate validity and suitability of the SBCT in a large cohort of healthy individuals and people with NMD. We hypothesized that the SBCT would be a simple and feasible measure of pulmonary function that could screen for lung restriction and guide further diagnostic work-up.
METHODS
Study design
Between October 2020 and September 2021, 100 healthy adult individuals and 100 adult people with NMD were sequentially enrolled in this study and underwent a structured test protocol comprising single breath counting, FVC, FEV1, PEF, maximum inspiratory pressure (MIP), and sniff nasal inspiratory pressure (SNIP). The latter is a reasonable surrogate for MIP if facial muscle weakness prevents a tight lip seal [8, 17]. For healthy probands, the absence of any neurological or pulmonary disease was required. Active smokers and subjects with morbid obesity (body mass index/BMI>40) were excluded. People with NMD were recruited from the neuromuscular outpatient clinic or the NMD respiratory unit, respectively. Patients with tracheostomy, severe dysarthria or complete loss of speech were excluded. Study participants completed the German version of the Borg Rate of Perceived Exertion Scale immediately before testing started [18]. Volitional tests – SBCT, spirometry, MIP and SNIP – were explained and supervised by one investigator (E. K.). Each test was repeatedly performed in the upright and supine position. Written informed consent was obtained from all participants. The study was approved by the local ethics authority (Ethikkommission der Westfälischen Wilhelms-Universität Münster und der Ärztekammer Westfalen-Lippe, 2020-688-f-S).
Single breath count test (SBCT)
The SBCT procedure was thoroughly explained and demonstrated by the investigator. Participants had to take a maximal inhalation and count as long as possible in a normal voice with a single breath. Counting had to be in concordance with a digital metronome set at 2 beats per second and providing both visual and audible cues (Android smartphone application The MetronomeTM, Version 1.25.2, Soundbrenner, Berlin, Germany). Counting began with the number “1”. Testing only proceeded if participants had shown their ability to reliably conduct the procedure. In each position, upright and supine, three attempts were performed and the best value was documented.
Spirometry
Spirometry was performed using a handheld electronic spirometer (Vitalograph Micro SpirometerTM, Vitalograph, Hamburg, Germany). Measurements were conducted in accordance with current recommendations [8]. In each position, at least 3 consecutive tests were performed until the best result was achieved and showed less than 10% variation from the preceding attempt. FVC was expressed in absolute numbers and as percentage of the predicted value based on gender, height, and age [19]. A nasal clip was used for all tests to prevent air leaks.
Inspiratory muscle strength tests
For assessment of inspiratory muscle strength, MIP and SNIP were measured. Both pressures were recorded using a handheld electronic manometer (MicroRPMTM, CareFusion, Baesweiler, Germany). For MIP recordings, a flanged mouthpiece and a nasal clip were used. For SNIP measurements, one nostril was tightly occluded by the pressure-sensing probe while the contralateral nostril was left open [20, 21]. Participants were instructed to inhale strongly and maximally for at least 3 seconds. MIP was measured from residual volume (RV), i. e. following maximum exhalation [8, 22]. For comparability reasons, SNIP was also measured from RV instead from functional reserve capacity (FRC) as originally proposed [17]. From three consecutive attempts, the best result was used for data analysis.
Statistical analysis
Statistical data analysis was performed using IBM SPSS® 26.0 (IBM, Armonk, NY, USA). Normal distribution was assessed using the Shapiro-Wilk test. Results are presented as mean and standard deviation or median and interquartile range, respectively. For intergroup comparison the paired t-test or the Wilcoxon signed rank test were used for dependent variables, as appropriate. For independent variables the two-sample t-test or the Mann-Whitney U test were used depending on distribution.
Correlations between continuous variables were analyzed using Pearson’s correlation coefficient (r) in case of normal distribution and Spearman’s Rho (ρ) for non-parametric data. Strength of correlation was categorized as weak (r = 0.10–0.39), moderate (r = 0.40–0.69), strong (r = 0.70–0.89), or very strong (r = 0.90–1.0) [23]. P-values<0.05 were considered statistically significant. Linear regression analysis was performed to test whether the SBCT predicts FVC and MIP. As both lung capacity and inspiratory muscle strength are not physiologically infinite a logarithmic model was additionally applied.
To identify SBCT thresholds that indicate either lung restriction (FVC < 80%) or inspiratory muscle weakness (MIP < 60 cmH2O) receiver operating characteristics (ROC) analyses were performed. Based on individual coordinate points on the ROC curve, sensitivity, specificity and the Youden index (sensitivity+specificity –1) were calculated for each possible cut-off value. The maximum Youden index was used to select the most accurate cut-off [24]. Finally, patients with NMD were stratified according to the presence of respiratory failure defined as either established NIV or newly diagnosed daytime hypercapnia (pCO2 > 6.0 kPa) or nocturnal hypoventilation (transcutaneous pCO2 > 6.7 kPa), respectively. Based on these subgroups, SBCT cut-off values were evaluated for prediction of NIV indication.
RESULTS
Study cohort
In total, 200 participants were enrolled in the study, including 100 healthy individuals (20–77 years of age) and 100 people with NMD (20–84 years of age). In the patient subgroup, 23 subjects could only be examined in the upright position. Measurement of SNIP was unavailable in one healthy subject. Male-to-female ratio was 50 : 50 among healthy individuals and 65 : 35 among people with NMD (Table 1).
Study groups
NMD, neuromuscular disorders, SNIP, sniff nasal inspiratory pressure.
The spectrum of neuromuscular diagnoses comprised motor neuron disease (n = 48, including ALS, spinal muscular atrophy, and spinal and bulbar muscular atrophy), genetically confirmed myopathies and muscular dystrophies (n = 36), polymyositis, unclassified myopathies, Charcot Marie Tooth disease, Parsonage-Turner syndrome with bilateral phrenic nerve involvement, congenital myasthenic syndromes, and cervical radiculopathy (Table 2). Prior to volitional testing, mean score on the Borg scale was 6.0 (±0.14) in healthy adults (indicating “no exertion”) and 9.34 (±2.7) in people with NMD (reflecting “very light exertion”; p < 0.05)
Diagnostic spectrum among study participants with NMD
NMD, neuromuscular disorders. 1genetically confirmed.
Group comparisons
In healthy individuals, normal distribution was found for SBCT, FVC, FEV1, PEF and MIP in both the upright and supine position, and for supine SNIP. Thus, only upright SNIP and FVC (% predicted) were not normally distributed. Among the entire NMD cohort (n = 100), all values were non-parametric except for FVC (% predicted). In the 77 patients in whom both upright and supine measurements were available normal distribution was found for upright FVC, FVC (% predicted), FEV1, PEF and for supine FVC and FEV1.
Group comparisons were performed between study groups and, within each group, between subgroups stratified according to gender, age, and body position. In healthy subjects, SBCT and all other volitional measures were significantly higher in men than in women (Table 3). In addition, all measures were significantly higher in the upright than the supine position and, except SNIP, in younger probands (<50 years) than in older individuals (≥50 years, Table 3).
Results of SBCT and volitional tests of respiratory muscle function in healthy subjects and people with NMD (subgroups stratified according to gender, age, and body position)
Results are reported as 1mean or 2median, and, in brackets, 3standard deviation or 4interquartile range, as appropriate. Asterisks indicate p < 0.05 (one-sided) in appropriate statistical tests: 5two-sample t-test, 6paired t-test, 7Mann-Whitney U test, 8Wilcoxon ranked sign test. Non-parametric tests were used for comparison between healthy subjects and people with NMD in case of non-parametric distribution in the latter group. FVC, forced vital capacity, FEV1, forced expiratory volume in 1 second, PEF, peak expiratory flow, MIP, maximum inspiratory pressure, NMD, neuromuscular disorders, NS, not significant, SNIP, sniff nasal inspiratory pressure. *p < 0.05 (one-sided), #, SNIP values were available for 99 healthy subjects (upright and supine), 100 patients (upright) and 77 patients (supine), respectively.
In the patient group, male individuals achieved significantly higher median values for SBCT, FVC, FEV1, PEF, MIP, and SNIP than female subjects (Table 3). Regarding all measures, median values were also significantly higher in the upright as compared to the supine position (Table 3). After stratification for age (<50 vs. ≥50 years) no significant differences were found regarding both upright and supine values (data not shown). As expected, healthy subjects performed significantly better on SBCT and all volitional tests than people with NMD in both the upright and supine position (Table 3).
Intercorrelation of spirometry parameters and inspiratory pressures
In healthy subjects, FVC and FEV1 were significantly correlated with MIP and SNIP in both body positions, but strength of correlation was weak to moderate only (data not shown). In contrast, upright and supine FVC (L) were strongly correlated with the respective MIP (cm H2O) in patients with NMD (ρ= 0.77 and ρ= 0.72). Correlation coefficients between FVC (L) and SNIP in the upright and supine position were ρ= 0.67 and ρ= 0.63, respectively (all p values < 0.01). In both groups, MIP and SNIP were strongly related irrespective of body position (data not shown).
Correlation of SBCT with age, spirometry parameters and inspiratory pressures
Upright and supine SBCT showed weak inverse correlation with age in healthy individuals (Table 4). In this group, SBCT was moderately correlated with FVC and FEV1 but only weakly with PEF, MIP, and supine SNIP (Table 4).
Correlation of the SBCT with age and volitional tests of respiratory muscle function
ρ= Spearman’s correlation coefficient, r = Pearson’s correlation coefficient, *p < 0.05 (one-sided), **p < 0.01 (one-sided). FVC, forced vital capacity, FEV1, forced expiratory volume in 1 second, PEF, peak expiratory flow, MIP, maximum inspiratory pressure, NMD, neuromuscular disorders, SNIP, sniff nasal inspiratory pressure.
In people with NMD, upright and supine SBCT were not correlated with age, but correlation with spirometry and inspiratory pressures was markedly stronger than in healthy subjects (Table 4). Furthermore, people with NMD and inspiratory muscle weakness as defined by MIP < 60 cmH2O showed stronger correlation of SBCT scores with FEV1, PEF, MIP, and SNIP than patients in whom MIP exceeded 60 cm H2O (Supplemental table 1).
Regarding strength of correlation with spirometry, MIP and SNIP values, supine SBCT was only marginally superior to upright testing (Table 4).
Linear and logarithmic regression analysis
Univariable linear and logarithmic regression was performed in healthy subjects and patients with NMD for both FVC and MIP on SBCT in the upright position (Figs. 1 and 2). In healthy subjects the SBCT accounted for 23.7% of FVC variance and 4.5% of MIP variance (logarithmic model). In people with NMD, the SBCT accounted for 44.5% of FVC variance and 37.7% of MIP variance (logarithmic model).
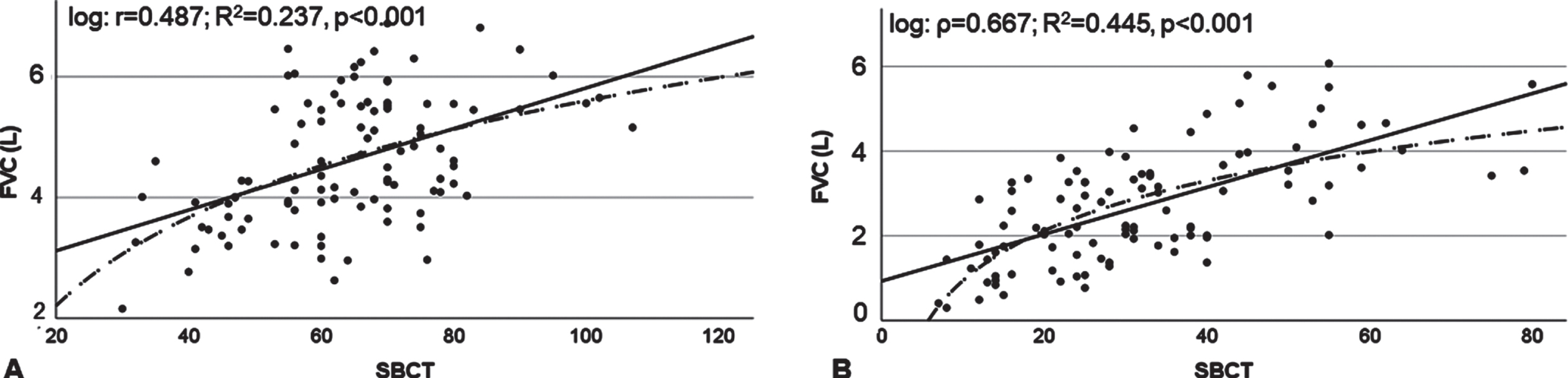
Linear and logarithmic regression of upright FVC on upright SBCT in healthy subjects (Panel A) and people with NMD (Panel B). FVC, forced vital capacity, NMD, neuromuscular disorders. Solid line, linear regression curve, dotted line, logarithmic regression curve.
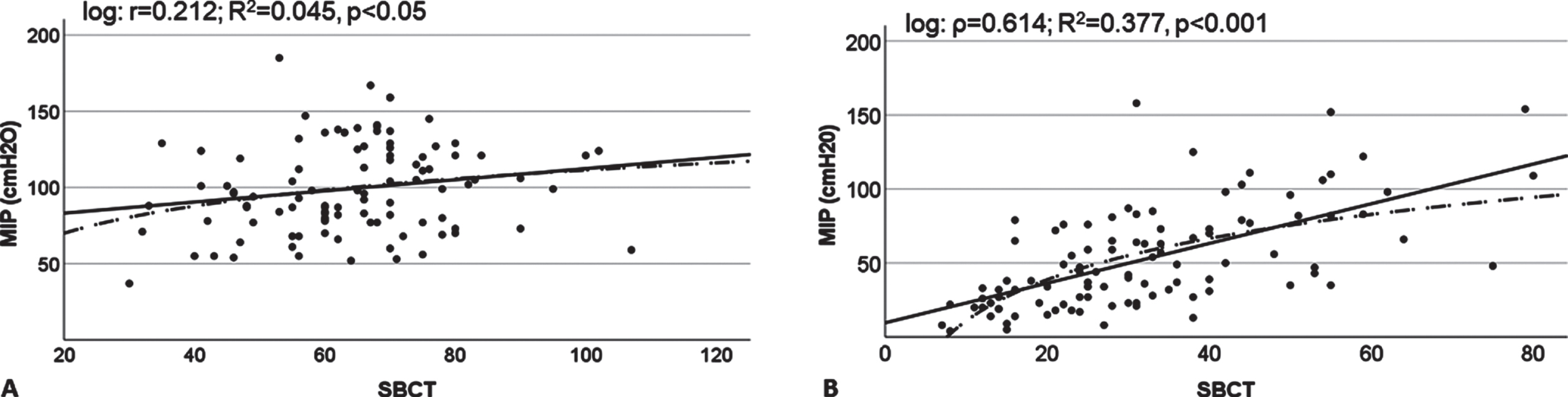
Linear and logarithmic regression of upright MIP on upright SBCT in healthy subjects (Panel A) and people with NMD (Panel B). MIP, maximum inspiratory pressure, NMD, neuromuscular disorders. Solid line, linear regression curve, dotted line, logarithmic regression curve.
Receiver operating characteristics (ROC)
ROC analyses were performed in people with NMD and for upright values only (Fig. 3). SBCT values < 41 indicated lung restriction (sensitivity 0.89, specificity 0.62, area under the curve (AUC) 0.80), and SBCT values < 27 predicted inspiratory muscle weakness (sensitivity 0.61, specificity 0.86, AUC 0.79). Subsequently, ROC analyses were performed to identify thresholds for SBCT and FVC (% predicted) that indicated the need for NIV. The latter was predicted by SBCT < 39 (sensitivity 0.92, specificity 0.46, AUC 0.70, Fig. 3C) or FVC < 68.5% (sensitivity 0.85, specificity 0.62, AUC 0.75, figure not shown). In a two-step approach, cross-tabulation for FVC < 68.5% was confined to patients with SBCT < 39, leading to a further increase of sensitivity to 0.91 (specificity 0.54, AUC 0.70).
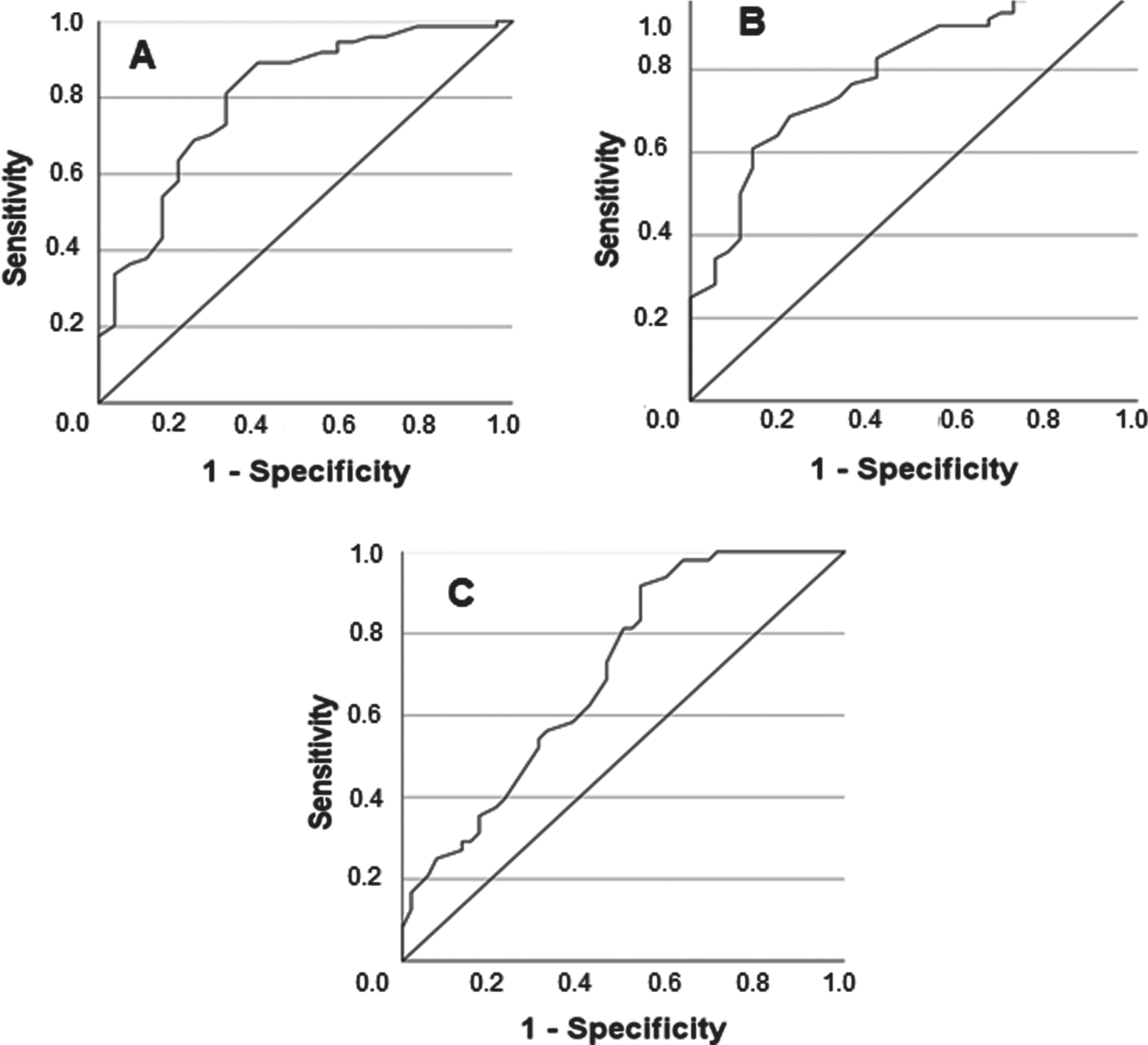
Receiver-operating characteristics (ROC) analysis of different SBCT cut-off values (upright) for prediction of lung restriction (FVC < 80% predicted, Panel A), inspiratory muscle weakness (MIP < 60 cmH2O, Panel B), or NIV indication (as defined by sleep-related hypoventilation or chronic hypercapnic respiratory failure, Panel C) in people with NMD. For further detail, see text.
DISCUSSION
Study design
Apart from its sheer sample size this study goes beyond previous work in several aspects: Firstly, SBCT was validated against spirometric parameters in conjunction with both MIP and SNIP which are direct measures of inspiratory muscle strength [20, 22]. Secondly, validation was performed in people with NMD and, for the first time, in healthy individuals. Thirdly, all tests were performed in the upright and supine position, the latter being known to potentially unmask diaphragm weakness [25]. Fourthly, validation of the SBCT in healthy subjects was specifically designed to account for gender and age. Fifthly, people with a wide range of different NMD were enrolled to assess test validity for a broader spectrum of conditions. Finally, predictability of lung restriction, inspiratory muscle weakness and NIV indication by distinct SBCT thresholds was investigated.
Validation of the SBCT
The present study showed that standardized conduction of the SBCT is feasible in both healthy individuals and subjects with different NMD. Plausibility of the SBCT as a measure of inspiratory capacity is evident from the fact that it meets basic physiological expectations: In both groups, significantly higher SBCT values were achieved in the upright than in the supine position, and male participants generally scored higher than women. Furthermore, among healthy subjects SBCT values were higher in younger than in older individuals. These results were expectable as lung size is larger in men and decreases with age [19]. In addition, lung capacity is physiologically higher in the upright than the supine position as auxiliary respiratory muscles can be recruited more effectively [25]. Moreover, it is plausible that in people with NMD, spirometry measures, inspiratory pressures and SBCT scores were markedly lower than in healthy subjects. Finally, robustness of data and validity of the SBCT are reflected by the fact that SBCT values were significantly correlated with FVC and FEV1 in both the upright and supine position. This holds true for both people with NMD and healthy subjects. Interestingly, it could be shown that statistical correlation of the SBCT with FVC, FEV1 and, of note, also PEF is substantially stronger in NMD patients than in healthy subjects. Moreover, the SBCT statistically relates to MIP and SNIP in people with NMD only. Thus, the SBCT parallels other volitional measures of respiratory muscle function in both health and disease. In patients with NMD, this association is particularly close and becomes even closer in subjects with reduced inspiratory muscle strength, irrespective of body position. Of note, data analysis showed that statistical correlation of the SBCT with other volitional tests was only slightly stronger for supine than for upright measurements, rendering the upright test sufficiently valid.
Previous studies that applied the SBCT had several limitations. In healthy subjects, the SBCT has been studied only once in terms of feasibility but without validation against spirometry [26]. Studies validating the SBCT in patients with NMD were conducted with small sample size and a limited spectrum of conditions only [10, 27]. Validation of the SBCT was mainly performed against FVC (upright), yielding correlation coefficients like those observed in the present work. In patients with pulmonary disease, the SBCT has been validated against FVC, FEV1, and PEF, with moderate correlation in clinically stable patients with obstructive or restrictive conditions [10, 11]. One study in adult patients with chronic obstructive pulmonary disease showed that SBCT and PEF are strongly related if acute exacerbation is present [28]. This corresponds to the present study’s finding that statistical association of the SBCT with volitional measures of respiratory performance was stronger in patients with NMD than in healthy subjects and even stronger in case of respiratory muscle weakness. Maximum SBCT is likely to be impaired in subjects with either lung restriction or severe airway obstruction that both reduce the volume that can be inhaled by taking one breath. Thus, the SBCT may better reflect inspiratory capacity in diseased people than in healthy individuals because respiratory impairment is present. This notion is supported by the fact that regression analysis of SBCT on either FVC or MIP revealed higher determination coefficients for NMD patients than for healthy subjects (see online supplemental material). In addition, maximum SBCT was closely related to MIP and SNIP in people with NMD only (Fig. 2B). As correlation of SBCT with MIP, SNIP and spirometry parameters was strongest in study participants with MIP < 60 cm H2O, external validity of the SBCT is apparently better if respiratory muscle weakness is already present, likely increasing test reliability. Furthermore, the SBCT might be especially helpful for remote monitoring and in patients unable to execute spirometry or inspiratory pressure testing. Construct validity of the SBCT is underlined by its strong association with both of these measures which showed, at the same time, close relation to each other as previously described in ALS [29]. However, MIP and SNIP should be considered complementary rather than exchangeable due to variable limits of agreement and different feasibility in certain clinical situations (e. g. children, weakness of mouth closure) [30].
Predictive value of the SBCT
The predictive value of the SBCT has only been addressed in a single study on patients with ALS [13], using a 50% -threshold for FVC% predicted that defines severe lung restriction or indication for NIV according to US Medicare criteria, respectively. However, this threshold may be much too low for patients with rapid disease progression as early initiation of NIV is associated with longer survival [31]. For other NMD than ALS, no studies exist that specifically focus on the predictive value of the SBCT. In contrast, predictability of NIV indication by FVC, MIP and SNIP has been investigated in several conditions [32–35].
The present study shows that SBCT thresholds can be identified which allow for prediction of lung restriction, inspiratory muscle weakness, or NIV indication. Using this study’s protocol SBCT cut-off scores are < 41 for FVC < 80% predicted,<27 for MIP < 60 cmH2O, and < 39 for NIV indication. Of note, in most study participants receiving home ventilatory support indication for NIV had been based on nocturnal hypercapnia which is probably more sensitive than any other test [36, 37]. Prediction of MIP < 60 cm H2O by a SBCT score < 27 is of little help as sensitivity is rather low and indication for NIV can already be suspected with higher scores. Furthermore, this MIP threshold (also derived from the US Medicare criteria for NIV indication) is somewhat arbitrary, denies the anthropometrical range of normal [22] and likely indicates inspiratory muscle weakness that is already severe. Cut-off scores of the SBCT for prediction of either lung restriction (<41) or NIV indication (<39) are much more sensitive than the < 27 threshold that is indicative of inspiratory muscle weakness. Based on test accuracy, it seems reasonable to primarily use the < 41 SBCT threshold for identification of patients with probable lung restriction in whom further investigation is required. General suitability of the SBCT is underlined by the fact that for prediction of NIV indication, the < 39 SBCT threshold was not inferior to the optimal cut-off for FVC which was found to be < 68.5%.
As the SBCT requires only little equipment it may be applied by general practitioners or non-specialized neurologists for initial assessment of respiratory function in people with NMD. If patients are capable to score≥41 on the SBCT and symptoms of respiratory muscle weakness or sleep-disordered breathing are absent (e. g., dyspnea, orthopnea, or sleep complaints), inspiratory capacity is probably sufficient to warrant nocturnal normoventilation. In subjects incapable to count to 41, further diagnostic work-up should be initiated, comprising spirometry, MIP/SNIP testing, and, eventually, diagnostic sleep studies along with overnight capnometry.
Study limitations
Despite its comprehensive design the present study has several limitations. Firstly, there is no correction factor for the SBCT adjusting for gender, age, and height. The study showed that healthy probands, females and older individuals achieved lower SBCT scores than males and younger subjects, likely reflecting the impact of lung size. Cut-off values for prediction of lung restriction or NIV indication were identified by statistical means irrespective of anthropometric aspects. Thus, SBCT thresholds must be considered as approximations with limited specificity until normative values become available that account for gender, age, and height as applicable for FVC and MIP [19, 22]. However, the predictive value of the SBCT for lung restriction is not affected by this shortcoming as FVC (% predicted) already accounts for anatomical differences. [19, 22].
Secondly, predictability of NIV indication by the < 39 SBCT threshold is limited by the fact that patients with established NIV and subjects with newly diagnosed hypercapnia were combined in one subgroup. Thus, NMD patients with long-standing NIV and severe weakness of the respiratory muscles might have led to underestimation of the cut-off value. Moreover, the SBCT score at the onset of hypoventilation was unknown for patients already receiving NIV, which likely narrows validity of study results regarding screening purposes. These shortcomings could be addressed in a study that applies SBCT and diagnostic capnometry only in patients in whom NIV has not yet been established.
Thirdly, more than half of the study participants (74 healthy subjects and 61 people with NMD) showed a learning effect reflected by increasing SBCT scores from the first through the third attempt. However, the same is likely to apply to other volitional measures as previously shown for MIP [38]. Fourthly, the number of test repetitions was limited, and variability of results might have been lower with more attempts [8]. However, this study was designed to apply a test protocol that is both standardized and manageable in clinical routine. Fifthly, it may be considered a limitation that SNIP was measured from RV rather than FRC as originally described [20]. This approach was chosen to facilitate comparison of SNIP and MIP values. Lastly, the SBCT might be difficult or impossible to perform for patients with severe dysarthria who were excluded in the current study.
Conclusion
The SBCT is a simple bedside test that allows for assessment of global lung function and inspiratory muscle strength in both healthy subjects and people with NMD. It is sufficiently valid when compared to spirometry and inspiratory pressure measurement and may be useful to predict lung restriction and even indication for NIV. It can easily be performed without advanced equipment and allows for remote monitoring, e. g. during phone calls or video appointments. The SBCT may increase awareness for respiratory muscle involvement in patients with NMD and helps to identify patients in whom further diagnostic work-up is required.
Footnotes
ACKNOWLEDGMENTS
The authors are grateful to Mr Dan Pieper for supporting patient recruitment.
FUNDING
This study was supported by the Deutsche Gesellschaft für Muskelkranke (DGM) e. V., Freiburg, Germany.
CONFLICTS OF INTEREST
All authors declare no conflicts of interest.