
Abstract
Background:
Progressive equinovarus deformities are common in people with Duchenne Muscular Dystrophy (DMD); they may provoke pain, pressure spots, cause problems with wearing footwear, and may lead to an unstable sitting position.
Objective:
Explore indications and compare complications and long-term outcomes after soft tissue and osseous interventions in people with DMD.
Methods:
Retrospective, monocenter, longitudinal study. Data on indications, equinus and varus deformity before and after surgery, wound healing problems, ‘pain’, edema, and long-term outcomes were collected from medical files. Soft tissue interventions were compared with osseous interventions.
Results:
From a series of 18 patients, data on 32 surgical interventions and 169 follow-up visits were analyzed. ‘Footrest placement’ was the most frequent surgical indication, followed by pain. Osseous interventions were performed in older patients with rigid deformities. Directly after surgery remaining deformities were reported after soft tissue interventions (18 %), no remaining deformities were reported after osseous interventions. Pain and edema were frequently present, especially after osseous surgery. Longitudinal follow-up showed that surgical interventions could lead to a neutral foot for a for more than 3 years on average years. Relapses of foot deformity occurred, especially the recurrence of varus deformity after osseous interventions.
Conclusions:
Surgical interventions can successfully lead to a neutral foot position for for more than 3 years on average. Soft tissue interventions appear to be superior to osseous corrections, considering the varus recurrence period and complications, and may be considered when feet are still (partly) correctable. Pain management and edema prevention should be anticipated before surgery. Future research on patient reported outcomes as well as evaluating the outcome of the initial indication is needed to further identify benefits.
Keywords
INTRODUCTION
Duchenne muscular dystrophy (DMD) is a progressive X-linked neuromuscular disease that occurs in 1 in 5,000 live-born boys, resulting in muscular weakness, associated motor delays, loss of ambulation, respiratory impairment, and cardiomyopathy [1, 2]. DMD typically leads to muscle weakness of the proximal muscles in the early phases of the disease, leading to loss of ambulation around 8–14 years and more distal weakness in the latter disease stages. Early development of progressive equines and hindfoot varus deformities is common in people with DMD, which progresses upon full-time wheelchair use [3]. Without interventions, foot deformities can further progress, as illustrated in picture 1, and may cause pain and problems with support on the footrest. Literature has described before that foot deformities may provoke pain, pressure spots, problems with wearing footwear and/ or orthoses [4, 5]. Moreover, abnormal foot positioning may lead to an unstable sitting position, which increases the demand on the trunk muscles and negatively influences arm function [6, 7].
An adult person with Duchenne with equinovarus deformity who did not underwent interventions. Picture 1a: foot position at the foot rest while wearing shoes. Picture 1b: bare feet.
There is little published data on surgical interventions to improve foot shape in non- ambulatory people with DMD. Studies from the eighties and nineties focused mainly on prolongation of (braced) ambulation with use of subcutaneous (multi-level) tenotomies in combination with knee-ankle-foot-orthosis [8–11]. Although these interventions may indeed prolong the (supported) ambulatory phase, in practice the burden of these procedures and wearing knee-ankle-foot orthosis during day-time is often too high for patients to gain a short period of braced ambulation [12]. More recently, Scher et. al. [13] investigated the benefits of tenotomies in people with DMD and concluded that Achilles tendon (AT) lengthening, posterior tibial tendon transfer to the second metatarsal bone, and toe-flexor tenotomies could be indicated when difficulty in wearing shoes or foot positioning occurs in people with DMD based on interview on 30 ambulant people with DMD who underwent surgery, compared to a control group consisting of 58 people with DMD who did not underwent surgery. Leitch et. al. [3] also found less equinus deformities after soft tissue interventions in thirty non- ambulant people with DMD compared to the control group, however, no significant differences were seen concerning pain, wearing footwear, cosmetic concerns and satisfaction within a mean follow-up period of 6 years. In this study, the positioning on the foot rest was not evaluated, which is an important topic as described above.
Soft tissue interventions alone do not always provide adequate correction. In such cases, osseous procedures, such as a talectomy, may be needed to provide adequate correction, and diple and triple arthrodesis has been used for severe deformities in the mature foot in patients with cerebral palsy [14]. No previous study has investigated osseous interventions to regain a plantar foot position in people with DMD, although such interventions are described as a valuable alternative to improve foot shape in other neurological conditions in which rigid equinovarus deformity can occur, such as arthrogryposis, cerebral palsy, and spina bifida [14, 15]. Recent care guidelines for people with DMD [16] leave room for consideration of orthopedic interventions for foot deformities, balancing the risks of surgical interventions in general for this vulnerable population versus the benefits of these interventions.
Currently, as there is no reported evidence on balancing risk and benefits of foot surgeries in people with DMD, we performed this study, which evaluates the soft tissue and osseous surgical interventions which were performed on people with DMD in the neuromuscular center of the Radboudumc in Nijmegen, The Netherlands. This study aims to explore the indications and compare outcomes of different types of surgical interventions which were performed in people with DMD.
MATERIALS AND METHODS
This exploratory, retrospective cohort study was conducted at the neuromuscular center of the Radboudumc in Nijmegen, The Netherlands, where more than 120 people with DMD are seen annually. Retrospective data was collected on people in which DMD was confirmed genetically and/or by muscle biopsy, when they underwent surgery to correct foot deformities between 2012 and 2019, and when data of at least one follow-up visit was available in the centers’ database. The study was approved by the medical ethical committee of the Radboudumc (2019-5760).
Outcome measurements
The following pre-operative patient characteristics were collected: age at time of surgery, corticosteroid use, and splint use. Data on equinus deformity and varus deformity was collected for both sides. Equinus deformity was expressed by degrees of dorsal flexion limitation. The rigidity of the feet was expressed as whether the foot was correctable yes or no (partly correctable is also yes). Correctable means that the foot could be manual re-positioned during physical examination. Data on indication was collected, categorized as “pain”, “foot placement on foot rest”, “shoe wearing difficulties”, “orthoses wearing difficulties”, “pressure spots”, and “standing and transfer difficulties”.
Surgical procedures data were collected from the surgical reports; for analyses, we categorized the interventions as “soft tissue interventions” or “osseous interventions”. If both soft tissue and osseous interventions were performed during one procedure, we categorized this as an osseous intervention. First was noted if the intervention could correct the full foot deformity, or if a remaining deformity was present within one day after surgery. Then, the outcomes measured during follow up visits, were expressed as (1) recurrence of equinus deformity > 0 degrees, and (2) recurrence of varus deformity (yes/ no). Placement on the footrest was reported as adequate when the feet soles had complete contact with the footrest and supported the seating position. Complications - problems with wound healing, pain, edema - were assessed during follow-up (presence, yes/no). If any other complications or adverse events were reported, and if there was contributing qualitative information described in the medical records, this was also collected. Data was collected anonymously using CastorEDC (v42.41).
Statistical analysis
Explorative descriptive analysis was conducted, using SPSS (IBM SPSS Statistics for iOS, version 26, IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize patient characteristics and prevalence levels for each subgroup. Medians and ranges were used for continuous variables which were not normally distributed; means and standard deviations were used for continuous variables which were normally distributed. Frequencies (percentages) were used for categorical variables. The Mann- Whitney U test was used to explore the differences of continuous variables between groups, and the Chi square was used to determine the differences of dichotomous variables between groups. The significance level for two-tailed correlations was set at p≤0.05. Explorative longitudinal analysis, included Kaplan Meier curves and Log Rank comparisons, to explore the different trends in effect and complication-duration after the different surgical interventions. In case of a bilateral surgery, only one foot was included in those analyses, as the results in one patient are paired. In case there was a difference in outcome of the two feet, the timing of the first event was chosen.
RESULTS
Base line characteristics
In total, 32 surgical interventions in 18 patients were analyzed, all patients were non-ambulant. One patient needed surgical interventions at two different time points; he had a soft tissue intervention on the right foot and four years later a soft tissue intervention on both feet (which was reported as recurrence). Bilateral surgical interventions were most common; the 4 patients who underwent a unilateral intervention had an equinus deformity difference greater than 15 degrees between the left and right foot.
Patient characteristics at time of surgery showed that 13 patients were in the soft tissue intervention group, with a median age of 11.6 (range 8.8–15.5). The other 5 patients were in the osseous intervention group, with a median age of 16.2 (range 11.8–16.9), the age difference between both groups was significant (p = 0.046). Besides, the deformities in patients in the osseous intervention group were not correctable in the majority of the cases (see Table 1). One patient who underwent soft tissue interventions on both sides was able to perform standing transfers before surgery and lost this ability directly after surgery, which we see as an adverse event. Corticosteroid use was comparable in both groups (around 80%) and there was no significant difference in splint use between both groups. The median follow-up after surgery was 44.9 months, with a range from 9–84.8 months.
Patient characteristics at the moment of surgery (n = 18)
*Mann Whitney U/ Chi-square test between soft tissue- and osseous interventions p < 0.05;
** y = ‘yes’.
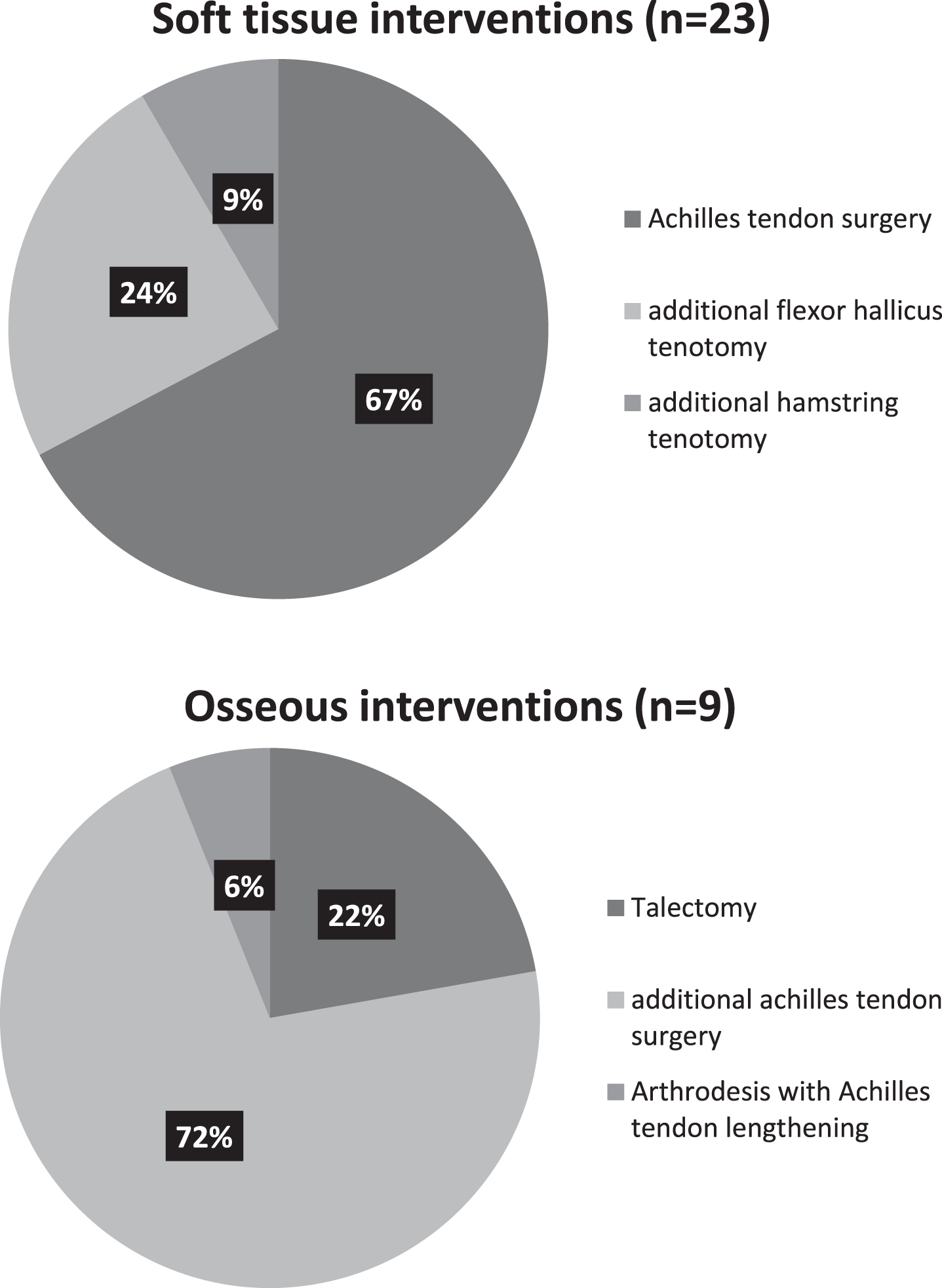
As shown in Table 2, foot placement on the wheelchair footrest was the most frequent indication for surgery (36%), otherwise pain (24%) and/ or difficulties fitting shoes (21%) are frequent indications. Figure 1 displays the overview of all surgical procedures; (percutaneous) Achilles tenotomy was the most performed soft tissue intervention (67 %), talectomy in combination with achilles tenotomy was the most performed osseous intervention (72%). Additional hamstring tenotomy was done in one patient at both sides, to improve knee extension range and increase sitting tolerance. Postoperative effects directly after surgery are displayed in Fig. 2; rest deformity was only seen after soft tissue interventions. Pain and edema occurred in respectively 64 and 30 % of all operated feet directly after surgery. Pain was more prevalent in the group who underwent osseous interventions (80 vs 46%). Problems with wound healing were not reported in our study population.
Surgical indications*
* indications were often reported for both feet if bilateral surgery was indicated. Multiple answers were possible; one patient could have two indications for a surgical intervention.
Surgical interventions.
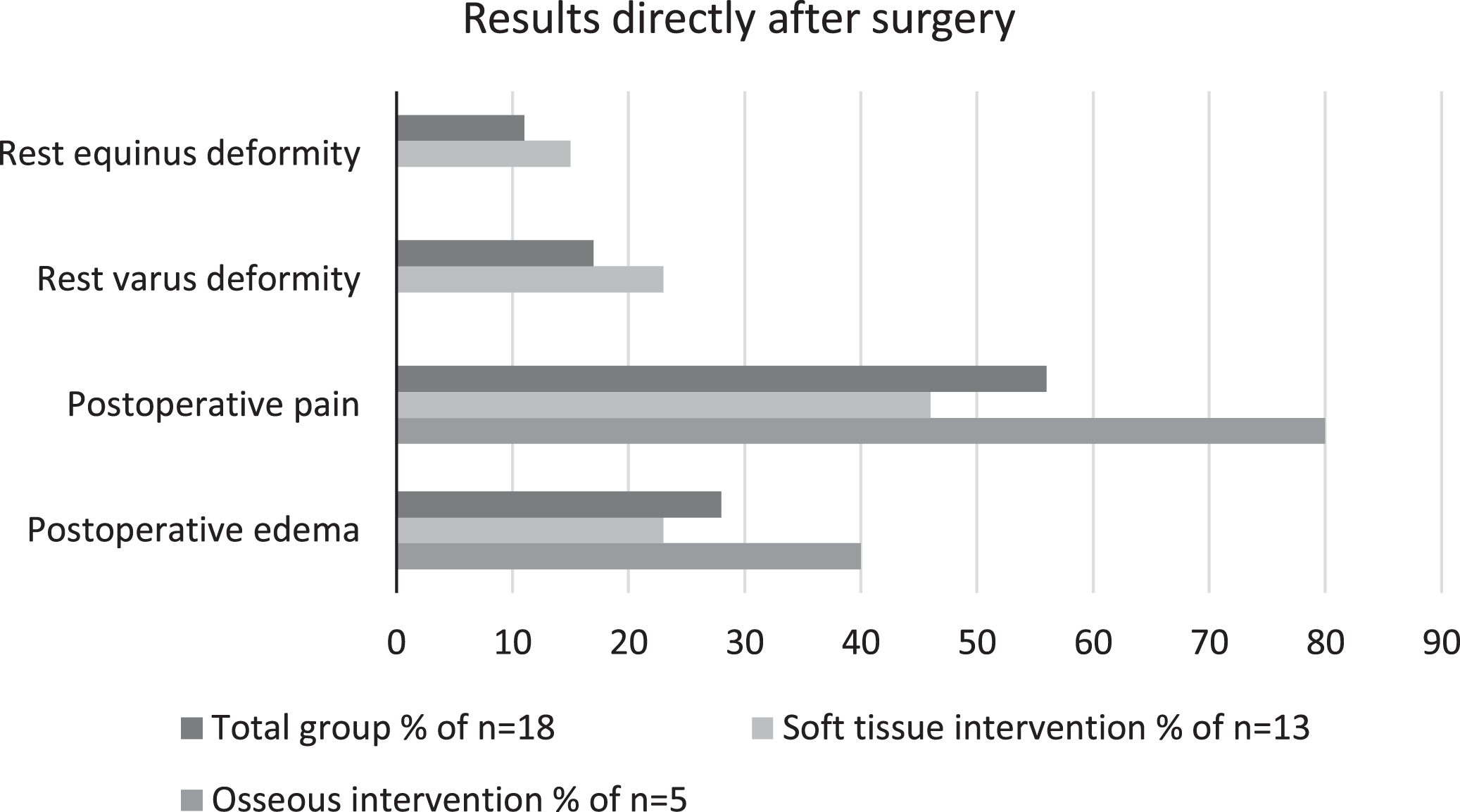
Results directly after surgery, within one day.
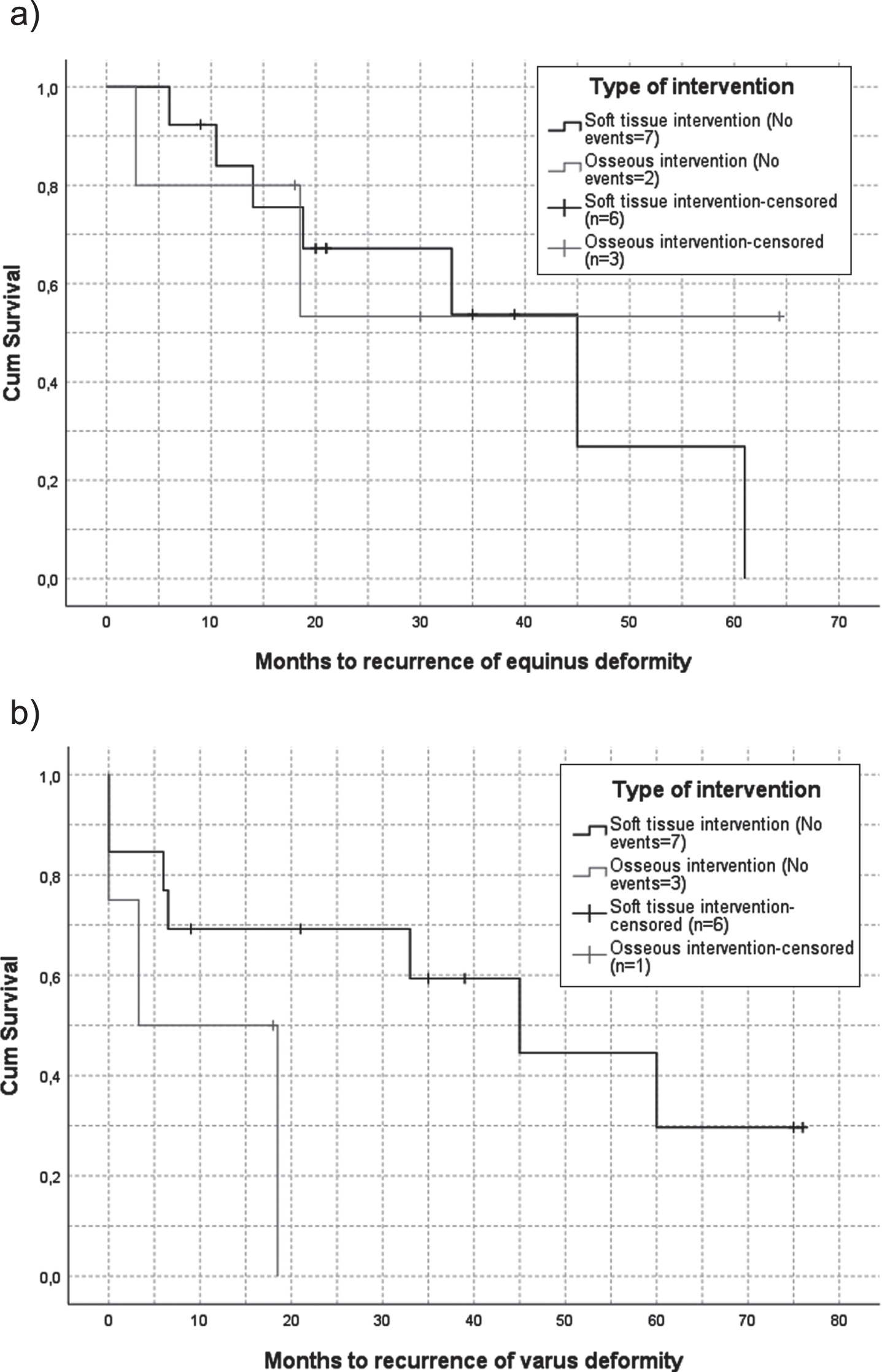
Data of 169 visits after 32 surgical procedures were analyzed (mean of 5.2 visits per procedure). Fifty per cent of the patients still had an ankle dorsal flexion of > 0 degrees 45 months after soft tissue intervention, and not reached after 70 months in the osseous intervention group (Fig. 3a). Varus deformity tended to recurrence earlier in the osseous intervention group as seen in Fig. 3b; the time point at which 50% had a recurrence in varus deformity was 3.3 months for osseous intervention and 45 months after soft tissue interventions. For the osseous interventions; one patient underwent a bilateral arthrodesis, and showed a slight recurrence in varus deformity unilaterally after 3.5 months. The log rank test showed no significant differences between the interventions groups.
Kaplan Meier survival curves of recurrent foot deformity for soft tissue –or/ and osseous interventions. Event is recurrence of equinus deformity (log rank p 0.705) (a) and recurrence of varus deformity (log rank p 0.101) (b).
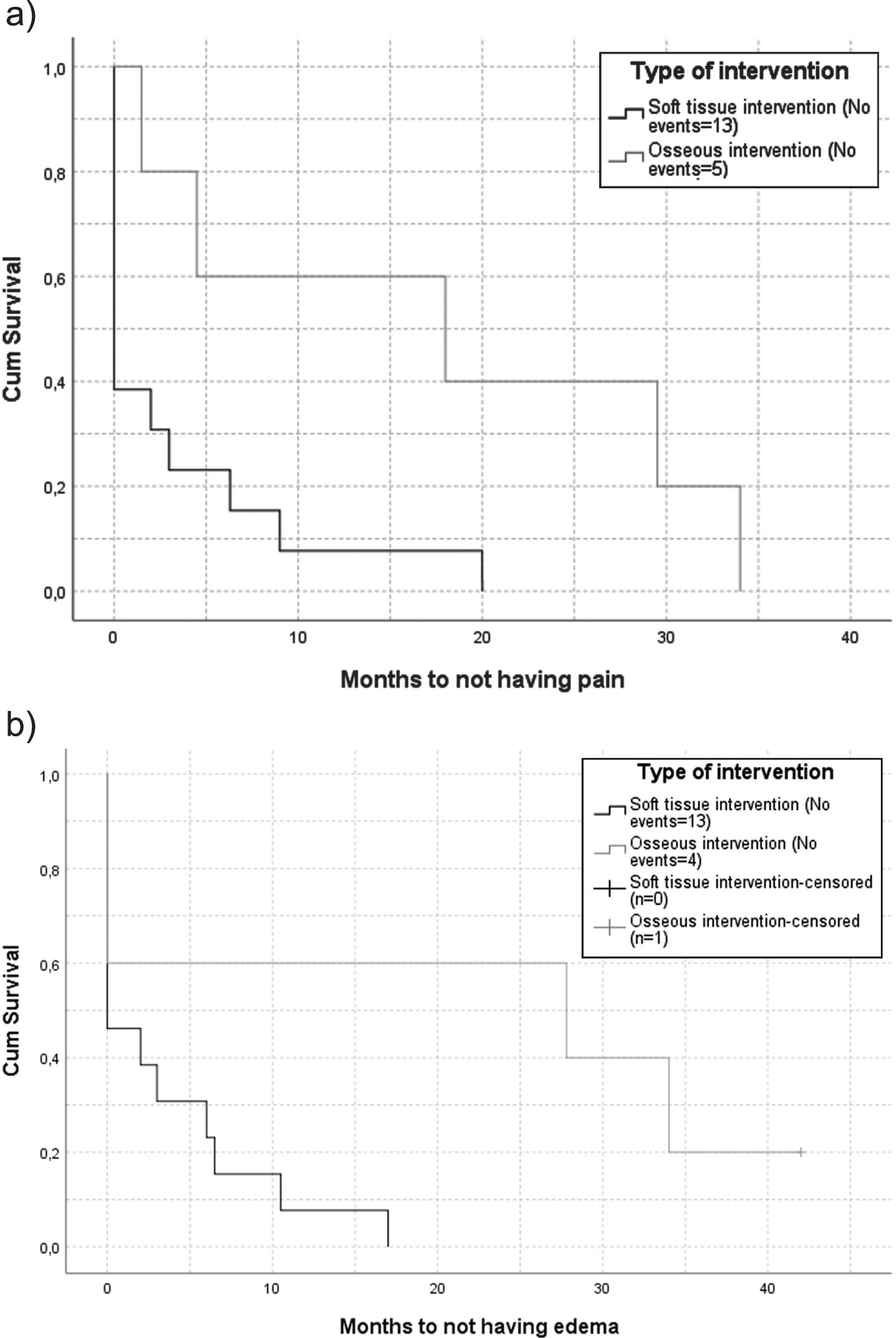
Longitudinal data on the complications pain and edema in the first six months after surgery are presented in Fig. 4. Figure 4a. displays the reported pain, and shows that over 50% of the patients did not report pain directly after surgery and none of them experienced pain 20 months after surgery in the soft tissue intervention group. In the osseous intervention group 50% of the patients still experienced pain 18 months after surgery. For edema (Fig. 4b) 50% of the patients, still reported edema after 27.8 months after an osseous intervention, while less than 50% initially reported edema after soft tissue interventions. None of the patients in the soft tissue intervention group had edema after 17 months. The log rank test showed significant differences between the different intervention groups, respectively p 0.026 and p 0.022.

Kaplan Meier survival curves of duration of postsurgical pain and edema. Event is (a) absence of pain (log rank p 0.026) and (b) absence of edema (log rank p 0.022).
Additional qualitative information from the medical records showed that reported pain after more than three months is in most cases described as hypersensitivity in touching or when wearing shoes or splints. One patient in the osseous intervention group, who underwent a talectomy, showed chronic edema and needed compression stocks for the longer term.
DISCUSSION
The current retrospective study explored the indications and outcomes for soft tissue interventions and osseous interventions in non-ambulatory people with DMD to correct foot deformities. Results show that osseous interventions are mainly done in older people with more rigid deformities. Soft tissues interventions seem to have more beneficial results in the follow-up visits concerning the period of recurrence of varus deformity and on the complications pain and edema.
Foot placement, pain and fitting of shoes were the most frequent indications to perform surgical interventions; in the soft tissue group foot rest placement was the most common indication, in the osseous intervention group, pain was the most common indication.
This is the first study which includes osseous interventions to improve foot shape in non-ambulatory people with DMD. As in other neurological diseases, soft tissue interventions are not always sufficient in correcting rigid equinovarus deformity [14, 15]. In such cases osseous interventions can be performed as an alternative, when improving foot shape is indicated. Our results show, that osseous interventions are used for corrections of foot deformity and that all people regained a neutral foot shape directly after surgery. However, the occurrence of longer lasting pain and edema should also be considered.
Our longitudinal follow-up shows earlier recurrence of varus deformity, especially after osseous interventions. This may be due to the fact that osseous interventions were performed on an older group in a later stage of their disease progression. The results of the patients who underwent soft tissue interventions in the current study are in line with the recurrence in the patients who underwent soft tissue surgery in Leitch’s study [3]. Leitch additionally showed that the group without surgery has significant worse equinus deformity, suggesting that soft tissue interventions are able to improve foot position. The recurrence of foot deformity in the patients who underwent osseous interventions in the current study seems to occur more quickly than described in the patients with spina bifida and arthrogryposis. El-Sherbini et. al. [14] found a recurrence of deformity occurred in 6 of the 13 feet after talectomy during a mean follow-up of 6 years in patients with spina bifida and arthrogryposis. The difference between these patient groups may be explained by the progressive character of DMD compared to the stationary character of spina bifida and arthrogryposis. To summarize; both soft tissue and osseous interventions can regain a neutral foot shape for on average more than three years. Our data supports the choice to perform soft tissue interventions, unless this is not possible, for example in more rigid foot deformities, i.e. in people in more advanced disease stages. In these cases osseous interventions can result in a better foot position. Nonetheless, recurrence of deformity remains a frequent complication in the long term, as DMD is a progressive disease. It is important, in future research, to gain more information on the severity and practical consequences of the recurrence; e.g. what are the consequences for foot placement and wearing shoes/ orthoses?
The current study emphasizes that postoperative pain and edema appeared to be frequent complications after surgical interventions to correct foot deformity. Pain is present in all patients directly after osseous intervention, while after soft tissue interventions only half of the patients reported pain. In the long term both pain and edema last significantly longer after osseous interventions. Important to note for these curves is that the number of patients who underwent soft tissue interventions is higher, so the percentage of patients who experience pain is relatively lower compared to the patients who underwent osseous interventions. The high prevalence of pain and edema in both groups, but especially in the osseous intervention group, should make clinicians aware that adequate pre-operative anticipation (including education), and (long-lasting) postoperative pain and edema management are indispensable factors related to every surgical intervention on the feet in people with DMD. Problems with wound healing were not reported in this study, despite of the use of corticosteroids by many of them. This may be explained by the small sample, or by the cautious considerations concerning surgical interventions in our center.
We acknowledge that this study has several limitations. First, the small population limits the conclusions that can be drawn from this study. Seemingly, our neuromuscular team might be hesitant in indicating surgical interventions as only 32 surgical interventions were performed in 7 years, while over 120 people with DMD visit our neuromuscular center for annual follow-up. Because of the small group it is not possible to distinguish the effect of the different types of interventions within the soft-tissue and osseous intervention group. Besides the difference in group size, together with the age difference can be confounders in the results. For example pain and edema can be more present in general in the older patient group. Given the recurrence of the varus deformity, we hypothesize that a tibialis posterior transfer may be a valuable addition in surgical interventions of foot deformity in DMD, which could be further investigated. The second limitation is the retrospective design, which can be sensitive to errors and missing values, such as evaluation of the intervention goal and the use of orthotics. Additionally, the time frame between visits were variable, as there was a large range in follow-up periods. Finally, we were not able to include patient reported outcome measures or to evaluate if the intervention solved the problem which was addressed as indication. As illustrated in picture 1, progressive foot deformities may cause bigger problems such as pain and lack of foot support, which may subsequently lead to sitting intolerance and arm function decline. As life expectancy increases in people with DMD, such future perspectives have to be taken into account. Future prospective research with fixed time-frame visits, a standardized measurement protocol, patient reported outcome measures, and a longer follow-up period is important to learn more about surgical interventions in patient with DMD. Despite these drawbacks, we consider the results of this study as clinically meaningful and important, since little is known about indications, timing and outcomes of surgical interventions on DMD foot deformities and osseous interventions are not previously described in this population.
Based on our explorative study, no hard indications or guideline on foot surgery in DMD can be proclaimed. However, since disease progression increases the rigidity of foot deformity, it is generally known that the window for soft tissue interventions is limited. Furthermore, we feel that soft tissue interventions are preferable over osseous interventions in effect and the complications pain and edema. Therefore, we advise to consider soft tissue interventions at an earlier –non-ambulatory–phase when foot deformities are not fixed, thus still correctable by soft tissues interventions. Moreover, when considering foot surgery, we advise to be clear on the indication, expectations and complications such as pain and edema, in a shared decision setting with the boys and their parents. The increased life expectancy, long term scenarios, sitting tolerance, and arm function should be part of this consideration. Postoperative care concerning pain management and edema prevention is indispensable. Lastly, we recommend evaluation of surgical interventions in a structured way including effect of surgery, pain, edema, recurrence of foot deformity and patient reported outcomes.
DECLARATION OF INTEREST
None.
CONFLICT OF INTEREST
The authors have no conflict of interest to report