
Abstract
Background
Charcot-Marie-Tooth (CMT) neuropathies entail a large group of diseases with different gene mutation patterns, which produce heterogeneous phenotypes. Although health-related quality of life (HRQOL) is significantly impaired, a comprehensive assessment of HRQOL in CMT patients in Germany considering phenotypical heterogeneity represented a research gap.
Objective
The aim was to assess HRQOL and the satisfaction with health care in CMT patients in Germany.
Methods
CMT patients > 15 years with a genetically confirmed CMT subtype were recruited through a national CMT patient registry. HRQOL was assessed using the EQ-5D-5L questionnaire. Furthermore, subjective impairments in daily or work activities and satisfaction with health care were assessed using 4-point scales.
Results
HRQOL in CMT patients (n = 385) was impaired compared to the German population. Most patients reported problems in the dimension mobility (89.6%), pain/discomfort (89.4%) and usual activities (81.0%). Except for patients with hereditary neuropathy with liability to pressure palsy (HNPP), we found no differences in HRQOL between the CMT subtypes. 72.0%of CMT patients were satisfied with available health care services. However, patients reported to expect more CMT-specific knowledge and support as well as easier prescription and cost coverage procedures from health professionals and insurances.
Conclusions
The patient-reported outcomes in the assessed CMT cohort elucidate the need for more specific health care services that also address the heterogeneous phenotypes. Although the assessment has been limited to the German health services setting, insights may be applicable to CMT-specific care in other national settings.
Keywords
INTRODUCTION
Charcot-Marie-Tooth neuropathies (CMT) entail a group of slowly progressive hereditary motor and sensory neuropathies, with an estimated prevalence of 1:2,500 [1–3]. The genotype is heterogeneous, with the most common mutations in PMP22, MPZ, GJB1 and MFN2 genes and continuously reported novel causative genes [4–9]. This heterogeneity is also mirrored in the phenotype with clinical symptoms ranging from mild to severe impairments. Common symptoms encompass distal weakness, atrophy, sensory loss and foot deformities, e.g. pes cavus and claw toes. Typically, first signs appear in the feet and legs in childhood or later in life; the hands become affected with ongoing disease [3, 11]. Frequently associated CMT comorbidities are restless leg syndrome, fatigue or scoliosis [12]. As there is no causative therapy until now, therapeutic options are restricted to symptomatic and supportive care, e.g. analgesics, physical and occupational therapy as well as medical aids to support the impaired mobility and hand function [5, 13]. In Germany, the level and specificity of health care services for CMT patients mainly depend on the capacity of the chosen care ecosystem. Accordingly, consumption of resources range from medical aids used, physician contact frequency to supportive therapies like physiotherapy and rehabilitation measures [14].
CMT is associated with a significant impairment of health-related quality of life (HRQOL) [15–20]. HRQOL comprises a physical, mental and social dimension and is a subjective evaluation of the health status by the patient [21, 22]. Due to the heterogeneity of the disease, health status reported by CMT patients is of high interest [5, 23] and advanced assessment procedures focusing on CMT-specific symptoms have been suggested [24].
HRQOL in German CMT patients was not assessed comprehensively with a validated tool until now: One study used the SF-36 focusing on fatigue in CMT patients, but only reported the results of selected scales [25]. Another assessed HRQOL indirectly by analysing patients’ attitude toward childbearing considering the risk a child could inherit a similar disability [26].
In this study, we assessed the HRQOL in a German cohort of genetically confirmed CMT patients with the EQ-5D-5L, a validated standardised generic tool to measure HRQOL. Additionally, we compared HRQOL in CMT patients between CMT subtypes and with the German population. Furthermore, disease-associated factors influencing HRQOL were determined and satisfaction with health care services by CMT patients was recorded.
MATERIALS AND METHODS
A cross-sectional study was performed in the year 2015 to assess HRQOL in a German cohort of CMT patients. We recruited patients through the national CMT patient registry (www.cmt-register.de) in Germany, which was launched in 2013 as part of the European Network of Excellence TREAT-NMD (www.treat-nmd.eu). Patients were eligible to take part in the study aged > 15 with a genetically confirmed diagnosis of CMT. 622 registered CMT patients met the inclusion criteria.
Subjective impairments in daily activities as well as impact on working life according to time, physical or mental condition, in mobility or flexibility, and in the social dimension were assessed on a 4-point scale.
HRQOL was measured with a German version of the EuroQol five-dimension questionnaire (EQ-5D™ is a trade mark of the Stichting EuroQol Research Foundation) to enable comparability. We used the version EQ-5D-5L and asked patients to rate their current problems in five dimensions (mobility, self-care, usual activity, pain/discomfort, anxiety/depression) on a 5-point scale. With this information a total of 3,125 (55) possible health states are described. Additionally, a visual analogue scale (EQ-5D VAS) ranging from 0 (worst) to 100 (best state) is deployed for health status assessment [27]. Each EQ-5D health state corresponds to a country-specific single index value (EQ-5D index) reflecting the societal utility or preference-based value estimated by the general population [27]. According to the value sets from Germany, the EQ-5D index ranges from –0.661 (worst health state) to 1 (best health state) [28].
In addition, we asked for the satisfaction of health care services on a 4-point scale and collected suggestions for improvement in a free text format. Our questionnaire captured sociodemographic and disease-specific aspects. Patients were asked for known comorbidities and performed surgeries associated with their CMT in a free text format. The educational level of the patients was classified according to the International Standard Classification of Education [29] and summarized as low, middle, or high. Patients could choose between a paper- and a web-based version of the questionnaire. Information about the CMT severity were gathered via the CMT-Neuropathy Score second version (CMTNS2) [30, 31], genetic findings and diagnoses were used as assigned in the registry.
The informed consent to participate was confirmed by patients prior to the study implementation. Ethical approval was obtained from the ethics committee of the Ludwig-Maximilians-University of Munich.
Differences in HRQOL measured by the EQ-5D-5L VAS between CMT patients and the German reference population [32] were analysed by t-test. To determine differences in HRQOL between subgroups regarding sociodemographic and disease-specific factors, we first used the Kolmogorov-Smirnov test to check for normal distribution followed by t-test, Mann-Whitney U test, Kruskal-Wallis test or one-way ANOVA as appropriate. Additionally, we analysed correlations between metric patients’ characteristics and HRQOL with Spearman’s ρ. A p <0.05 was used as significance level. We used IBM® SPSS® Statistics Version 25 for statistical analyses.
RESULTS
Patient characteristics
Finally, 464 patients aged > 15 answered the questionnaire (74.6 %). Of these, 385 (83.0 %) had a genetically confirmed diagnosis and were included in this study. 62.3 %had a genetically confirmed CMT1A subtype. Patients were 16 to 95 years old with a mean age of 47.1 years (SD: 13.4). The severity range of CMT was measured by the CMTNS2 and showed a broad distribution within the study population as well as the duration of disease as given in Table 1. Most patients could take care for themselves. However, 23 patients reported the need for permanent attendance by another person. One third of the patients lived with another CMT patient in one household. Most often, these persons were the patients’ children or their parents (58.4 %and 46.4 %, respectively).
Sociodemographic and disease-specific patient characteristics
As data were not normally distributed, median and interquartile range (IQR) are reported. Unless otherwise stated data refer to the study population of n = 385. Because of rounding, percentage might not add up to exactly 100%. 1Data of the national patient registry.
We found a high percentage of patients reporting CMT-associated comorbidities, including scoliosis (cohort prevalence of 11.4 %), foot or toe deformities (6.8 %), restless leg syndrome and hip dysplasia (4.4 %each), hearing loss (4.2 %) or sleep disorders including sleep apnoea (3.9 %). Additionally, patients reported further comorbidities like other spinal problems (25.5 %), organ dysfunctions like diabetes, thyroid or liver disease (20.8 %), cardiovascular (16.6 %) and other neurological diseases (15.6 %). One third of patients reported surgeries due to their CMT, in most cases foot corrections in general (15.8 %of patients), tendon transfers (13.5 %), osteotomy (7.8 %) or arthrodesis (6.5 %) were performed. The educational level in the population was higher compared to representative data for Germany [33]. Table 1 shows further sociodemographic and clinical features of the patients.
Subjectively evaluated impairments
92.4 %of the patients evaluated themselves as being impaired in the activities of daily living and 67.9 %reported impairments in school or work activities. This reflected physical constraints and the associated perceived limitations in mobility, flexibility and time (Fig. 1). Impairments concerning both physical and emotional status seemed to be of higher importance in school/work activities as compared to activities of daily living. The consequences are reflected in changing employment situations in 39.2 %of the CMT patients: 24.0 %of the working patients had to reduce their working times in the course of the disease, 20.6 %of the patients had to give up their occupational activities due to CMT, and 13.7 %had to change their working place or their profession to remain active.
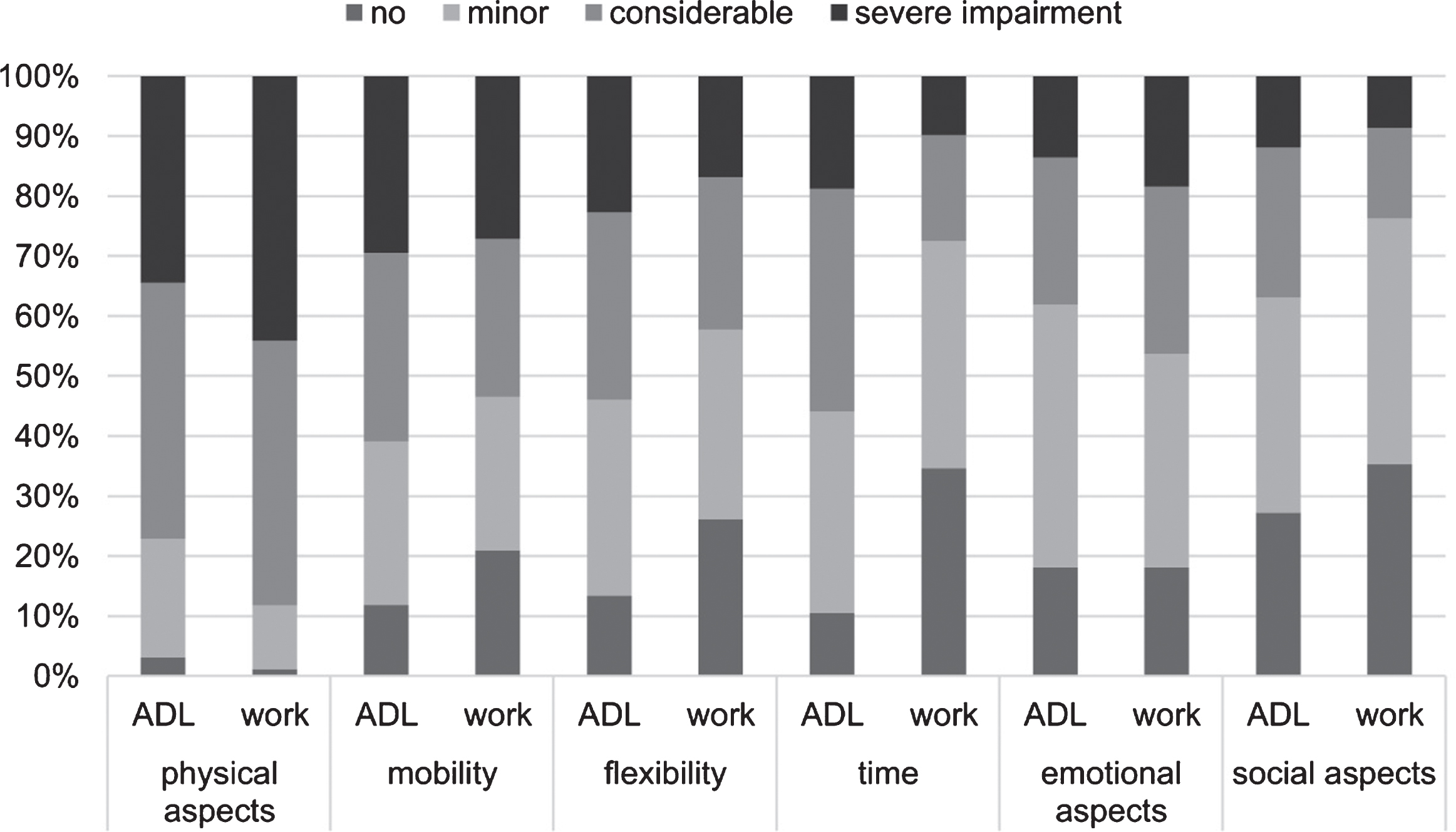
Subjectively evaluated impairments in activities of daily living and in school or work. Percentage of patients who indicated impairments in activities of daily living and school/work activities, respectively (n = 352–354 for activities of daily living and n = 243–245 for school/work activities). ADL: activities of daily living; work: school/work activities.
Quality of life
According to the EQ-5D-5L most patients reported problems in the dimension mobility (89.6 %of patients), followed by pain/discomfort (89.4 %) and usual activities (81.0 %, Fig. 2). The least problems occurred in self-care, 66.6 %of CMT patients reported no problems in this dimension. Extreme problems in the dimensions pain/discomfort (3.9 %) and mobility (3.6 %, Table 2) were quite low. Patients rated their current health status at a mean of 58.5 (SD: 19.8, median: 60, IQR: 45–75) on the EQ-5D VAS. The EQ-5D VAS rating by CMT patients was significantly lower compared to the German reference population (84.3; p < 0.001, Fig. 2). The mean EQ-5D index in CMT patients according to the societal preferences in Germany was 0.65 (SD: 0.28, median: 0.75, IQR: 0.52–0.85, Table 2).
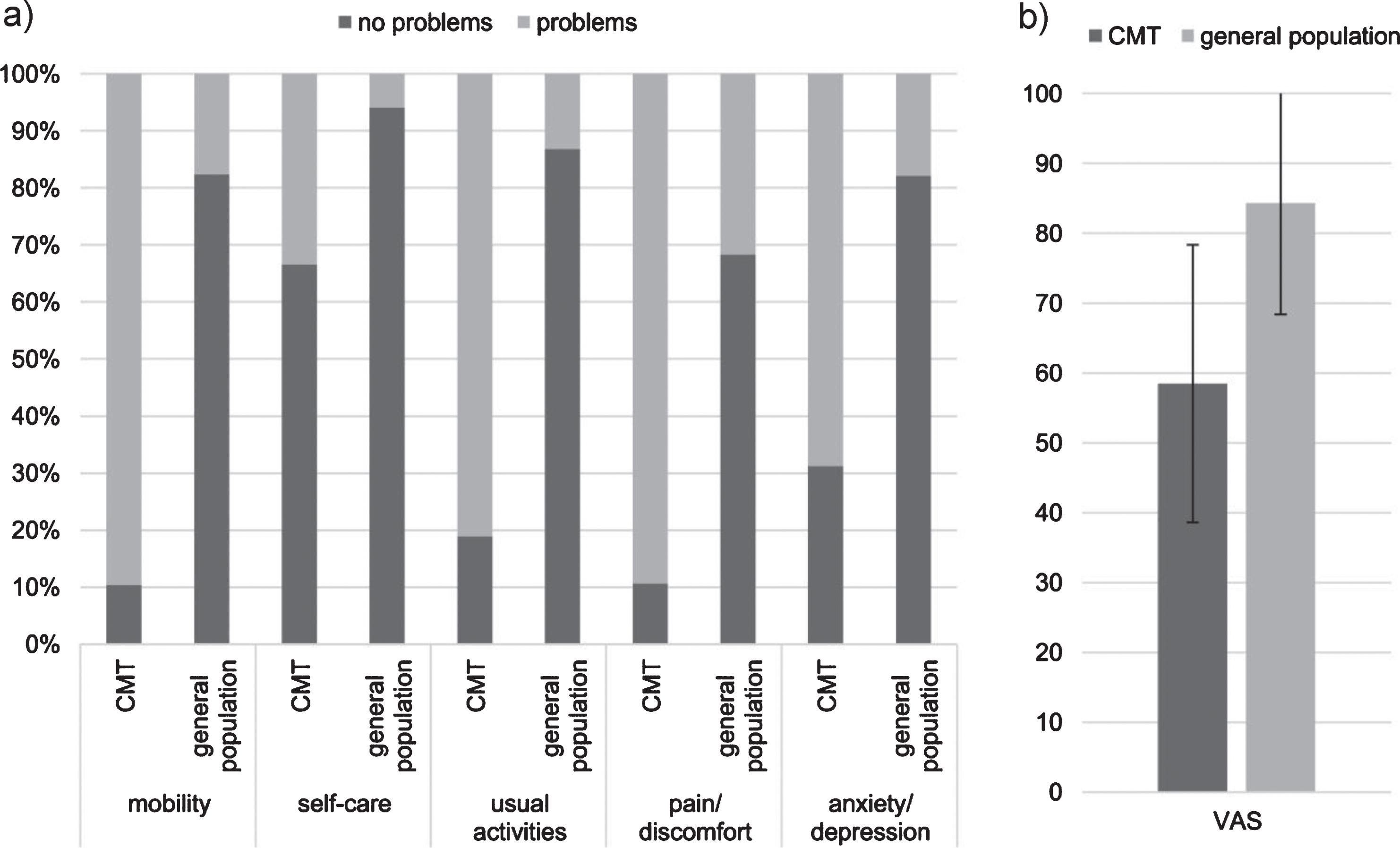
HRQOL in CMT patients and the German general population measured with the EQ-5D-5L. a) percentage of reported problems in each dimension, b) mean score of the visual analogue scale (VAS). “No problems” reflects level 1 of the EQ-5D-5L in each dimension, “problems” summarizes level 2 to 5 (slight to extreme problems). VAS: visual analogue scale (0: worst, 100: best health). For comparability purposes results of the VAS are presented as mean and standard deviation, although they were not normally distributed. Error bars indicate standard deviation. Data for the general population are based on [32].
Results of the EQ-5D-5L in CMT subtypes
As EQ-5D VAS and EQ-5D index data were not normally distributed, we present median and interquartile range. p < 0.05 indicates significant differences between subtypes (result of a Kruskal-Wallis Test). Results for other subtypes, e.g. HSANIA, HSANIC, are not displayed due to the small number of patients (n = 3).
We found gender differences in the dimension self-care reflecting a higher impairment in men, as well as in the dimension anxiety suggesting a higher impact on women (p < 0.05). EQ-5D scores were worse in patients who reported CMT-associated or other comorbidities. Patients who have undergone surgery had a lower overall HRQOL according to EQ-5D VAS and EQ-5D index and significantly more problems with mobility and daily activities compared to patients without performed surgeries (p < 0.05). In addition, patients with more problems in the EQ-5D dimensions reported themselves as being impaired in daily activities or in school or at work, others were not working or reported need for permanent attendance (p < 0.05). Single, divorced or widowed patients reported far reaching problems in the dimensions self-care and anxiety compared to married patients or patients in a partnership (p < 0.05). Differences between CMT types existed within the dimension mobility showing more extensive problems along with their impact on HRQOL for CMT types 1, 2, 4 and X as compared to hereditary neuropathy with liability to pressure palsy (HNPP) (p < 0.05, Table 2). No differences in HRQOL between sexes by CMT subtype were found with exception of more problems in the dimension self-care in male compared to female CMT1 patients (p < 0.05).
HRQOL, measured as patient-reported EQ-5D VAS and valued according to the societal preferences as EQ-5D index, declined with the severity of disease (CMTNS2, ρ= –0.38 and –0.42), age (ρ= –0.22 and –0.16), the duration of disease (ρ= –0.18 and –0.23) and higher BMI (ρ= –0.13 and –0.14), and improved with a higher educational status (ρ= 0.20 and 0.28, all p < 0.05).
Satisfaction with health care
The majority of patients were very (17.6 %) or rather (54.4 %) satisfied with health care services. Increasing satisfaction with health care was associated with higher HRQOL (ρ= 0.26 with EQ-5D VAS and 0.30 with EQ-5D index, p < 0.05). Satisfaction with health care was also associated with the scores in the EQ-5D subscales anxiety/depression (ρ= 0.35), pain/discomfort (ρ= 0.26), usual activities (ρ= 0.24) and mobility (ρ= 0.17), indicating a lower satisfaction with increasing problems in the corresponding dimensions. No association was detected in the dimension self-care (p > 0.05).
272 patients suggested improvements for health care services. Most frequently, patients referred to the lack of CMT-specific knowledge of caring health professionals and health insurances (25.7 %). Other issues involved problems with prescription, cost coverage and ineffective supportive CMT therapies including physiotherapy or occupational therapy (25.4 %). Furthermore, patients reported a general improvement need (20.2 %), need for psychological support (13.2 %), as well as general medical assistance (13.2 %).
DISCUSSION
To our knowledge, this is the first study in a German sample reporting comprehensively the HRQOL of CMT patients with a validated tool. In line with earlier studies from Germany [25, 26], we found a lower HRQOL in patients with comorbidities and a higher disease severity. Nevertheless, the association between HRQOL and
The perceived
Interestingly, we could detect differences between
Compared to the
Nevertheless, the range of standard deviation in the evaluation of the current problems in the five dimensions as well as of the current health state reveals the heterogeneity of the CMT phenotypes also from a patients’ perspective.
EQ-5D was applied in two studies analyzing the HRQOL in CMT cohorts in the United Kingdom and the Netherlands [38, 39]. Both former studies used the EQ-5D-3L, assessing the current problems in the five dimensions on a 3-point scale. In line with our results, Calvert et al. show more intense problems in CMT patients as compared to the general population, particularly in the dimensions mobility, usual activities and pain/discomfort. In contrast to the results from UK, the EQ-5D index was higher in our population (0.44 vs. 0.69) and patients reported problems with self-care less frequently. This can be explained by the slightly higher mean
Gender differences in HRQOL are also inconsistent in the published literature with deteriorated HRQOL in female CMT patients primarily in France, Italy and the USA [16, 35].
Other sociodemographic factors, e.g. the employment and family status, had also an influence on the HRQOL, in line with results from Italy, the USA and Australia, respectively [15, 19]. Factors such as BMI and educational status with a potential influence on HRQOL have been considered for the first time, although they might be important confounders in HRQOL assessments [40]. Especially the body composition seems to be a relevant indicator for the health status CMT patients, as reported recently [41]. The dimension mobility of CMT patients seems to reflect the highest relevance.
Improvements suggested by the patients regarding prescriptions and CMT-specific implementation of promising therapeutic options, e.g. physiotherapy or occupational therapies, indicate a relevant unmet need in health care provision. This emphasizes the relevance of patient-reported outcomes to identify unmet care needs, particularly those that can be solved. The perceived impairments and their impact on overall health status of CMT patients can successfully guide the search for feasible care improvements in the light of a still missing magic bullet against CMT.
The mainstay of improving the HRQOL of CMT patients is the preservation of physical functions including long-term mobility. Occupational therapy, which is used by approximately 50 %of US American and 33 %of German CMT patients [14, 42], can be an effective instrument. The reasons for not using occupational therapies were recently assessed in CMT patients. It was found that the informed physicians and therapists are pivotal for providing access to state-of-the-art treatment [42]. Suggested improvements by patients in our study cohort are accordingly indicating a lack of support, advice and information of physicians and therapists. These patients confirmed shortcomings might be explained by a lack of specific knowledge regarding existing and effective CMT care options. Accordingly, the care pathway for CMT patients need to be nourished with existing and effective interventions as well as treatment guidelines that support health professionals who do see CMT patients less frequently. Access and implementation should be measurable by using patient-reported outcomes along with HRQOL instruments.
There are some
In conclusion, our results underpin the importance of patient-reported outcomes for the advancement of CMT care pathways in a broader context. The patients’ perspective helps to identify, prioritize and better understand disease-specific factors that influence the range of CMT specific health states. The generic EQ-5D could be replaced once a disease-specific HRQOL instrument has gained international acceptance. Although the results were gathered in the German health care setting, some findings might be generalized. This include acquaintance with the heterogeneity of CMT and the full range of effective interventions among health professionals and payers, particularly as it represents a rather rare disease with its typical challenges in this regard.
Footnotes
ACKNOWLEDGMENTS
This work was supported by the Friedrich-Baur Public Trust, Burgkunstadt within the ‘Oberfranken Förderprogramm’ (Upper Frankonia Program).
The authors wish to thank the CMT patients for participating in this study, H. Saodiy, I. Hirschmann, F. Walter, C. Klug and K. Fernando Samarappuli, for scientific assistance and database research. We thank the PIs of the CMT-NET centers (Profs. B. Gess, Aachen, M. Sereda, Göttingen, P. Young, Münster) for cooperation and support.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.