
Abstract
Background:
The impacts of genetic muscle disorders on quality of life in affected children are well-documented. However, few studies have investigated children’s coping strategies and relationships between coping and quality of life.
Objectives:
To determine coping strategy use, efficacy, and associations with quality of life in children with a genetic muscle disorder.
Methods:
Forty-eight children (6–15 years, 58% male) with a genetic muscle disorder were identified as part of a national prevalence study. Children completed the Kidcope in response to a specific stressor (doctors visits) and the Pediatric Quality of Life Inventory Neuromuscular Module.
Results:
‘Wishful thinking’ (75%, 36/48) and ‘cognitive restructuring’ (71%, 34/48) were the most frequently used coping strategies. ‘Self-criticism’ (12%, 6/48), and ‘blaming others’ and ‘resignation’ (both 19%, 9/48) were the least used strategies. Coping strategy use did not differ across age and sex groups (p’s from 0.08 to 1.00). Positive coping strategies tended to be more effective (medians ranged from 2.00 to 2.75) than negative strategies (medians ranged from 1.38 to 2.50). Using a greater number of different types of positive (F(4, 46) = 5.79, p = 0.001) and/or negative (F(4, 44) = 5.64, p 0.001) coping strategies was linked to poorer health-related quality of life.
Conclusion:
We conclude that children with genetic muscle disorders use a wide range of positive and/or negative coping strategies in response to stressors associated with a doctor visit and may benefit from greater support to improve health-related quality of life. Findings support the value of routine screening of children’s coping to identify those who would benefit from support.
INTRODUCTION
Coping with the demands of childhood and adolescence can be challenging when living with a genetic muscle disorder [1], including the muscular dystrophies, congenital myopathies, and ion channel muscle disorders. Beyond physical difficulties due to severe progressive muscle wasting and weakness, affected children may face increased risks for pain, reduced life expectancy, and medical complications (cardiac, respiratory, and orthopaedic difficulties). Affected children may also experience an increase in the frequency of doctors’ visits [2], that have been described by children as disruptive to their daily commitments (i.e. school) and exhausting [3]. They are at risk of a range of psychosocial issues, including social and communication problems [4], loneliness, and a lack of empathy from others [5]. Children also report impaired health-related quality of life (HRQoL) [1, 7], which is an individual’s perception of the impact of health and illness on the physical, mental and social aspects of their life [8]. Given there are no cures for genetic muscle disorders, treatment focuses on symptom management and helping young people to cope with living with a chronic and often progressive disease [9].
‘Coping’ refers to an individual’s thoughts and behavioural efforts to handle stressors and minimise the negative effects that stressors can cause [10, 11]. These efforts may change over time and across different types of settings as individuals attempt to manage external and/or internal demands that are considered to be exceeding the resources of the person [11]. While there is on-going debate about how to classify different types of coping behaviours [12], one way is to consider coping strategies as either positive (e.g. social support) or negative (e.g. self-criticism). In general terms, positive strategies try to address the problem by managing the stressor, while negative strategies attempt to evade the stressor. It has been suggested that children who try to manage a stressor by using positive coping strategies, such as problem solving, tend to function better than those who use try to evade the stressor negative strategies, such as distraction and withdrawal [13]. However, the effectiveness of coping strategies may also depend on the characteristics of a specific stressor and a child’s ability to use coping strategies in a flexible way to support positive outcomes [14]. Prior evidence also indicates age and sex differences. Older children have been found to use a broader range of coping strategies than younger children [15], for example. There is also evidence to suggest that girls are more likely to use social support [16] and self-blame whereas boys are more likely to use problem-solving skills [17].
Coping strategies used by children and adolescents have been studied within the context of natural [18] and human-made disasters (e.g. fire, traffic accidents) [19], peer victimisation [20], and a range of health conditions, including chronic fatigue syndrome [21], and chronic illnesses [22]. However, few studies have examined coping in relation to a specific stressor associated with living with genetic muscle disorder in childhood. Most studies have focused on coping among parents, mostly of boys with Duchenne muscular dystrophy (DMD) [23–25], siblings [26], or affected adults [5, 27–30], which cannot be extrapolated to children themselves living with a genetic muscle disorder. One exception is Tesei et al’s (2020) study that examined coping strategies used by parents and children and young adults (n = 51) living with muscular dystrophies [31]. In response to experiences of ‘substantial stress’, the types of coping strategies used by children did not differ significantly from the general population with the exception of less frequent use of problem solving strategies. Health care providers for children with DMD are advised to assess children’s emotional adjustment/coping on at least an annual basis [32]. Yet, little is known about the ways that children try to cope with specific stressors associated with living with a genetic muscle disorder and whether or not their efforts are effective when dealing with health-related stressors. Coping strategy use has been linked with child HRQoL in other populations, including juvenile idiopathic arthritis [33], type 1 diabetes mellitus [34], and migraine or tension-type headache [35]. However, there does not appear to have been any previous research examining links between the coping strategy use and HRQoL outcomes in children living with a genetic muscle disorder. Identifying the most effective coping strategies and those linked to better HRQoL outcomes may help to inform/refine the design and targeted delivery of interventions to help children to manage specific stressors associated with a genetic muscle disorder.
As part of a larger study of the prevalence and impacts of genetic muscle disorders, the current study sought to extend knowledge of coping in affected children, within the context of visits to the doctor. Specific aims were to 1) identify the types of coping strategies used by children in response to a specific type of stressor associated with a genetic muscular disorder, including by age and sex groups; 2) determine the efficacy of coping strategies in response to a specific stressor; and 3) examine associations between coping strategy use and child self-reported HRQoL. Although our study is mainly exploratory it was expected, based on prior evidence [13], that those children who reported using more positive coping strategies would be characterised by better HRQoL compared with children using more negative coping strategies. Also, it was expected that older children would use different coping strategies compared to younger children given evidence of developmental progression towards more sophisticated and effective coping responses with age [36].
MATERIALS AND METHODS
Ethical approval
Approvals for the study were obtained from the Health and Disability Ethics Committee of New Zealand (Reference number: 14/NTB/118) and the Auckland University of Technology Ethics Committee (Reference number: 14/296). All study processes complied with the Helsinki Declaration of 1975.
Study population
A large, population-based, epidemiological study of prevalence and impact (MD-PREV study) sought to identify all living adults and children with genetic muscle disorders, residing in New Zealand on 01 April 2015. Based on diagnostic standards outlined by Norwood and colleagues [37], genetic muscle disorders were defined as inherited disorders that primarily affect the muscles encompassing non-dystrophic congenital myopathies and muscular dystrophies, as well as ion channel muscle diseases. Disorders of the anterior horn cell, neuromuscular junction and nerves were excluded. Multiple and overlapping sources of case ascertainment were used. These included medical record searches tailored to each District Health Board in New Zealand, using combinations of keywords and/or International Classification of Diseases and Related Health Problems (ICD-10) codes. Similar search strategies were used to check New Zealand Ministry of Health records, the New Zealand Neuromuscular Disease Registry, and Genetics Health Service databases. Advertisements to encourage self-referrals to the study and contact with relevant community support organisations also aided case ascertainment. For all potentially eligible symptomatic and asymptomatic cases, medical records (including investigations and test results) were obtained to confirm details of each diagnosis. Study eligibility was confirmed by a neurologist. Cases with insufficient evidence to confirm a diagnosis were excluded.
Children (aged < 16 years at the point prevalence date) needed to have clinical or molecular confirmation of muscular dystrophy (including Duchenne, Becker, limb-girdle, facioscapulohumeral, Emery-Dreifuss or congenital muscular dystrophy), congenital myopathy, congenital or juvenile-onset myotonic dystrophy or ion channel muscle diseases (i.e. myotonia congenita or periodic paralysis). The parents of affected children were contacted and invited to complete an impact assessment. Written informed consent was obtained from all parents. Children were also invited to participate and provided written assent, where feasible.
Study procedure
Those consenting to participate were interviewed by a trained research assistant either in-person or by telephone. Based on Lazarus and Folkman’s classic definition of coping [11], children completed the Kidcope –child version [22] which is a 15-item self-report screening tool designed for use by pediatric patients that assesses use of 10 different cognitive and behavioural coping strategies in response to a specific stressor. These include four positive and six negative strategies (Table 1). Five coping strategies (cognitive restructuring; social support; blaming others; resignation; and self-criticism) were assessed using one question. Five coping strategies (distraction; social withdrawal; problem solving; emotional regulation; and wishful thinking) were assessed using two questions, and coded as positive for use if at least one of the two questions were endorsed. Given the Kidcope invites children to report a personal problem (the stressor) within a specific situation (the setting), and then to describe their efforts at coping with that stressor (coping strateies), children were asked to think of a situation when they went to the doctor and weren’t very happy about it. Then children rated their use of each coping strategy (coded as yes or no) and, if used, the perceived efficacy (1 = Not at all, 2 = A little, or 3 = Very much) of each coping strategy.
Kidcope coping strategies
While an adolescent version (for 13 + years) is available, the child version (for 7–12 years) was used by all participants to provide comparable data across younger and older children. The pyschometric properties of the Kidcope instrument have been reported and indicate acceptable reliability, correlations with other standardised coping scales (i.e. the Coping Strategies Inventory) and proven test-retest reliability [22]. The Kidcope instrument has been used to examine coping strategies in a range of populations, including among children in New Zealand [39]. To our knowledge this is the first time that the Kidcope has been used in children and adolescents with genetic muscle disorders.
HRQoL was assessed using the child (8–12 years) report versions of the 17-item ‘About My Neuromuscular Disease’ subscale of the Pediatric Quality of Life Neuromuscular Module (PedsQL™3.0 Neuromuscular Module) [40]. The Pediatric Quality of Life Neuromuscular Module was designed to measure HRQoL dimensions specific to children ages 2 to 18 years with neuromuscular disorders. It encompasses 3 scales: 1) About My Neuromuscular Disease (17 items related to the disease process and associated symptomatology), 2) Communication (3 items related to the patient’s ability to communicate with health care providers and others about his/her illness), and 3) Family Resources (5 items related to family financial and social support systems). The ‘About My Neuromuscular Disease’ subscale was considered to be the most robust subscale and selected for use in the current analysis. Items were scored using a 5-point Likert scale to reflect difficulties with each item, ranging from 0 = never to 4 = almost always. In accordance with standard scoring instructions, each item, including reverse scoring, was rescaled on a 0 to 100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25 and 4 = 0). Scale scores are computed as the sum of the items divided by the number of items which were answered. Higher scores indicate better HRQoL.
Study specific questionnaires were used to capture children’s demographic characteristics (child age at point prevalence date recorded as part of the larger prevalence study, sex, ethnicity) and health information (diagnosis, co-morbid medical conditions).
Statistical analysis
A sensitivity analysis compared the characteristics of those children who were included in the current analysis (n = 48) to those same-aged children who were not (n = 85). For Aim 1, Cochran’s Q tests were used to determine if there were any statistically significant differences in the proportion of children using different negative and different positive coping strategies. Chi-square tests for categorical variables were then used to determine the types of coping strategies used by the total sample, and by younger (age 6–11 years) and older (12–15 years) children and sex (male, female) groups. T-tests for continuous variables were used to determine mean use of positive and negative coping strategies in response to a specific stressor. For Aim 2, normal distribution assumptions across all efficacy items were not met by Shapiro–Wilk tests. Therefore, group medians and standard errors (SE) were used to examine children’s efficacy ratings for each coping strategy. Where two items assessed efficacy of a single type of coping strategy and children endorsed both items, an average perceived efficacy rating was used. As children only reported the efficacy of those coping strategies that they had used, perceived efficacy was not examined by age and sex groups given the low number of responses. For Aim 3, Pearson’s corelations (r) and Analysis of Variance (ANOVA) were used to examine associations between the total number of (i) positive and (ii) negative strategies used and children’s self-reported HRQoL. Because of the number of analyses and small sample size, a Bonferroni adjustment with a p-value of less than 0.005 was set as the criterion for significance to control for Type 1 errors. All data analyses were performed using IBM SPSS software, version 23.
RESULTS
Sample characteristics
The prevalence study identified 159 affected children living in New Zealand on the point prevalence date. As shown in Table 2, in the prevalence sample, the mean age was 9.04±3.75 years [range 0–15 years], and the majority of children were male (68.7%, 33/48) [40]. The most common diagnoses were DMD (38.3%, 61/159) and congenital myopathy (23.9%, 38/159). Of the 122 families contacted, 50.0% (61/122) of children completed an impact assessment (Fig. 1). Of those children who completed an impact assessment, 78.6% (48/61) of children had Kidcope data available and were included in the current analysis. The non-enrolled sample aged 6 to 15 years who were excluded in the current analysis (n = 85) were similar (p > 0.05) to those children included (30.1%, 48/159) for those characteristics shown in Table 1, except for sex (77.6%, 66/85 males versus (vs) 58.3%, 28/159, p = .01) and ethnicity (25.9%, 22/85 NZ European vs 62.5%, 30/48, p < 0.001). The majority of children included in the current analysis were male (58.3%, 28/48) and New Zealand European (62.5%, 30/48). DMD was the most common diagnosis (35.4%, 17/48). One quarter of all children in the current study had co-morbid medical conditions (25.0%, 12/48), most commonly attention deficit conditions (n = 2), malignant hypothermia (n = 2), and allergies (n = 2). Other co-morbid medical conditions included, but were not limited to, asthma, facial dysplasia, and anxiety disorder (ns = 1). Across the 3 Kidcope items assessing emotional responses in relation to the stated scenario, more than half of all children reported feeling ‘A little’ to ‘Very much’ nervous/anxious (63.8%, 30/47), sad/unhappy (57.4%, 27/47), and/or cross/angry (53.2%, 25/47).
Sample characteristics
*n = 39 due to 9 cases of missing data.
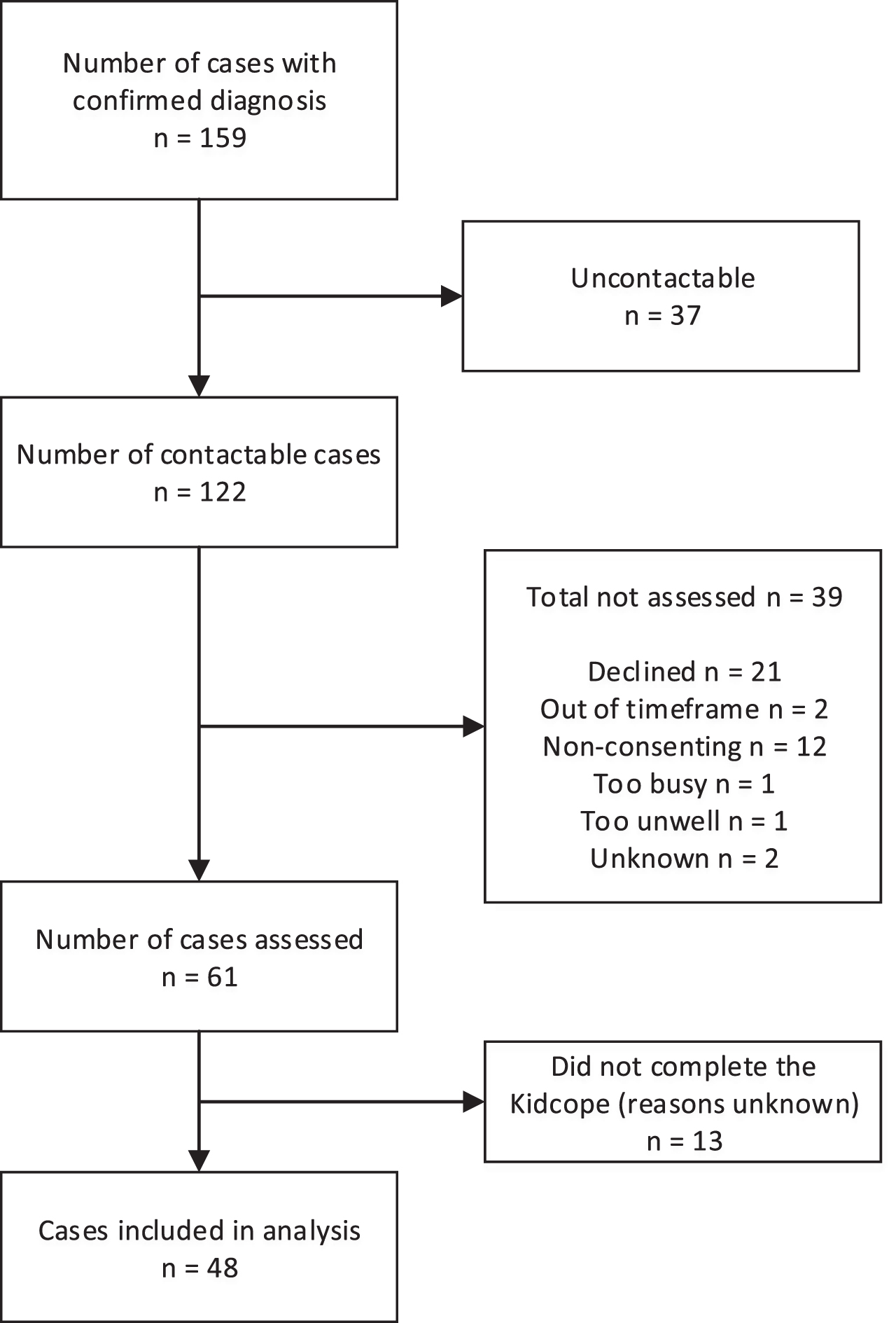
Flowchart of child recruitment.
Coping strategy use (Aim 1)
As shown in Table 3 and in response to a specifc stressor (a visit to the doctor), there were no significant differences in the proportions of children who reported using the four positive coping strategies (ranging from 52.1% [problem-solving] to 70.8 % [cognitive restructuring], χ2(3) = 3.545, p = 0.315), with more than half of all children using positive coping strategies. In contrast, there was greater variation in children’s use of the six different negative coping strategies (ranging from 12.5% [self-critism] to 75.0% [wishful thinking], χ2(5) = 74.19, p < 0.001). Most frequently used negative strategies were ‘wishful thinking’ (75.0%, 36/48) and distraction (68.8%, 33/48), and positive strategies were ‘cognitive restructuring’ (70.8%, 34/48) and ‘social support’ (68.8%, 33/48). Least frequently used coping strategies were ‘self-criticism’, ‘blaming others’, and/or ‘resignation’ (all negative strategies). An inspection of data (Table 3) shows that this pattern was largely consistent across all age and sex groups (p > 0.005).
Coping strategy use by total sample, age and sex groups in response to a specific stressor (visit to a doctor) (Aim 1)
†n = 46 due to two cases of missing data. *n = 47 due to one case of missing data.
Coping strategy perceived efficacy (Aim 2)
As shown in Table 4, ‘social support’, ‘distraction’, and ‘resignation’ were perceived to be the most effective and ‘blaming others’, and ‘self-criticism’ as the least effective coping strategies in response to the targeted stressor (doctor visit) (Table 4). Overall, children perceived positive coping strategies as more effective than negative coping strategies, with the exceptions of ‘distraction’ and ‘resignation’ that were rated as effective.
Group median (SE) perceived efficacy of coping strategies in response to a specific stressor (visit to a doctor) (Aim 2)
n = number of children rating the perceived efficacy of each coping strategy. SE = Standard Error.
Child coping strategy use and HRQoL (Aim 3)
The total number of positive, r = –0.421, p = 0.01, and negative, r = –0.532, p = 0.01, coping strategies used by children were negatively correlated with children’s self-reported HRQoL. Children’s self-reported HRQoL was associated with the total number of positive (p = 0.017) and negative (p = 0.001) coping strategies used by children (Table 5). Following Bonferroni adjustment using a p-value of p < 0.005, use of a greater number of negative coping strategies was linked to significantly poorer mean HRQoL.
Positive and negative coping strategy use in response to a specific stressor (visit to a doctor) and mean self-reported HRQoL (Aim 3)
HRQoL: Health Related Quality of Life measured using the ‘About My Neuromuscular Disease’ subscale of the PedsQL 3.0 Neuromuscular Module.
DISCUSSION
We investigated coping strategy use and perceived efficacy in response to a specific stressor (visit to a doctor) and links to HRQoL in a population-based sample of children with a genetic muscle disorder. According to our findings, children with a genetic muscle disorder most frequently used ‘wishful thinking’, ‘cognitive restructuring’, ‘distraction’ and ‘social support’. Least used strategies were ‘self-criticism’, ‘blaming others’ and ‘resignation’. These findings are similar to those reported by Donaldson and colleagues (2000) who used the Kidcope instrument to examine coping among 768 elementary, middle, and high-school students (aged 9–17 years) in response to school, parents/family, siblings, and peer/interpersonal stressors [15]. As found in our study, ‘wishful thinking’ was used most frequently, whereas ‘blaming others’, ‘self-criticism’ and ‘resignation’ were least frequently used. Together, these findings suggest that the coping strategies used by children with genetic muscle disorders are comparable to strategies used by school children of a similar age when encountering everyday stressors. As in our study, Donaldson found that coping strategy use was similar for boys and girls and during childhood (9–11 years) and early adolescence (12–14 years). Donaldson found that older adolescents (15–18 years) used a greater variety of coping strategies compared with younger age groups. Tesei and colleagues examination of coping strategies used by children and young adults living with muscular dystrophies did not differ significantly from the general population with the exception of less frequent use of problem solving strategies [31]. In the current study, problem solving was one of the least frequently used positive coping strategies. This pattern of findings concurs with previous studies suggesting that problem-focused coping may be more common in controllable situations and decrease in less controllable situations [26, 41].
While our hypothesis of different coping strategy use across age groups was not supported, our sample did not include older adolescents (> 15 years). Examination of a sample of older adolescents with genetic muscle disorders may reveal age-related differences similar to those reported by Donaldson and colleagues. Together, these findings suggest that support programmes around coping that are designed for general school-aged children may also be helpful for children with a genetic muscle disorders across different age (6–15 years) and sex groups. However, it is important to acknowledge that the current study was not statistically powered to exclude inter-group differences based on these latter factors. Others have reported sex-based differences in coping strategy use in different populations, including children with chronic illnesses [20, 42]. Replication in larger samples will be required to confirm the similarities in coping strategy use across groups observed in the current study, and in response to other stressors associated with living with a genetic muscle disorder.
In terms of perceived efficacy, those positive coping strategies most used by children (cognitive restructuring, social support) in response to the stressor (visit to the doctor) were also rated the most effective. This finding suggests that the children in this sample had some insight into which positive strategies were most helpful and that these strategies were being implemented in an effective way. However, there appears to be less of a connection between use and perceived efficacy when examining negative coping strategies. ‘Wishful thinking’ was the most frequently used strategy out of the 10 assessed by the Kidcope. Yet this strategy was rated less helpful than other strategies. This finding may reflect some difficulties and/or a lack of knowledge about the use of alternative and more effective coping strategies. Children using ‘wishful thinking’, for example, may benefit from additional support to transition to using other more effective strategies. Overall, perceived efficacy findings from the current sample suggest that children with genetic muscle disorders are able to select and effectively use positive coping strategies but they may benefit from education and support about those coping strategies which may be less helpful.
Our hypothesis that children who used a greater number of positive coping strategies would report better HRQoL was not supported. Rather, findings from the current study suggest that children’s HRQoL actually decreased as the number of positive and, in particular, negative coping strategies being used increased. One possible explanation is that those children using a greater number of different types of coping strategies, whether negative or positive strategies, were doing so in an increased effort to manage their stressors. Times of disease progression may be especially important for supporting children in their efforts to cope. Patients with muscular dystrophy, particularly in DMD, report increased psychological distress when they are aware the progression of the disease [3, 43]. Further, interviews with adults in the advanced stages of DMD revealed heightened anxiety during critical disease-progression milestones, such as first time use of a wheelchair or respirator [3]. Children’s use of a higher number of different types of positive and/or negative coping strategies may be a flag for increased distress.
Importantly, it is not appropriate to assume any cause and effect relationships between children’s coping strategy use and HRQoL based on data from the current study. Children’s use of coping strategies may be used to manage and influence the emotional conseqences of stressful situations [13], such as stressors associated with increased frequency of doctor visits among those living with a genetic muscle disease [2]. However, it is unlikely that there is a direct association between children’s use of coping strategies and their HRQoL. It is more likely that effective coping strategies may influence a child’s emotional response by alleviating distress. In other words, relationships between stressors associated with living with a genetic muscle disease and HRQoL may be mediated by children’s use of coping strategies.
The present study has some limitations. Given study data were collected as part of a prevalence study, the small size of the sample was limited to those cases identified on the point prevalence date. The small sample limited the study design to a certain extent. For example, we were unable to examine children’s coping strategies in relation to specific co-morbidities (e.g. learning difficulties, intellectual and other developmental disabilities, autism, Attention Deficit Hyperactivity Disorder) that can differ, at least to some extent, across genetic muscle disorder diagnoses. A larger sample would better support the examination of additional factors that may impact children’s use and perceived efficacy of specific coping strategies. Sampling bias is also possible, given those families who were most stressed, not coping, and/or in the greatest need of support, may have been less inclined to take part in an impact assessment. Families who feel they are coping well, and are less stressed, may be more likely to have time and energy available to support study participation. We did not examine other factors that can affect coping and outcome such as family and environmental factors, and specific comorbidities that would ideally be examined in a larger study sample. It is also important to acknowledge measurement limitations in the current study. The Kidcope was originally designed to assess children’s coping within the context of general healthcare consultations. In the current study, we assessed coping among children living with a genetic muscle disorder in relation to a visit to the doctor that they weren’t very happy about. However, we did not specifically ask children to think about a doctor visit specifically related to their genetic muscle disorder. Further, rather than using a more in-depth interview approach, we used the Kidcope screening tool to provide an initial insight into children’s coping in response to a specific stressor (doctor visit). It is important to acknowledge that coping strategies may vary across different types of stressors associated with living with a genetic muscle disorder. However, initial use of a brief screening measure examining coping in response to a specific stressor may be more feasible in a clinical setting. Finally, we must state that this was an exploratory study. Despite these limitations, our findings provide an initial insight into the coping of children with a genetic muscle disorder. An added strength is our focus on child self-report that does not appear to have been previously examined across a range of genetic muscle disorders and including children and adolescents.
Our study findings, along with an increasing proportion of individuals with genetic muscle disorders living into adulthood [44, 45], highlights the need for further research to better understand coping in children with a genetic muscle disease. Future research should investigate whether changes in coping occur over the course of the disorder and established stages of the coping process (i.e. shock and denial, anxiety, anger and guilt, depression and psychological homeostasis) [46], and seek to identify what aspects of genetic muscle disorders are most stressful. This could be achieved by self-identification of key illness-related and non-illness-related stressors as used in previous studies [22]. It would also be useful in future studies to examine coping strategies and perceived efficacy across different environments and stressors (i.e. school, siblings, friends, and boy-girlfriend relationships), as well as the potential impact of approved and experimental therapeutic options on children’s perspectives of coping (and HRQoL). Finally, further investigation should focus on the effects of coping skills training for children and any potential secondary benefits for parents and families. Clinically, more in-depth knowledge of coping across different types of stressors could inform the timing and nature of targeted therapeutic strategies that could be offered at specific points in the disorder (i.e. initial awareness of diagnosis, transition to adolescence, greater duration/severity of illness, etc.). We conclude that those children with genetic muscle disorders use a wide range of positive and/or negative coping strategies to cope with stressors associated with a visit to a doctor and may benefit from greater support to improve HRQoL. Findings also support the value of routine screening of coping in children with genetic muscle disorders.
Footnotes
ACKNOWLEDGMENTS INCLUDING SOURCES OF SUPPORT
We are indebted to the participating families and their children who were willing to share their experiences with us. We also thank the research team for their hard work and commitment to ensuring the success of the MD-PREV study. Members of the MD-PREV research group are: Alice Theadom (Chair and Principal Investigator), Kerry Walker, Tamasin Taylor, Miriam Rodrigues, Richard Roxburgh, Gina O’Grady, Annemarei Ranta, Donald Love, Jenny Stewart, Gemma Poke, Graeme Hammond-Tooke, Ronelle Baker, Margaret Williams, Kelly Jones, Braden Te Ao, Priya Parmar, Valery Feigin, and Rita Krishnamurthi. This work was supported by the Health Research Council of New Zealand [grant number 14/399] and The Brendel Trust.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.