
Abstract
Background:
Spinal muscular atrophy (SMA) is hereditary motor neuron disorder, characterised by the degeneration of motor neurons and progressive muscle weakness. It is caused by the homozygous loss of function of the survival motor neuron (SMN) 1 gene. SMA shows a wide variability of disease severity.
Objective:
To investigate self-reported bulbar problems in patients with SMA, and their relationship to age, functional motor scores and active maximum mouth opening.
Methods:
We used the Diagnostic List of Dysphagia and Dysarthria in (pediatric) patients and relevant recent clinical data from the national SMA database.
Results:
The 118 included patients with SMA frequently reported jaw problems (34%), fatigue associated with mastication (44%), choking (56%) and intelligibility problems (27%). Jaw, mastication and swallowing problems frequently occurred in combination with each other. There was an increase of reported bulbar problems in patients with SMA type 3a, older than 30 years of age, compared to younger patients of this SMA type.
The Hammersmith Functional Motor Scale Expanded scores showed a negligible correlation with jaw and mastication problems, a low negative correlation with swallowing problems and a moderate negative correlation with intelligibility problems. Reduced mouth opening showed a significant, but low correlation with bulbar complaints in patients with SMA type 2.
Conclusions:
Fatigue associated with mastication and swallowing problems were frequently reported complaints. Patients 30 years and older with milder forms of SMA showed an increase of self-reported bulbar problems.
Abbreviations
HFMS(E) = Hammersmith Functional Motor Scale Expanded; METC = Medical research and Ethics Committee; SMA = spinal muscular atrophy; DDD(p)NMD = Diagnostic List of Dysphagia and Dysarthria in (pediatric) patients with
Neuromuscular Diseases; aMMO = active maximum mouth opening;
INTRODUCTION
Proximal spinal muscular atrophy (SMA) is a hereditary motor neuron disorder caused by the homozygous loss of function of the survival motor neuron (SMN) 1 gene. It is characterized by large variability in disease severity as reflected by the SMA classification system, that distinguishes four SMA types (i.e. type 1–4) based on age at onset and the acquisition of specific motor milestones (i.e. sitting and walking independently) [1–3]. SMA is characterized by degeneration of alpha-motor neurons in the spinal cord and dysfunction of the neuromuscular junction [4]. This causes progressive muscle weakness that is most pronounced in proximal muscle groups of the extremities, axial and respiratory muscles [1, 5]. Post-mortem studies also showed abnormalities of brainstem motor nuclei, suggesting that bulbar functions (of speech and swallowing) are affected in a caudal to rostral gradient [6].
The number of studies on bulbar functions such as mastication, swallowing and speech, in SMA is relatively small [7–10]. Instrumental swallowing studies have shown abnormalities, i.e. piecemeal deglutition, post-swallow residue in the valleculae and above the upper esophageal sphincter, but have only been performed in small numbers of patients with relatively severe motor deficits [11, 12]. Questionnaire-based studies have explored the prevalence of bulbar problems [10, 14]. These studies showed that a substantial group of patients reported problems with biting, chewing, mouth opening and swallowing, but they did not cover the full spectrum of SMA. Finally, magnetic resonance imaging (MRI) studies have shown fatty infiltration of specific bulbar muscle groups [10].
Nutritional management, swallowing and gastrointestinal dysfunction are an important topic in the standards of care that focuses on management of children with SMA [5]. The aims of this study were to explore some important questions regarding bulbar function that remain to be answered. These include: 1) what is the prevalence of self-reported problems of mastication and swallowing across the full age and severity spectrum of SMA?; 2) what is the prevalence of speech problems?; 3) are age, the level of motor function and active maximum mouth opening (aMMO) correlates of bulbar dysfunction?
In addition, we explored the test-retest reliability of the Diagnostic List of Dysphagia and Dysarthria in (pediatric) patients with Neuromuscular Diseases (DDD(p)NMD).
PATIENTS AND METHODS
Patients
We invited 185 patients with a genetically confirmed diagnosis of SMA registered in the Dutch SMA registry, to complete a questionnaire about feeding and swallowing problems. In case of young children, caregivers were asked to fill in the questionnaire. Patients who gave informed consent filled in an online questionnaire using a unique personal access code, which they had received by email. Patient characteristics are summarized in Table 1.
Patient Characteristics
Abbreviations: SMA, spinal muscular atrophy; M, male; F, female; n, number of patients; HFMS(E), Hammersmith Functional Motor Scale Expanded. *All patients with SMA type 1 in this study survived infancy.
The Dutch SMA registry contains detailed data collected as part of an ongoing population-based prospective study. We classified SMA types according to the following criteria: type 1: onset before 6 months, does not learn to sit; type 2: onset between 6–18 months, able (or has been able) to sit independently; type 3a: onset between 18–36 months, able (or has been able) to walk without support; type 3b: onset after > 3 years, able (or has been able) to walk without support; type 4: onset > 30 years) [3]. We also used the most recent entries in the registry regarding the need for (non-)invasive ventilation, aMMO and the HFMS(E) scores, a widely used score that reflects (remaining) motor function in SMA [20]. For aMMO, which reflects fatty infiltration of specific bulbar muscle groups, patients were asked to open their mouth as wide as possible. The distance was measured between the right maxillary and mandibular incisors as described previously [9, 10].
We defined swallowing problems as problems with moving food or drinks from the oral cavity to the esophagus. Choking was defined as a blockage of the airway by foods or drinks.
The Medical research and Ethics Committee (METC) of the University Medical Center Utrecht was consulted and approved the study protocol according to the Dutch legislation on clinical studies.
The questionnaire
The Diagnostic List of Dysphagia and Dysarthria in (pediatric) patients with Neuromuscular Diseases (DDD(p)NMD) was originally developed by a group of speech-language therapists involved in the care of dysphagia and dysarthria in neuromuscular diseases with the aim of identifying feeding and swallowing problems [15]. The questionnaire consists of 39 dichotomous questions and 2 multiple choice questions, including specific questions about jaw function, mastication and swallowing problems, the need to adapt food consistency, mealtime duration, requirement for tube feeding, weight issues, occurrence of respiratory infections, and intelligibility problems in particular complaints about insufficient loudness of the voice, shortness of breath when talking, getting tired when talking (supplementary file).
To compose a severity score of the reported bulbar problems, four composite scores were created by adding up the reported jaw (4 items), mastication 3 items), swallowing (5 items) and intelligibility problems (6 items). A total composite score of the items related to feeding was created by adding up the composite jaw, mastication and swallowing scores (12 items). To assess the reproducibility of the questionnaire, a random sample of 30 patients was asked to fill in the questionnaire a second and a third time with a time interval of four weeks.
Statistical analysis
Descriptive statistics were used for patient characteristics and questionnaire responses (n, %). For analysis we combined the subgroups SMA type 3b and 4, as subgroup 4 was very small (n = 3), and disease course is largely comparable.
Associations between bulbar problems were tested using Fisher Exact Test for categorical data. Bulbar problems among different age-groups were presented as frequencies. The correlation between the reported jaw, mastication and swallowing problems and data about functional motor abilities were analysed using Spearman’s rank test, as HFMS(E) is an ordinal scale. The correlation between a MMO and reported jaw, mastication and swallowing problems was analysed using Kendall’s Tau because of the size of the patient subgroups (n = 27 and n = 14). To evaluate test-retest reliability, the agreement of the dichotomous items was analyzed with a two-way random effects intraclass correlation coefficient (ICC) and a Cohen’s kappa. The level of significance for two-tailed p-values was set at <0.05. All analyses were performed in SPSS 22 (IBM,SPSS statistics version 22, Chicago, IL, USA).
RESULTS
Patients
In total, 118 patients (or their caregivers) (age range 1–75 years) completed and returned the questionnaire (response rate: 64%). We assumed that adult patients reported their own experiences and that parents did this on behalf of or together with their children. No significant differences in gender (p = 1.00), age (p = 0.21), SMA type (p = 0.58), use of (non-) invasive ventilation (p = 0.51) or HFMS(E) scores (p = 0.36) were detected between the responders and non-responders.
The study was conducted from September 2016 to November 2017, a period in which Nusinersen was not reimbursed in the Netherlands. Patient characteristics are summarized in Table 1.
Reported bulbar problems
Mastication, swallowing and intelligibility problems were reported more frequently by patients with the more severe forms of SMA, but jaw problems were reported to an equal degree across the different types of SMA. Detailed answers on the questionnaire are depicted in Table 2. The most common bulbar problems reported by all patients, irrespective of SMA type, were ‘biting off a large piece of food’ (34%); ‘fatigue associated with mastication’ (44%); ‘choking’ (56%) and ‘a weak voice’ (27%). Swallowing problems (i.e. swallowing food and the feeling of food getting stuck in the throat) were mainly related to solid food. There was a significant association between jaw and mastication problems (p < 0.001), jaw and swallowing problems (p < 0.001), and mastication and swallowing problems (p < 0.001).
Prevalence of jaw, mastication, swallowing and intelligibility problems
Data are given as n (%) or median (range). *All SMA type 1 patients in this study survived infancy.
The questionnaire revealed various issues related to feeding and swallowing problems, like the need to adapt food (cutting into small pieces, pureeing food or avoiding hard foods), meal duration, getting tired when eating, eating or drinking insufficiently and dreading mealtimes (Fig. 1). Nearly half of the 55 patients who adapted their food did not manage to finish their meals within 30 minutes. In addition, a considerable number of patients reported difficulty eating enough (8%), drinking enough (14%) or eating and drinking enough (3%), but did not receive (partial) tube feeding.
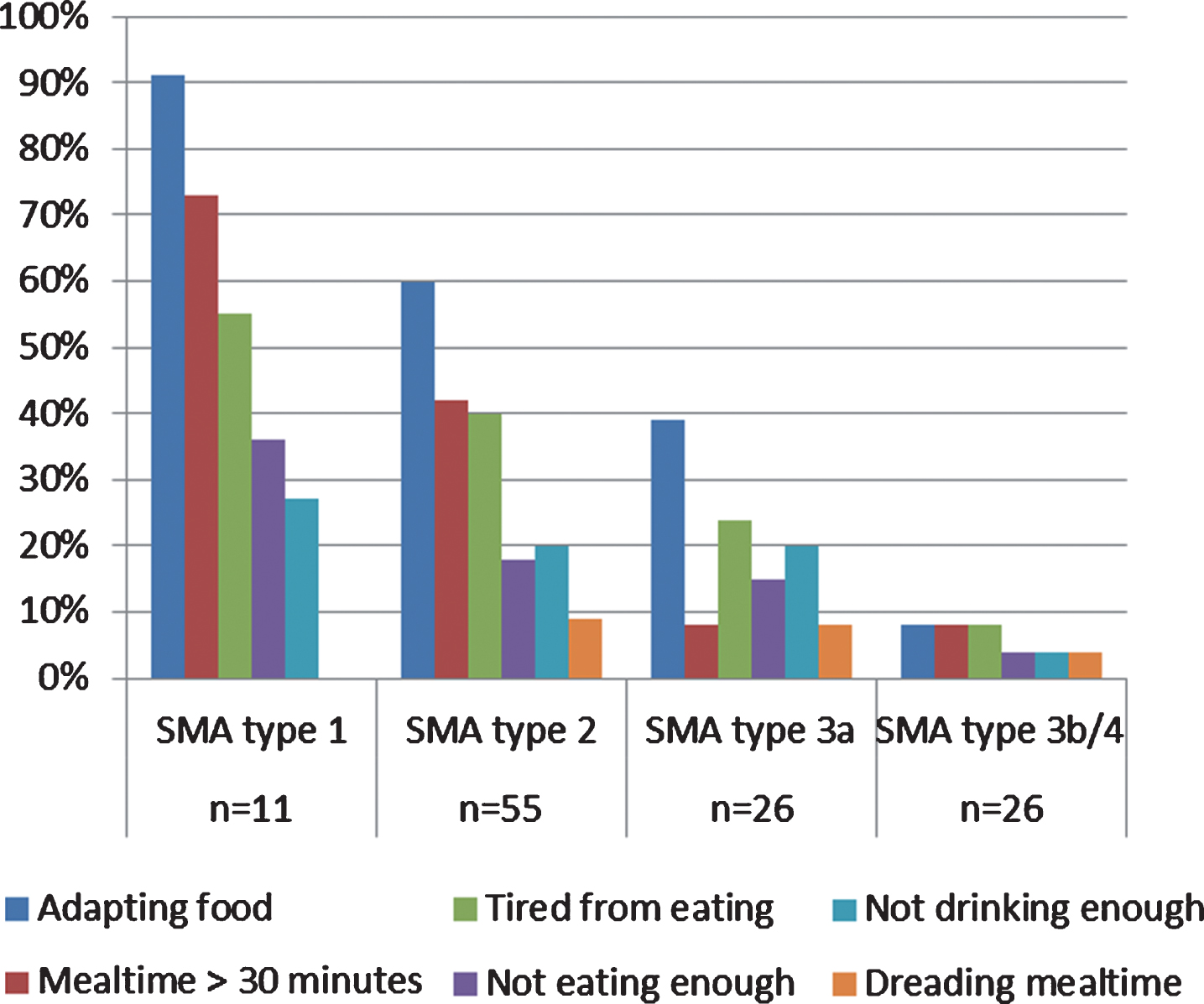
Feeding related issues reported by patients with SMA type 1, 2, 3a, 3b/4 (N = 118).
Influence of age on reported bulbar problems
We investigated bulbar problems among different age groups stratified for SMA type (Fig. 2). Patients of all age-groups with SMA type 2 reported jaw, mastication, swallowing and intelligibility problems. Almost all patients with SMA type 3a aged 30 years and older (n = 16) reported swallowing problems. Other bulbar problems were also frequently reported in this age group of SMA type 3a patients, in particular jaw (60%), mastication (33%) and intelligibility problems (60%).
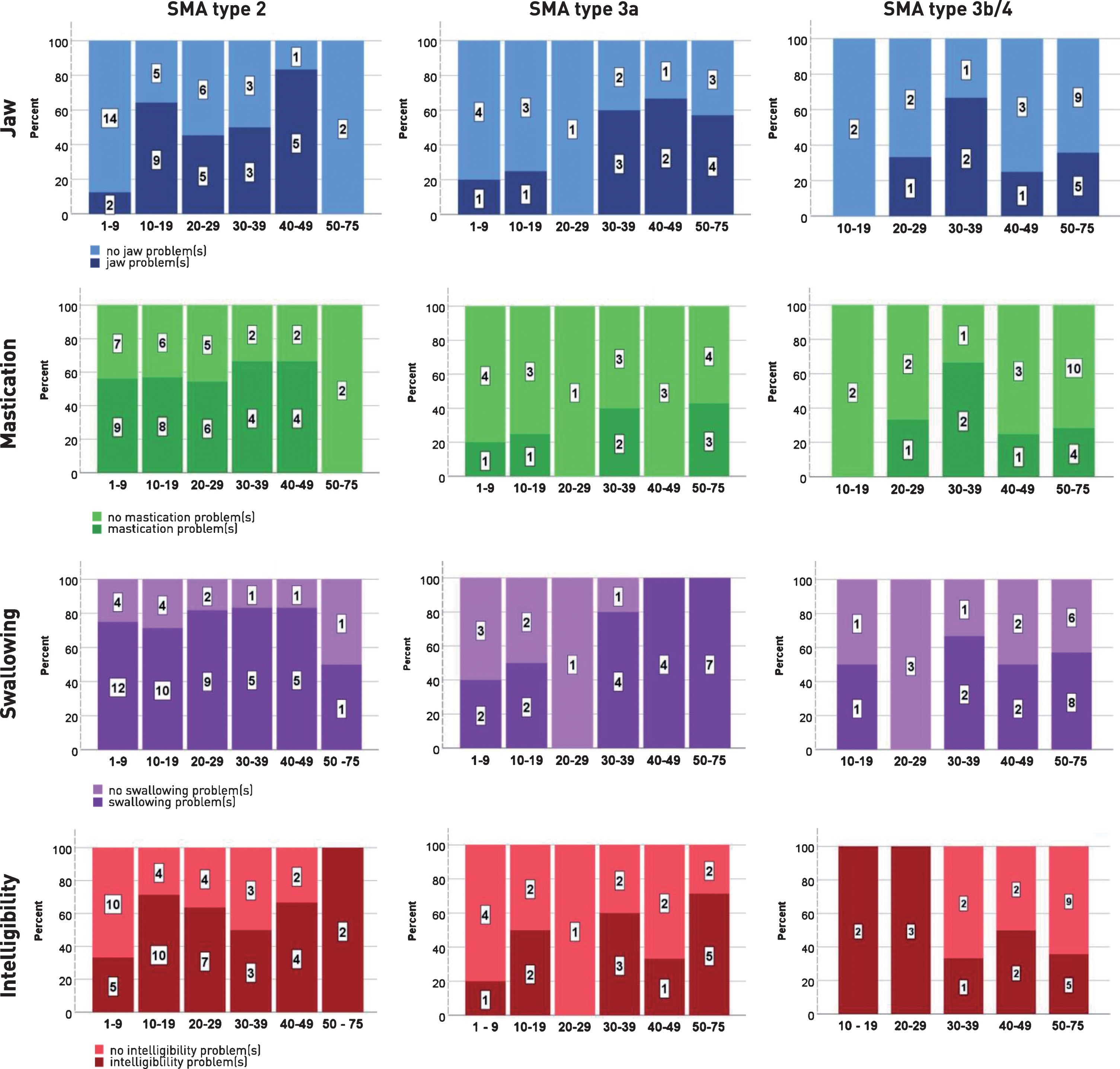
Reported bulbar problems in SMA type 2, 3a, 3b/IV, across different age-groups per type SMA.
Patients with SMA type 3b/4 aged 30 years and older (n = 21) reported jaw (38%), mastication (33%), swallowing (57%) and intelligibility problems (38%).
Functional motor abilities and reported bulbar problems
The HFMS(E) score (n = 101) showed a negligible correlation with reported jaw problems (rs = – 0.28, p = 0.005) and mastication problems (rs = – 0.27, p = 0.006); a low negative correlation with swallowing problems (rs = – 0.48, p = <0.001) and a moderate negative correlation with intelligibility problems (rs = – 0.54, p = <0.001).
Active maximum mouth opening in relation to reported jaw, mastication and swallowing problems
The correlation between aMMO and reported bulbar problems (total composite score, see methods) in patients with SMA type 2 (n = 27) was low (τ= – 0.39, p = 0.007). There was no significant correlation between aMMO and reported bulbar problems in patients with SMA type 3a (n = 14) (τ= 0.083, p = 0.694) and 3b/IV (n = 17) (τ= – 0.016, p = 0.933) (Fig. 3).

The relationship between aMMO in millimeters (n = 93) and the total composite score (0–12 points) in patients with SMA type 2, 3a and 3b/4.
Test-retest reliability of the questionnaire
Fourteen out of 30 patients (or their caregivers) (47%) returned the questionnaire a second and third time. The Intra-rater reliability of the Diagnostic List of Dysphagia and Dysarthria in (pediatric) patients with Neuromuscular Diseases (DDD(p)NMD) was high for the total score (n = 14, ICC = 0.94, (CI 0.80 – 0.98), and sub scores of jaw problems (ICC = 0.96, (CI 0.87 – 0.99), mastication problems (ICC = 0.99, CI 0.97 – 1.00), swallowing problems (ICC = 0.95, (CI 0.84 – 0.98) and speech problems (.ICC = 0.91, (CI 0.73 – 0.97). The Cohen’s Kappa was > 0.80 for 14 out of 27 items and 0.60 – 0.79 for six items (i.e. problems swallowing food, mealtime longer than 30 minutes, choking, tired when eating, jaw problems when laughing and sore throat when speaking). The Cohen’s kappa was <0.60 for three items (i.e. coughing with solid foods, jaw problems when biting off large food, sufficient voice volume). The Cohen’s Kappa could not be calculated for four items (coughing when drinking, excessive belching, eating enough, (partial) tube feeding), as a result of a correction for chance agreement when too many answers fall into the same category (for example the majority of the patients answered ‘coughing when drinking’ with ‘no’).
DISCUSSION
This study aimed at documenting self-reported bulbar problems in SMA. It adds important new information to previous studies. First, we included patients across the entire age and severity spectrum of SMA. Second, the questionnaire used (DDD(p)NMD), which overlaps with those used previously [13, 14], showed good test-retest characteristics. Finally, we studied correlations with HFMS(E) and aMMO, scores that reflect the overall level of motor function and of bulbar muscles, respectively.
A significant proportion of SMA patients, including aging patients with milder variants, experience bulbar problems. This is important to note, as previous studies have primarily identified bulbar problems in younger and more severely affected patients [13, 14]. Jaw, mastication and swallowing problems frequently occurred in combination with each other. This implies that when patients report jaw, mastication or swallowing problems, this may reflect a wider range or combination of bulbar problems. We show that fatigue associated with mastication is relatively common as suggested previously [5, 7]. We also found reduced intelligibility interfering with communication in daily life, an item that was not studied previously, in a large proportion of patients. Fatigue associated with mastication and swallowing problems may preclude some patients from achieving sufficient intake.
In addition to exploring the prevalence of specific bulbar problems, we studied correlates of bulbar dysfunction. Age correlated with the presence of bulbar complaints. This suggests that swallowing and mastication problems, which are relatively uncommon among younger patients with SMA type 3a and 3b/4, may become more common after the age of 30 years, although we cannot exclude the possibility that this difference is caused by caregiver reporting in younger and self-reporting in older patients. We also found a low to moderate negative correlation of swallowing and intelligibility problems with HFMS(E). Motor scores decline with longer disease duration, which may help to explain progressive bulbar complaints with advancing age [16–19]. Finally, we hypothesized that aMMO is more closely associated with bulbar dysfunction. The correlation between aMMO and bulbar problems was - similar to previous observations [10] - significant for patients with SMA type 2, but not in type 3a and 3b/4. This suggests that the value aMMO in the assessment of bulbar problems is limited to type 2. Questionnaires, estimates of motor scores and aMMO may be tools to identify patients with bulbar function limitations. However, the true prevalence of bulbar function problems is probably even higher than self-reported, as patients may adapt to gradually worsening function. For example, problems with mouth opening were dramatically underreported [8–10]. Additional validated instruments to detect bulbar dysfunction are needed, or at least a like-for-like comparison of instrumental swallowing studies and questionnaire results. One of the strengths of our study is the relatively large sample size that covers the full spectrum of SMA. This allowed us to document bulbar problems in patients with all ages, milder forms of SMA and long disease duration. Our data also identified intelligibility problems and fatigability of bulbar muscles that may have been overlooked previously. Finally, we showed that the degree of reproducibility of the questionnaire is probably good.
This study also has limitations. Although the response rate is satisfactory and no significant differences were detected between responders and non-responders, it is possible that patients with relatively severe bulbar complaints are over represented. We therefore cannot exclude that this may have led to an overestimation of bulbar problems. Another limitation is that patients were not asked about their motor function, i.e. the capacity to bring food to the mouth, or to perform oral care independently. However, the questionnaire consists of questions that clearly refer to mastication and swallowing. The question about the ability to brush teeth had the intention to reveal limitations in jaw opening. Since patients may have interpreted this question as the ability to brush their teeth independently, it was excluded from analysis. Statistical power of subgroup analyses was limited as in previous studies. Finally, the use of self-reporting questionnaires has its limitations, not in the least because patients and caregivers may report differently. Nonetheless, our work shows that awareness of bulbar problems in all SMA types and ages needs improvement.
Future studies to further delineate bulbar problems in SMA may benefit from combining more objective measures for bulbar dysfunction, e.g. video-fluoroscopic swallowing studies or imaging of bulbar muscles, with subjective questionnaires.
CONTRIBUTORS
AMBH contributed to study design, analyzed and interpreted data, and drafted the manuscript. CAW contributed to study design, performed statistical analyses, analyzed and interpreted data, and critically revised the manuscript. RIW contributed to study design, performed statistical analyses, analyzed and interpreted data, and critically revised the manuscript. FA, critically revised the manuscript. MTAA critically revised the manuscript; BB critically revised the manuscript. IC, critically revised the manuscript. EG, critically revised the manuscript, including writing for content, study concept. LHB, critically revised the manuscript. WLP contributed to revising the manuscript for content, including writing for content, study concept or design, analysis or interpretation of data, statistical analysis, study supervision or coordination, obtaining funding. LE contributed to revising the manuscript for content, including writing for content, study concept, analysis or interpretation of data, statistical analysis, study supervision or coordination.
FUNDING SOURCE
This study was supported by research grants from the Prinses Beatrix Spierfonds, WOB 14-25.
ROLE OF THE FUNDING SOURCE
The funding source who provided support for the conduct of the research had no role in study design; in the collection, design, and interpretation of the data; in the writing of the report; and in the decision to submit the article for publication.
DECLARATION OF INTERESTS
AMBH, CW, RIW, FA, MTAA, BB, IC, EG, LE declare no financial or other conflicts of interest. LB reports grants from Netherlands ALS Foundation, Prinses Beatrix Spierfonds, Netherlands Organization for Health Research and Development (Vici scheme), the European Community’s Health Seventh Framework Program (FP7/2007-2013, grant agreement no. 259867), and personal fees from Baxter and Biogen (Scientific Advisory Boards). WP receives research support from the Prinses Beatrix Spierfonds, Stichting Spieren voor Spieren and Netherlands ALS foundation. His employer receives fees for ad hoc consultancy services to Biogen (scientific advisory board), Avexis (scientific advisory board), and Novartis (data-monitoring committee).