
Abstract
Background:
We have previously shown that patients with chronic inflammatory demyelinating polyneuropathy (CIDP) improve muscle strength and aerobic capacity after resistance and aerobic exercise.
Objective:
The purpose of this study was to determine if muscle strength and aerobic capacity are preserved one year after discontinuation of regular exercise.
Methods:
All patients in the previous exercise study were eligible for a one-year follow-up with measurement of combined isokinetic muscle strength (cIKS) by dynamometry and maximal oxygen consumption velocity (VO2-max). Data are presented as median (ranges).
Results:
Ten of 17 patients accepted to participate in the follow-up study. Following the exercise study six patients discontinued exercise and at one-year follow-up cIKS had decreased by –13.0 % (–25.8 to –2.9) (p = 0.03) and VO2-max by –16.6 % (–18.8 to –12.6) (p = 0.06). Four patients continued exercise (three with aerobic training and one with resistance training) and at one-year follow-up cIKS and VO2-max were preserved compared to the end of the exercise study (11.6 % (–8.9 to 32.1) (p = 0.88) and –8.4 % (–34.5 to –2.2) (p = 0.13), respectively).
Conclusions:
Continuation of aerobic and resistance exercise may preserve gains in muscle strength and aerobic capacity in patients with CIDP.
INTRODUCTION
In chronic inflammatory demyelinating polyneuropathy (CIDP), treatment with injection of subcutaneous immunoglobulin (SCIG) is effective to improve and preserve muscle strength [1, 2]. Whether physical training as add-on to medical treatment is effective, is sparsely studied.
In CIDP, few studies have described a positive effect of training on muscle strength, quality of life and aerobic capacity, but interpretation has been complicated by inclusion of mixed groups of patients with inflammatory polyneuropathy (Guillain-Barré syndrome and CIDP) [3–5]. In a recent study of CIDP patients treated with SCIG, we demonstrated an improvement in muscle strength by 14 % and in aerobic capacity by 11 % after twelve weeks of resistance and aerobic training [6].
The aim of the present follow-up study is to determine whether muscle strength and aerobic capacity are preserved one-year after discontinuation of regular intensive training.
METHODS
All patients included had participated in the previous study of resistance and aerobic training in CIDP patients treated with SCIG as described elsewhere [6] and gave informed consent to participate in the follow-up study. They had all completed 12 weeks of unilateral resistance training of elbow and knee flexion/extension three times weekly with increasing loads. The untrained side served as control. Moreover, they performed aerobic training on an ergometer bike three times weekly for 12 weeks at a heart rate of 70 % of the maximal heart rate. Participants were neither recommended to continue or stop regular training at the end of the scheduled training until the follow-up visit.
One-year after the training study had stopped we asked the patients to perform a follow-up test. This encompassed measurement of combined isokinetic muscle strength (cIKS) of knee and elbow flexion/extension bilaterally and determination of aerobic capacity on ergometer bike with increasing loads with measurement of maximal oxygen consumption velocity (VO2-max). Moreover, a clinical examination of muscle strength by Medical Research Council (MRC) score, a 6-minute-walk test (6-MWT) and questionnaires about disability (overall disability sum score, ODSS), fatigue (Fatigue Severity Scale, FSS) and quality of life (Short form 36, SF36) were assessed.
The study was approved by the local ethics committee of the Central Region of Denmark. All participants gave informed consent.
Data are presented as medians (range) and compared by paired or unpaired t-test, or rank sum score when not following Gaussian distribution.
RESULTS
Ten out of seventeen participants were evaluated at the follow-up visit. All patients were stable and optimally treated for their CIDP and received SCIG as the only immune modulatory treatment.
Two of the ten patients had continued regular aerobic bicycle exercise after study participation (#2 and #4), one did aerobic training (running) (#8) and one had continued resistance training (#10), however, not at the same intensity level as during the study period.
They trained two to three times weekly for 30 to 60 minutes per training session. Baseline data and the gain in muscle strength and aerobic capacity due to participation in the previous training study are presented in Table 1 for each subgroup.
Baseline data including gains in muscle strength and aerobic capacity during the training study for the ten patients included in the follow-up
Note: Values are numbers or median (range).
In the six patients discontinuing regular training cIKS decreased by –13.0 % (–25.8 to –2.9) (p = 0.03), whereas the four patients continuing exercise had an unchanged cIKS of 11.6 % (–8.9 to 32.1) (p = 0.88) compared to week 12. For both groups cIKS was unchanged compared to baseline (week 0), 5.7 % (–10.3 to 20.3) (p = 0.22) and 23.5 % (–4.6 to 34.6) (p = 0.25), respectively.
Patient #10, who continued resistance training, gained 33 % in muscle strength during follow-up, but was almost unchanged during the previous training period of 12 weeks. Patient #8, who continued aerobic training by running, gained 22 % in muscle strength. Finally, patient #7 had a remarkable increase in muscle strength (62 %) during the training study period, but deteriorated by 40 % at follow-up following discontinuation. Only two patients had a lower level of muscle strength at follow-up compared to baseline (week 0) (Fig. 1a).
Aerobic capacity tended to decrease in the six patients discontinuing exercise (–16.6 % (–18.8 to –12.6) (p = 0.063)). The four patients continuing exercise had an unchanged aerobic capacity, –8.4 % (–34.5 to –2.2) (p = 0.13), (Fig. 1b). Three patients had a lower level of aerobic capacity at follow-up compared to baseline.
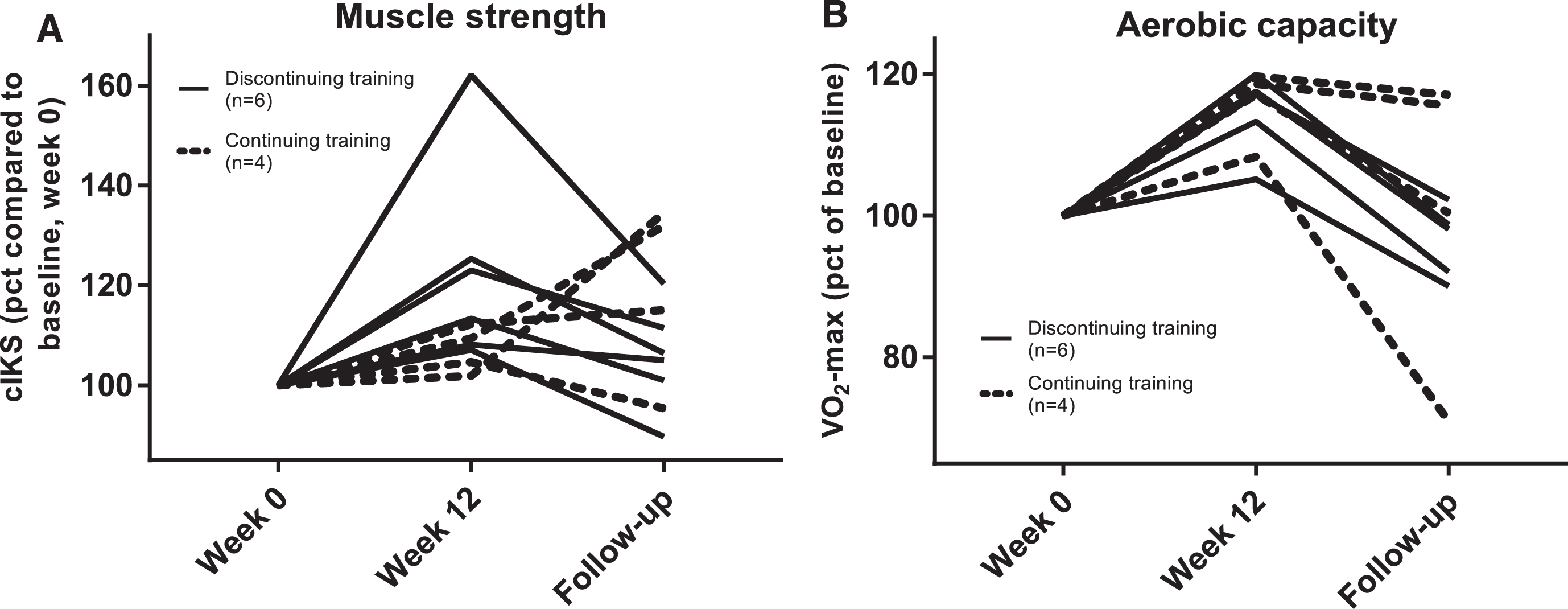
Individual changes in isokinetic muscle strength (cIKS) (A) and maximal oxygen consumption velocity (VO2-max) (B) during participation in previous training study (week 0 to 12) and at the one-year follow-up.
At follow-up, the MRC score was unchanged in both groups (continued vs. discontinued) compared to week 0 (–0.3 % (–3.0 to 0) (p = 0.50) vs. –0.6 % (–1.8 to 2.9) (p = 0.88)) and to week 12 (0 % (–0.6 to 0.6) (p = 0.67) vs. 0.3 % (–1.1 to 6.7) (p > 0.99).
The 6-MWT was unchanged compared to week 0 (5.6 % (–0.9 to 22.2) (p = 0.25) vs. –0.1 % (–3.4 to 2.8) (p = 0.75)) and to week 12 (0.2 % (–1.3 to 9.7) (p = 0.88) vs. –3.3 % (–6.6 to 9.6) (p = 0.63)).
Disability evaluated by the ODSS was unaltered compared to week 0 (–1 point (–3 to 3) (p = 0.75) vs. 0 point (–1 to 1) (p = 0.99)) and to week 12 (0 point (–2 to 3) (p = 0.99) vs. 0.5 point (–2 to 1) (p = 0.99)).
Quality of life by SF 36 and FSS were unchanged in both groups compared to baseline and week 12 (data not shown).
Comparing the ten patients participating at follow-up with the seven patients not participating, there was no significant difference in the response to aerobic and resistance training during the initial 12 weeks trial.
DISCUSSION
This is the first study to evaluate the muscle strength and aerobic capacity after discontinuation of regular intensive physical training for 12 weeks in CIDP.
Only one of four studies of physical training in immune-mediated polyneuropathy evaluated CIDP exclusively [6]. The other studies included a mixed group of patients with Guillain-Barré syndrome and CIDP patients [3–5]. All studies reported a significant increase of muscle strength and aerobic capacity, but none of these studies assessed the long-term effect of physical training.
In other neurological diseases (e.g. myopathies and myotonic dystrophy), physical training has been shown to increase muscle strength and aerobic capacity [7–9]. Moreover, in line with the present study, a follow-up in stroke patients one year after a training intervention showed that despite discontinuation of regular training, muscle strength was preserved, but aerobic capacity decreased to baseline level [10]. Maintenance of muscle strength after discontinuation of regular training has been demonstrated in healthy elderly [11, 12] as well as in patients with multiple sclerosis [13].
Clearly, a limitation of our follow-up study is that only 10 out of 17 patients (59 %) agreed to participate and that 60 % did not continue regular exercise. Interestingly, the response to resistance and aerobic training was similar in patients participating at follow-up compared to the rest of the original cohort. This indicates that not only patients who improved at the initial intervention continued training. When evaluating patients who continued exercise with those who discontinued there was a significant decline in muscle strength, whereas the aerobic capacity only tended to be lower in the group discontinuing training. All patients discontinuing exercise had a decrease in muscle strength and aerobic capacity. In three of the four patients continuing exercise muscle strength had increased considerably (15, 22 and 33 % increase compared to week 12). For aerobic capacity two patients had a decline of 14 and 34 %. It seems that to maintain or improve aerobic capacity, high-intensity training is necessary. Of the four patients continuing training, they all reported that the intensity was lower during the follow-up period than during the intervention period.
It is possible that included patients had a higher physical activity after discontinuation of regular training than those declining to participate. Another limitation could be the variation in adherence to training following the initial study and lack of documentation of the amount of other training performed. Only four patients continued regular training at the end of participation and only one of them performed resistance training. This further supports the finding that the preserved muscle strength is not due to continued resistance training, only [6]. To preserve aerobic capacity it seems mandatory to perform exercise at a high intensity level. The level of intensity of training during the follow-up period was not recorded. The main reasons for discontinuing training, was that the patients felt it was too time consuming, and that the regular follow-up during the intervention encouraged them to continue training. To further improve adherence to continued training we suggest to include regular contacts during a follow-up period, a training coach and training in smaller groups. Finally, individualized training sessions with a combination of aerobic and whole body resistance training could also be beneficial to improve compliance. In future trials, we suggest inclusion of additional assessments such as fatigue scores and pain scores, and focus on more individualized training (e.g. training of balance) to optimize the effects of regular training. Finally, a combination of external electrical stimulation of muscles combined with resistance exercise could be considered.
In conclusion, we find that muscle strength and aerobic capacity declined after discontinuation of regular intensive exercise, but was unchanged in patients continuing with aerobic or resistance training. This further underscores the importance of resistance and aerobic training interventions and suggests that recommendations for regular training are necessary to preserve aerobic capacity in patients with CIDP.
DISCLOSURE OF CONFLICTS OF INTERESTS
Lars K. Markvardsen received speaker honoraria from Octapharma and CSL Behring.
Anne-Kathrine R. Carstens has no conflicts of interest.
Kirsten L. Knak has no conflicts of interest
Kristian Overgaard has no conflicts of interest
John Vissing received research and travel support and speaker honoraria from Genzyme/Sanofi and Ultragenyx Pharmaceuticals and served as consultant on advisory boards of Genzyme/Sanofi, Lundbeck, Ultragenyx Pharmaceuticals, NOVO Nordisk and Alexion Pharmaceuticals.
Henning Andersen received research and travel support from Octapharma, CSL Behring and Genzyme/Sanofi, speaker honoraria from Genzyme/Sanofi and served as consultant on advisory board of UCB Pharma, NMD Pharma and Genzyme/Sanofi.
Footnotes
ACKNOWLEDGMENTS
Gitte Kaiser Hartvigsen and Janni Mosgaard Jensen from Section for Sport Science, Department of Public Health, Aarhus University are thanked for their assistance.