
Abstract
Background:
Serological testing is routinely performed in the work up for a diagnosis of Amyotrophic Lateral Sclerosis (ALS) to exclude pathologies with similar clinical phenotypes.
Objective:
To determine the proportion of serological workup that changes the primary diagnosis and/or clinical management for patients presenting with signs of ALS.
Methods:
A retrospective chart review was conducted on patients from the Calgary Neuromuscular Intake Clinic in which the neurologist working diagnosis post-assessment is ALS. Charts from 2012 to 2016 with completed standard serological workup were reviewed. The proportion of abnormal results per investigation was determined and whether it resulted in a change in diagnosis and/or clinical management.
Results:
A total of 276 charts were reviewed and 85 met full inclusion criteria. Serum creatine kinase (35%), vitamin B12 (18%), complete blood count with differential (11%), and parathyroid hormone (10%) were the among the investigations that had a proportion of abnormal results greater than 5%. Only 6% of patients had an abnormal result that qualified for a change in their clinical management none of which changed the primary diagnosis of ALS.
Conclusions:
Standard serological investigations in the work-up for a patient with ALS may have low utility from a diagnostic and management perspective.
INTRODUCTION
ALS is the most common form of motor neuron disease (MND), with a reported incidence of 2.4 per 100,000/year in Canada [1]. Serological testing is routinely performed to exclude pathologies with similar clinical phenotypes to ALS [2–4]. Serological investigations ordered at the time of diagnosis of ALS are highly variable and often depend on the neurologist’s index of clinical suspicion, access to resources, and the potential harm to the patient from diagnostic delay [5].
A recent study assessed the consistency of serological workup in patients with probable ALS between neuromuscular specialists [6]. Their results demonstrated a positive consensus (greater than 75% answering they “always” or “often” order) among respondents regarding laboratory workup in patients with suspected ALS for only serum creatine kinase, chemistry panel, and thyroid function. The breadth of investigations ordered per respondent was not reported. To our knowledge, there have been no studies to determine the diagnostic yield of serological investigations in this patient population.
At the University of Calgary Neuromuscular Program, all patients with subacutely progressive neuromuscular symptoms, are assessed at an intake clinic which includes evaluation by a neuromuscular neurologist and nerve conduction/electromyographic studies. Patients diagnosed with ALS at the intake clinic are transferred to the Calgary ALS and Motor Neuron Disease Clinic. This arrangement provides a unique opportunity to evaluate the utility of the serological diagnostic work up of all patients referred to the intake clinic in whom the working diagnosis following their initial assessment is ALS. The ability to review all cases prior to transfer to the appropriate clinic reduces the risk of spectrum bias as patients initially thought to have ALS but ultimately having another diagnosis would not be excluded.
The aim of this study was to determine the frequency of which the serological workup of presenting with signs of ALS: 1. changed their primary diagnosis from ALS; 2. resulted in any clinical management change.
MATERIALS AND METHODS
Patient recruitment
A retrospective chart review was conducted on all living and deceased patients assessed at the intake clinic at the University of Calgary, Neuromuscular Program, Calgary, Canada. All charts from the Neuromuscular Intake Clinic, from October 2012 to September 2016, was reviewed for inclusion in this study. The inclusion criteria was as follows: The subject was considered to have ALS as their working diagnosis at the conclusion of their intake clinic assessment. The subject’s chart contained reported results of more than 90% of serological investigations ordered at the time of the clinic visit for the diagnostic workup of ALS. The following were considered as routine serological investigations: complete blood count with differential, electrolyte panel, liver enzymes, creatine kinase, lead, aluminum, parathyroid hormone level, thyroid function tests, vitamins B12 or folate, erythrocyte sedimentation rate or C-reactive protein, serum and urine protein electrophoresis, rheumatoid factor, and antinuclear antibody. These investigations were considered routine to maximize the number of charts meeting inclusion criteria as they most accurately reflected local neurological practice at the intake clinic throughout the 2012–2016 time period.
Cerebrospinal fluid studies and neuroimaging were not included in the analyses. Additional serological tests ordered by attending neurologists were considered but were not necessary for inclusion. This included screening for Lyme disease, HIV, Kennedy disease (genetic test), Hexosaminidase A deficiency, Human T-Lymphocyte Virus-1 associated myelopathy, anti-ganglioside antibodies, and Myasthenia Gravis antibody testing. These serological investigations became increasingly more common as local practice evolved during the 2012–2016 time period.
Analysis
The proportion of each abnormal result by test was determined. Each abnormal result was assessed for whether it resulted in a change in clinical management by: Identifying a diagnosis other than ALS (i.e. change in primary diagnosis); Any change in clinical management defined as: a new non primary diagnosis (i.e. B12 deficiency) a requirement for a new medication or dose adjustment subsequent requirement of invasive or non-invasive procedures for a specific medical condition other than ALS. new non-pharmacological treatment change in follow-up schedule or adjustment in goals of care
Investigations that had been completed more than 10 times were included in percentage calculations for abnormal results. All tests with a reported change in management were reviewed by both authors to ensure agreement of its classification. This study was approved and received certification by the Conjoint Health Research Ethics Board at the University of Calgary and Alberta Health Services.
RESULTS
A total of 276 charts were consecutively reviewed of which 94 charts had a working diagnosis of ALS at the conclusion of the intake clinic assessment. 9 charts (10%) were excluded because they did not contain at least 90% of the ordered serological work-up for ALS. None of these excluded charts yielded an alternative diagnosis at the most recent visit or time of death. Of the 85 charts meeting full inclusion criteria, 45 were male patients (53%), 50 were alive at time of analysis (59%), and the mean age of patients was 66 (34–84 years old) at the time of the initial assessment.
The proportion of abnormal results for each laboratory investigation is given in Fig. 1. Serum creatine kinase (35%), vitamin B12 (18%), complete blood count with differential (11%), parathyroid hormone (10%), anti-nuclear antibody (10%), thyroid stimulating hormone (6.6%), liver enzymes (6.4%), serum protein electrophoresis (5.4%), and standard electrolytes (5%) had a proportion of abnormal results greater than 5%. Three of the four elevated parathyroid hormone levels were previously established (primary hyperparathyroidism) and the last resolved to normal range with repeat lab work. During their initial assessment, none of these patients had chart documentation of clinical features and/or results on nerve conduction/electromyographic studies considered atypical for a presentation of ALS. There was no documentation on follow-up assessments that previously established treatment for primary hyperparathyroidism may have had an effect on ALS disease progression. A significant proportion of laboratory tests (38%) did not reveal any abnormalities in our analysis.
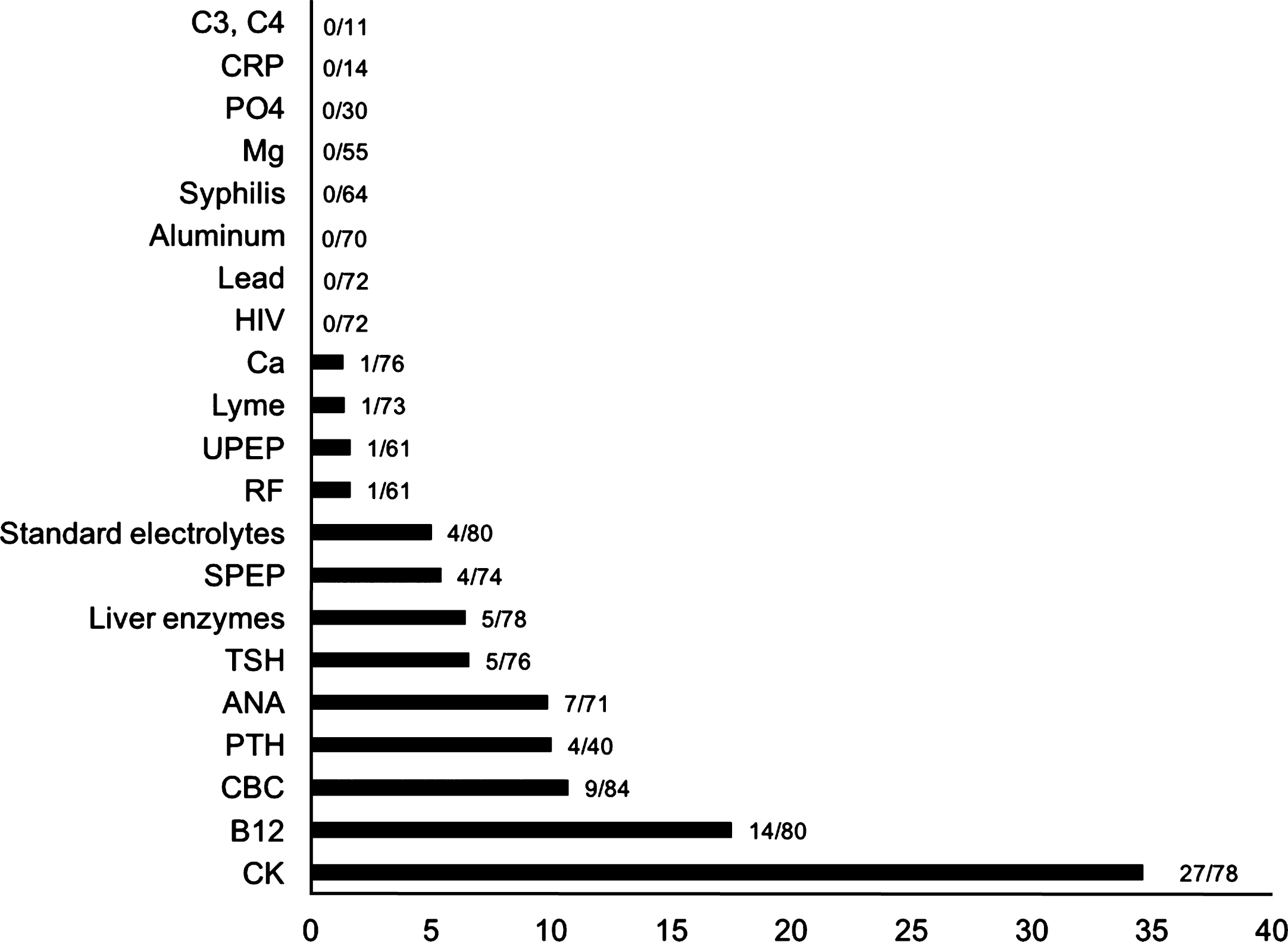
Proportion of abnormal results per investigation in standard ALS laboratory work-up. aHgb, K, and AST represent the highest values of abnormal percentages for complete blood count and differential, standard electrolytes, and liver enzymes respectively. Mg, magnesium; CRP, C-reactive protein; PO4, phosphate; C3, C4, complement; HIV, human immunodeficiency virus; Ca, calcium; UPEP, urine protein electrophoresis; RF, rheumatoid factor; SPEP, serum protein electrophoresis; TSH, thyroid stimulating hormone; ANA, antinuclear antibody; PTH, parathyroid hormone; CBC, complete blood count with differential; B12, cyanocobalamin; CK, creatine kinase.
Five patients (6%) had a change in management directly due to the serological work-up ordered at the time of initial assessment. Two patients had a new non-primary diagnosis of B12 deficiency that required subsequent supplementation. One patient required a medication adjustment that consisted of stopping a diuretic due to hypokalemia. Two patients required repeat or additional laboratory investigations to accurately interpret the abnormality found on initial testing. A patient with elevated serum copper (30.1μmol/L) had a ceruloplasmin level and 24-hour urine copper ordered which were within normal limits. A patient with positive Lyme serology using Western Blot technique had repeat serology which was negative. An infectious disease specialist concluded that it was a false positive and did not contribute to the patient’s condition.
All patients maintained their diagnosis of ALS during their subsequent re-assessments at the MND/ALS clinic without a change in diagnosis at the time of the most recent visit or death. The serological workup did not reveal any concomitant diagnosis that could contribute to the presentation of their primary condition of ALS.
DISCUSSION
This is the first study evaluating the utility of serological investigations in patients with a working ALS following their initial evaluation by a neuromuscular neurologist. The results demonstrate that in our cohort serological laboratory workup does not alter the diagnosis or management. All of the investigations with abnormal results (>5%) were deemed clinically insignificant with exception of the five patients that met criteria for change in management. The moderately elevated creatine kinase was an expected finding in ALS patients. Serum levels ranged from 161 to 1153 units/L but a myopathy was not identified in any patients on follow up. These investigations may be indicated in select cases from a general medical perspective but based on these data we conclude have low utility from a diagnostic and management perspective for patients with findings consistent with ALS. The findings from this study supports that classical serological investigations that are routinely ordered are not warranted for patients with a working diagnosis of ALS provided by a neuromuscular neurologist in a tertiary care center. Given the sensitive nature of this diagnosis, the decision to order serological investigations may include a patient’s concerns of treatable neurological conditions that may present similar to ALS. Our study took advantage of the flow of neuromuscular referrals that capture patients with a working diagnosis of ALS being assessed for the first time by a neuromuscular neurologist. There are many clinical scenarios in which a broader differential diagnosis is held by a neurologist following the initial assessment and additional serological testing may be indicated in those cases. In this study, highly experienced neuromuscular sub-specialists at a referral tertiary care centre provided the consultations and these findings may not generalize to less experienced physicians.
Future studies should attempt to reproduce these results in a larger, prospective cohort study. Broad implications from replicated results include shorter time to diagnosis and reductions in the economic cost of standard serological workup of patients presenting with typical ALS.
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
Footnotes
ACKNOWLEDGMENTS
Georgia Tabler for her assistance in the chart retrieval process.