
Abstract
Dementia with Lewy bodies (DLB) is one of the most common degenerative dementias after Alzheimer’s disease (AD) dementia. DLB is under-diagnosed across populations but may be particularly missed in older Black adults. The object of this review was to examine key features of DLB and potential associations with race in order to hypothesize why DLB may be under-diagnosed in Black adults in the U.S. In terms of dementia, symptoms associated with high rates of co-pathology (e.g., AD, vascular disease) in older Black adults may obscure the clinical picture that might suggest Lewy body pathology. Research also suggests that clinicians may be predisposed to give AD dementia diagnoses to Black adults, potentially missing contributions of Lewy body pathology. Hallucinations in Black adults may be misattributed to AD or primary psychiatric disease rather than Lewy body pathology. Research on the prevalence of REM sleep behavior in diverse populations is lacking, but REM sleep behavior disorder could be under-diagnosed in Black adults due to sleep patterns or reporting by caregivers who are not bed partners. Recognition of parkinsonism could be reduced in Black adults due to clinician biases, cultural effects on self-report, and potentially underlying differences in the frequency of parkinsonism. These considerations are superimposed on structural and systemic contributions to health (e.g., socioeconomic status, education, structural racism) and individual-level social exposures (e.g., social interactions, discrimination). Improving DLB recognition in Black adults will require research to investigate reasons for diagnostic disparities and education to increase identification of core symptoms in this population.
Keywords
INTRODUCTION
Dementia with Lewy bodies (DLB) is one of the most common degenerative dementias after Alzheimer’s disease (AD) dementia. DLB is one of two diagnoses under the broader umbrella of Lewy body dementia, which also includes Parkinson’s disease (PD) dementia. Prevalence studies estimate that DLB accounts for 4.2% of dementia diagnoses in community settings and 7.5% of diagnoses in secondary care [1]. These are likely underestimates, however, as it is believed that 1 in 3 cases of DLB are missed [2] and misdiagnosis as AD is common [2, 3].
While DLB may be under-diagnosed across populations, there is evidence to suggest that it is particularly missed clinically in the U.S. in individuals racialized as Black or African-American (subsequently described as “Black adults”). In a study of the prevalence of dementia subtypes among U.S. Medicare beneficiaries 68 years or older in 2013, diagnosis codes for Lewy body dementia were the least common for Black adults (4.0%). The prevalence of Lewy body dementia codes was 5.5% in White non-Hispanic adults and 6.1% in Hispanic adults [4]. Multiple studies using the U.S.-based National Alzheimer Coordinating Center (NACC) database identified that fewer Black participants with pathologic Lewy body disease had a clinical suspicion for Lewy body dementia in life compared to White or Hispanic participants [5, 6]. Over 96% of participants in clinical trials for Lewy body dementia identify as White [7].
Given that race and ethnicity are social constructs without scientific or biological meaning [8], explanations for the under-diagnosis of DLB in Black adults must look beyond biology. The term “race” is used to group people who share phenotypic features like skin color and are assumed to share an ancestral background, while ethnicity groups people sharing common languages and cultural traditions [8]. Associations of race with health and disease reflect complex relationships between a myriad of factors ranging from individual-level social exposures (e.g., social interactions, discrimination) to structural and systemic determinants (e.g., socioeconomic status, education, and structural racism) [9–11]. Genetic ancestry and admixture can play a small role as well [11]. We thus examined aspects of the core features of DLB and potential associations with race in order to hypothesize why DLB may be under-diagnosed in Black adults in the U.S. and identify possible strategies for increasing DLB recognition in this group.
DEMENTIA AND RACE
Dementia is an essential criterion for DLB diagnoses [12] (though research criteria for mild cognitive impairment due to suspected Lewy body disease also now exist [13]). When considering dementia generally, older Black adults are more likely to be diagnosed with incident dementia than White adults [14], with AD dementia diagnoses occurring at approximately twice the rate in Black versus White Americans [15]. However, Black adults are less likely to receive an incident diagnosis of mild cognitive impairment (MCI) prior to dementia (i.e., early/timely diagnosis; OR 0.73, 95% 0.56–0.94, versus White adults) [16]. In sensitivity analyses, this was particularly true for Black adults living in disadvantaged neighborhoods [16]. Other research also showed that non-Hispanic Black adults had worse cognitive function and more functional limitations at the time of receiving a dementia diagnosis, suggesting diagnostic delays in this group [17]. Reasons for more frequent but delayed dementia diagnoses in Black adults include environmental/contextual influences (e.g., education/educational quality, poverty, living in socially disadvantaged neighborhoods), structural risk factors (e.g., segregation, institutional racism), cardiovascular and metabolic risk factors, biases in neuropsychological testing, study methodological weaknesses (e.g., lack of data or small sample sizes, association studies insufficient for establishing causality, failure to include key social variables), and potentially ancestry [18, 19].
Most research shows that dementia diagnoses can be delayed in Black adults regardless of dementia etiology. But with research suggesting that dementia generally and AD dementia specifically are more commonly diagnosed in Black adults, it remains unclear why DLB would be less frequently identified in this population. It is possible that higher rates of co-pathology in Black adults with dementia [5, 20] and symptoms associated with that co-pathology (e.g., AD, vascular disease) obscure the clinical picture that might suggest the presence of Lewy body pathology. It is also possible that clinicians are predisposed to give AD dementia diagnoses to Black individuals based on the research showing high prevalence in this population. These hypotheses are supported by NACC research showing that 88% of Black participants with Lewy body pathology (65% diffuse, 35% transitional) were assigned a primary etiologic cause of AD clinically, with only 5% assigned a secondary diagnosis of suspected Lewy body disease despite 70% having sufficient Lewy body pathology to predict an intermediate-high likelihood of a clinical DLB presentation [5]. Unrecognized Lewy body disease could also potentially help explain lower proportions of amyloid PET positivity among Black adults with MCI or dementia [21].
THE INTERSECTION OF RACE AND CORE FEATURES OF DLB
To meet DLB criteria, individuals must have 2 of 4 core clinical features (or 1 core clinical feature and 1 indicative biomarker) in addition to dementia. The four core clinical features are visual hallucinations, REM sleep behavior disorder (RBD), fluctuating cognition, and parkinsonism [12]. Below we highlight research findings to illustrate what is known about these core features in older Black adults.
Visual hallucinations
Well-formed visual hallucinations are a core feature of DLB, with other types of psychosis (hallucinations in non-visual modalities, paranoia, delusions) serving as supportive features [12]. In NACC, there were no differences in the frequency of hallucinations or delusions between racial-ethnic groups in individuals clinically diagnosed with cognitive impairment due to Lewy body disease [22]. In individuals with Lewy body disease pathology, there were also no statistically significant differences in the frequency of visual hallucinations reported between racial-ethnic groups [5]. These findings are in contrast to a NACC study using all-cause dementia, where the odds of experiencing hallucinations and delusions were over double among Black participants with dementia (versus White) and other neuropsychiatric symptoms were also more common in Black participants [23]. Other research has also identified that hallucinations and paranoia were more common in Black adults with dementia [24].
These findings suggest that under-reporting of hallucinations and delusions may not be a major barrier to the diagnosis of DLB in Black populations. It is possible, though, that the presence of psychosis is ascribed to conditions other than DLB in Black adults. For example, clinicians may ascribe psychosis to suspected underlying AD co-pathology rather than suspecting or diagnosing comorbid DLB [5]. While hallucinations can occur in AD [25], multiple NACC analyses have found that psychosis (hallucinations and/or delusions) is more common in participants with Lewy body pathology (with or without concomitant AD pathology) [26, 27]. In fact, research from a U.K. brain bank showed that the presence of complex visual hallucinations was the only symptom helpful for identifying the presence of Lewy body disease in the context of mixed Alzheimer and Lewy body pathology [28]. Other research also identified visual hallucinations at presentation as being the best predictor of Lewy body disease on autopsy versus AD [29].
Another possibility is that hallucinations in older Black adults are ascribed to primary psychiatric conditions rather than an underlying dementia. One study found that DLB was initially misdiagnosed as a “mental illness” 24% of the time [3]. Hallucinations occur in both bipolar disorder and schizophrenia [30, 31]. Black individuals are over twice as likely to be diagnosed with schizophrenia versus White individuals [32] and differences in phenotypic presentations in bipolar disorder are thought to contribute to diagnostic disparities between Black and White adults [30]. Potential contributors to psychiatric diagnostic disparities include racial biases in recognition of mood symptoms, diagnostic instrument norms based on White populations, race-related environmental stressors, differences in access to treatment centers, and overlap of delusional and paranoid thoughts with experiences relating to race (e.g., persecution) [33, 34].
Indeed, in studies of delusional content in adults with schizophrenia [33] and older adults hospitalized with an acute psychotic episode [35], Black adults were more likely to report distrust, skepticism, oppressive experiences, and/or persecution from non-specific sources (e.g., “people are out to get me”). Recent research with individuals across the schizophrenia spectrum and non-psychiatric controls identified that Black participants endorsed higher scores on paranoia subscales (e.g., relating to suspiciousness, paranoid ideation), leading to inaccurate risk stratification in some Black individuals [36]. For example, baseline levels of racism-related vigilance or “healthy cultural paranoia”/“adaptive paranoia” were felt to reflect an elevated but appropriate level of awareness that Black individuals may have regarding how others perceive them [36]. In circumstances where individuals have long-standing hallucinations, it is plausible that a pre-existing psychiatric diagnosis obscures the onset of symptoms that might suggest DLB. It is also possible that Black adults are more likely to receive a diagnosis of late-onset primary psychiatric disorder instead of DLB. Recent research showed that Black adults accounted for a higher proportion of Medicare beneficiaries (age ≥66 years) with schizophrenia than Medicare beneficiaries without serious mental illness, and that schizophrenia was associated with a markedly higher dementia prevalence [37]. This study did not report age of schizophrenia diagnosis, however, and whether there are racial differences in the diagnosis of very late onset schizophrenia-like psychosis (diagnosed ≥60 years) in the U.S. is unknown. Very late onset schizophrenia-like psychosis may be a prodromal dementia state, as it is associated with a higher risk of subsequent dementia [38, 39] and a recent retrospective series found that 32% of individuals with very late onset schizophrenia-like psychosis had indicative biomarkers for DLB [40].
REM sleep behavior disorder
The absence of identified RBD is associated with delays in the diagnosis of probable DLB [41], so RBD recognition has clear implications for the prevalence of DLB diagnoses. Population-based studies of RBD in the U.S. include insufficient representation of Black adults to estimate frequency in this population [42, 43]. Research consistently demonstrates differences in sleep patterns between Black versus White adults, though, including shorter sleep duration, worse sleep quality, and more daytime sleepiness in Black adults [44]. Shorter sleep duration has implications for the identification of RBD, as periods of REM sleep increase with longer sleep duration. In a NACC analysis of individuals with Lewy body pathology, a lower proportion of Black participants reported RBD (6.3%) compared to non-Hispanic White participants (18.3%) or Hispanic participants (12.8%), though this was not statistically significant [5]. The Black cohort in the analysis had significantly more women (57%) than other racial ethnic groups (38%, 37%) [5], which could affect RBD prevalence. Women with DLB are less likely to have identified symptoms of RBD, attributed to less vigorous movements in sleep and/or the presence of AD co-pathology [45].
The living situation and care giving structure of Black adults may also affect report of caregiver-observed symptoms such as RBD. Bed partner recognition of abnormal sleep behaviors and bed partner injuries were the most common reasons people sought assessment for RBD symptoms [46]. Black participants in NACC, however, were less likely to have spousal study partners [47, 48], likely affecting the report of RBD symptoms which would most commonly be assessed by bed partners. The observation that Black caregivers are less likely to be spouses is also seen in U.S. caregiver statistics in general [49] and in other studies of older adults with and without dementia [50].
Fluctuations
No identified information, including from NACC studies, provides insight into whether cognitive fluctuations may be reported differently between racial-ethnic groups. A single study assessing Medicare beneficiaries in the National Health and Aging Trends Study found that non-Hispanic Black participants were more likely to have unexpected variations in their cognitive testing performance or dementia classification year-to-year (OR 2.12, 95% CI 1.61–2.78) [51]. Whether this reflects cognitive fluctuations as are seen in DLB or other factors (e.g., recent illness, environment, testing) is uncertain. It is also unknown whether the type of relationship between the caregiver and the person with DLB affects fluctuation reporting. In DLB generally (i.e., unrelated to racial and ethnic considerations), it is uncertain how readily fluctuations are identified across populations or the frequency of this symptom as a presenting feature. In one study, only 28% of individuals later diagnosed with DLB had reported fluctuations at the time of cognitive symptom onset [41]. Timely DLB diagnosis was driven more by the presence of RBD than other symptoms [41]. In a caregiver survey, however, 44% of respondents endorsed lapses in attention or alertness or staring spells as an early symptom [3].
Parkinsonism
Long-standing research documents that PD is diagnosed less commonly in Black (versus White) adults [52–55], with a prevalence ratio of 0.58 (95% CI 0.575–0.81) using 1995 and 2000–2005 Medicare data [55]. In an analysis using 2019 Medicare data, Black adults represented only 5.9% of the PD cohort despite accounting for 10.5% of the Medicare population [56]. It is also established that PD diagnoses are often delayed in Black adults and occur at a greater disease severity [52–54]. There are multiple proposed contributors to this, including healthcare access/disparities [52–54, 56], distrust of the medical system [52, 53], more comorbidities in Black adults [54], earlier age of mortality in Black adults [53], perceptions of aging (i.e., viewing parkinsonism as part of normal aging) [52, 57], clinician biases (in diagnosis, treatment) [52, 53], and clinician biases related to assessing hypomimia/facial expression [58]. However, there is also community-based research suggesting that parkinsonian signs may be less frequent in older Black adults compared to older White adults [59]. How best to reconcile these findings is uncertain.
In a NACC neuropathology study of participants with dementia prior to death, Black adults (with any dementia diagnosis) were less likely to self-report parkinsonism than non-Hispanic White adults (4.6% versus 13.3%, p = 0.01), but there were no differences in Unified Parkinson Disease Rating Scale total scores between groups [60]. The difference between self-reported and examination-based symptoms is also seen in PD studies, where Black adults more commonly under-reported disability than White adults relative to clinician-assessed motor impairment [57]. In a NACC analysis of individuals with cognitive impairment in clinically diagnosed Lewy body diseases, degree of parkinsonism on examination was similar between racial-ethnic groups [22]. It is likely that the same factors resulting in delayed PD diagnoses in Black adults (e.g., under-reporting of symptoms and/or disability, less access to specialty clinics, and other healthcare disparities and biases) also impact DLB diagnosis, but whether there are also differences in the frequency of parkinsonism requires further study.
OTHER POTENTIAL INTERSECTIONS OF RACE AND DLB
Genetics and epigenetics
While race is a social construct, ancestry and genetic admixture can potentially affect disease risk. In Lewy body dementia, identified risk loci include GBA, SNCA, APOE, BIN1, TMEM175, and TPCN1 [61, 62]. APOE and BIN1 may relate more to the common AD co-pathology in Lewy body dementia than to the α-synuclein pathology, however [61, 63], and TPCN1 also associates with AD [62]. These studies all used cohorts of individuals of European ancestry [61–63]. There are known ancestral differences relating to GBA and SNCA variants in PD [64, 65], but only recently have investigators published the results of a comprehensive genome-wide assessment of PD in individuals with African and African admixed ancestry [66]. This research identified a novel risk factor at the GBA1 locus that was unique from the GBA risk loci in European ancestry cohorts [66]. It is likely that this risk locus also has implications for DLB, but what role ancestry plays in the prevalence of DLB in different groups, if any, is uncertain.
Epigenetics is also an active area of research in Lewy body diseases [67–69], but there are limited investigations into the intersection of race and epigenetics to date in DLB. Research suggests that social determinants of health influence epigenetic modifications (e.g., to histones, DNA, micro-RNA) with downstream effects on susceptibility to various diseases, including dementia [70]. For example, epigenetic age (a biological aging marker) was accelerated in Black versus White older adults in the Health and Retirement Study, with impacts on cognitive and functional outcomes [71]. Similarly, other work has shown that chronic financial strain results in premature aging of Black women [72]. This emerging research suggests that in addition to the roles that environmental/contextual influences and structural risk factors may play in clinical diagnoses, these factors may also have implications for epigenetic contributions to disease.
DISCUSSION
Appropriate diagnosis of DLB is critical. One of the benefits of having a dementia diagnosis is validation for caregivers and family members that something is wrong [73]. This may be particularly true in the setting of behavioral symptoms such as psychosis, which can be particularly distressing to caregivers [74]. In some cases, this may be the primary reason that a caregiver brings their loved one to a memory clinic, as suggested by a study that found a higher proportion of Lewy body pathology in postmortem tissue of Blacks adults with dementia compared to White adults with dementia [20]. Identification of suspected underlying Lewy body disease also has implications for prognostic counseling, as Lewy body pathology is associated with progression in cognitively impaired individuals when present alone (i.e., without evidence of AD) and in the setting of AD (biomarkers or pathology) [75–77]. As disease-modifying therapies for dementia are identified, the presence of specific pathologies and/or co-pathologies will have implications for medication use and expected response.
Identification of Lewy body pathology also informs appropriate symptomatic treatment, particularly in the avoidance of potentially harmful medications. Individuals with DLB can have severe hypersensitivity reactions to antipsychotic treatment [78, 79] such that this was included as a supportive feature in the first three iterations of DLB diagnostic criteria [80]. This has implications regarding the risks of under-diagnosing DLB in Black adults. Whereas some research has shown no difference in antipsychotic use by race/ethnicity in community-dwelling individuals with dementia in the US [81], other research found that Black adults had a higher risk of receiving anti-psychotic drugs in nursing homes [82]. While subsequent research found no difference in inappropriate antipsychotic use in facilities with higher versus lower proportions of Black residents [83], research over the same period found a disproportionate increase in schizophrenia diagnoses in Black nursing home residents with AD and related dementias [84, 85]. This suggests that schizophrenia diagnoses may be used to subvert policies to reduce inappropriate antipsychotic use in dementia.
Given the importance of appropriate dementia diagnoses, approaches to improve recognition of DLB/potential Lewy body pathology in Black adults are critical. Potential research strategies could include further investigation of what symptoms herald underlying Lewy body pathology in the presence of other dementias (e.g., AD dementia, vascular dementia), application of emerging synuclein biomarkers in diverse populations, investigation of whether Black adults may receive more diagnoses of very late-onset schizophrenia instead of DLB, studies of RBD in diverse groups, and inclusion of individuals of African ancestry in Lewy body dementia genetic research. Improving clinical recognition of DLB will likely require intervening at multiple levels, including addressing structural racism and far-reaching social determinants of health and inequities, increasing community recognition of DLB signs and symptoms, training and supporting both specialist and non-specialist health care professionals in identifying signs suggesting underlying Lewy body pathology, ensuring access to emerging biomarkers in under-resourced communities, and identifying and implementing strategies to address potential concerns regarding biomarker procedures in diverse groups [16].
There are limitations to this viewpoint and the underlying data. Many of the referenced studies are from NACC, which is not population-based and in which inclusion of minoritized communities is affected by location site, recruitment factors, and focus of the contributing center [86]. The validity of assessing individuals by self-identified race is also uncertain. Persons racialized as “Black” are not a homogeneous group and include individuals from different ancestral, geographical, socioeconomic, and cultural backgrounds. The current viewpoint focused primarily on U.S.-based data, as that is what is available. Future research should take a global perspective on investigating structural and systemic contributions to under-diagnosis of DLB, including minoritized groups in DLB research, identifying DLB in medically under-resourced countries, and including individuals from different ancestral backgrounds in DLB studies.
CONCLUSIONS
DLB is under-diagnosed in Black adults, likely relating to under-recognition of some core features (e.g., RBD), concomitant symptoms relating to co-pathology, and attribution of symptoms to AD or primary psychiatric disease, all on a background of systemic barriers to diagnosis relating to environmental and structural risk factors (Fig. 1). Improving recognition of DLB in Black adults will require further research to investigate reasons for diagnostic disparities and community and clinician education to increase identification of core symptoms in this population.
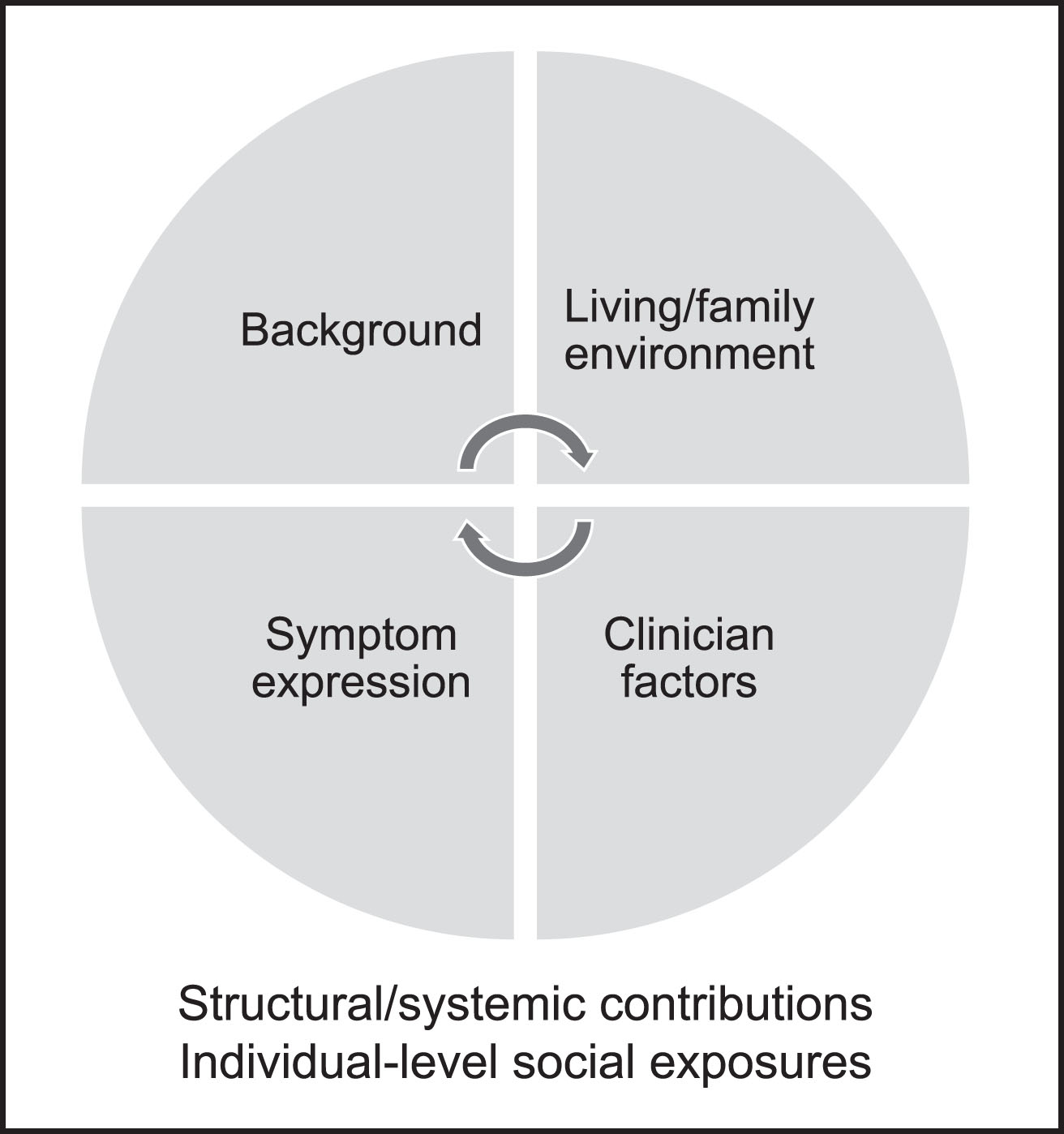
Under-diagnosis of dementia with Lewy bodies (DLB) occurs on the background of structural and systemic contributions to health (e.g., socioeconomic status, education, structural racism) and individual-level social exposures (e.g., social interactions, discrimination) which potentially affect multiple aspects of DLB diagnosis including dementia risk, epigenetics, sleep patterns, and access to care. An individual’s cultural or early life background or social origins may inform how they construe symptoms, such as the possibility that parkinsonism is interpreted as normal aging. Family and caregiver environment can also impact symptom recognition. For example, individuals without spousal caregivers may be less likely to have identified REM sleep behavior disorder. It is unclear whether race affects presentation of DLB symptoms, but there are reasons REM sleep behavior disorder might occur less frequently in Black adults (relating to sleep patterns) and some research suggests rates of cognitive changes and parkinsonism may differ between races. The presence of co-pathology (e.g., relating to Alzheimer’s or vascular diseases) may also affect symptom expression and recognition. In health care contexts, DLB is under-recognized across groups. In Black adults, clinicians may also mis-ascribe symptoms of DLB to other conditions such as Alzheimer’s disease, cerebrovascular disease, and/or primary psychiatric conditions. Improving DLB recognition in Black adults will require research to investigate reasons for diagnostic disparities and education to increase identification of core symptoms in this population.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgements to report.
FUNDING
Work on this manuscript was supported by P30AG066506. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The University of Florida Dorothy Mangurian Headquarters for Lewy Dementia and the Raymond E. Kassar Research Fund for Lewy Body Dementia also provide support for Lewy body dementia projects performed at the University of Florida.
CONFLICT OF INTEREST
Dr. Armstrong receives research support from the NIH (R01AG068128, P30AG066506, R01NS121099, R44AG062072) and as the local PI of a Lewy Body Dementia Association Research Center of Excellence. She serves on the DSMBs for the Alzheimer’s Therapeutic Research Institute/Alzheimer’s Clinical Trial Consortium and the Alzheimer’s Disease Cooperative Study. She has provided educational content for Medscape, Vindico, and Prime CME.
Dr. Barnes receives research support from NIH (R01AG022018, P30AG072975, R01AG056405, UF1NS100599, R01AG062637, RF1AG074549, R01AG070883, R01AG060376, R01AG065398, U19NS120384, R01AG073439, R01AG079226, R01NS125294, R01NR018443, R01AG055430, R01AG067525, R01AG076143, R01AG078533, U19AG078109, R01AG066134, R01AG077948, R01AG073627, R01AG064950, R01AG067497) and the Alzheimer’s Association (AARG-21-852512). She serves as the Deputy Editor for Alzheimer’s & Dementia.