
Abstract
Background:
People with Dementia (PwD) are frequently admitted to hospital settings. The lack of proper dementia knowledge, poor communication skills, negative attitudes toward dementia, and lack of confidence affects the quality of care, thus development of dementia trainings has increased. Nevertheless, literature regarding the effectiveness of training implementation is limited.
Objective:
The aim of this narrative synthesis is to 1) identify the characteristics of training programs and 2) explore the effectiveness of these training programs in everyday clinical practice.
Methods:
A systematic search in PubMed, PsycINFO, CINAHL, and Cochrane was conducted, including qualitative and quantitative peer-reviewed studies. Holton’s evaluation model with its three outcome levels (learning, individual performance, and organizational results) was adopted. 14 studies were included.
Results:
The synthesis of the results was divided into two parts: 1) to describe the characteristics and content of trainings 2) to evaluate the effectiveness of training programs according to the three outcome levels of Holton’s model, taking into consideration its construct domains: ability, motivation, and environment. Learning outcomes were assessed in all selected studies: 13 studies observed changes in individual performance, four studies reported changes within the organizational level, and only five showed sustainable changes over time.
Conclusion:
Person-centered care (PCC) approaches, interactive and varied teaching methods, supporting conditions like champions, action plans, and setting care policies, are all characteristics of effective trainings. Successful programs should be sustainable over time, demonstrating positive outcomes across the organization. Based on current findings, there is a lack of adequate evaluation with regard to training programs on the organizational level.
Keywords
INTRODUCTION
The world’s older population continues to increase, with the number of People with Dementia (PwD) rising in parallel [1]. PwD are more frequently admitted to hospital settings than older people without dementia [2]. It is estimated that 12.9–63.0% of people admitted to general hospitals have dementia [3]. As PwD can be intensive users of health services, caring these patients merits increased attention.
PwD are likely to stay in hospital longer [4] and their clinical outcome is predominantly negative. Malnutrition, dehydration, loss of functionality, increased disorientation, depression and delirium, low detection and diagnosis of dementia, frequent use of antipsychotic drugs, and a high mortality rate are some of the consequences of hospital admission [5]. Furthermore, the longer PwD stay in hospital, the stronger patients’ symptoms of dementia become. Up to 75% of PwD admitted to an acute hospital will experience Behavioral and Psychological Symptoms of Dementia (BPSD) [6], including agitation, aggression, wandering, hallucinations, and sleep disturbances [7] that further cause difficulties in managing and significant distress in caregivers [8–10]. The hospital surrounding appears to be unsuitable for PwD, as it can worsen BPSD [5] due to the fact that hospital admission is considered frightening and confusing for PwD [11].
The lack of proper dementia knowledge by all hospital care team members has recently been characterized as one of the major factors affecting care quality in hospital settings [5]. Moreover, poor communication skills, negative attitudes toward dementia, poor management strategies, and lack of confidence by nursing and medical staff, healthcare assistants, allied healthcare professionals, and other support staff further contribute to poor quality of PwD care [5, 13]. Due to these factors, staff training is highly recommended for hospital surroundings [14].
Adaptation of the way hospital staff providing care for PwD is a complex procedure due to multiple personal, social, and organizational factors prompting different responses to training interventions and, therefore, different outcomes [12]. For instance, staff’s professional focus may affect the way the information about a person’s social or medical history will be used. Also, the expectations of employers for dementia care may have a further impact on how staff members prioritize their work with PwD. In addition, lack of long-term studies and methodological differences of studies make it difficult to compare outcomes.
Although there are reviews describing the current care regarding environment, culture of care, attitudes, and challenging behavior or exploring dementia care best practices including educational staff trainings [4, 5], only few reviews aimed on evaluation of educational programs in hospital settings. A realist review by Handley, Bunn, and Goodman [15] focused on what works about dementia-friendly interventions for PwD in hospital settings and how to achieve desired patient outcomes, including well-being, reduced anti-psychotic medication, reduced distress and challenging behaviors, adverse incidents (such as falls or hospital-acquired infection), and length of stay. A more recent review aimed to evaluate the effectiveness of educational interventions for general hospital staff to improve the care and management of older people with delirium and/or dementia [16]. Although there is limited evidence about the features that characterize effective programs, some suggestions for successful training implementations do exist. Specifically, two recent literature reviews explored the most effective approaches of dementia training and education for hospital staff using a model (Kirkpatrick’s four-level model) to evaluate the outcomes [17, 18]. Thus, the evaluation of training programs' effectiveness is recommended for developing future training programs.
Holton’s evaluation and effectiveness model
To understand influencing factors of educational research outcomes is among the most critical issues in Human Resource Development (HRD). Among several evaluation models, there are four models which are well established in the research fields [19]. The first is Kirkpatrick’s [20] four-dimensional measurement typology (i.e., reactions, learning, behavior, results), which may be the simplest method for understanding training evaluation and the most widely used technique. The second from Tannenbaum and colleagues [21] is based on Kirkpatrick’s typology by adding post-training attitudes and dividing behavior into two outcomes for evaluation: training performance and transfer performance. The third provided by Kraiger [22] has three multidimensional target areas for evaluation: training content and design, changes in learners, and organizational payoffs.
The fourth, Holton’s Human Resource Development Evaluation Research and Measurement Model [23], is a more comprehensive framework than Kirk-patrick’s four level taxonomy. This model integrates not only training evaluation like the others, but also training effectiveness [19]. The model hypo-thesizes that HRD outcomes are primarily a function of ability, motivation, and environmental influences at three outcome levels learning (trainee’s reaction, motivation to learn, ability), individual performance (motivation to transfer, intervention fulfillment, learning outcomes, job attitude, transfer conditions, transfer design), and organizational performance (link to organizational goals, expected utility/or payoffs, external factors). Learning and individual performance represent individual behaviors that an intervention is intended to create. Organizational outcomes can be conceptualized as a function of organizational goals, individual motivation, and environmental factors [23]. Unfortunately, there is no possibility to full test the model because there are no available tools for some of the constructs. Some years ago, the model was modified by delineating specific constructs based on new research or theory [24]. Among several modifications: two separate constructs of “Motivation to Learn” and “Motivation to Transfer” completely re-conceptualized motivation by creating the construct of “Motivation to Improve Work Through Learning” [25]. Besides, the constructs of “Transfer Conditions” and “Transfer Design” were re-conceptualized to one construct: “Learning Transfer System Inventory”, including all factors in the person, training, and organization that influence transfer of learning to job performance. The modified model is more appropriate for empirical testing [24].
This narrative synthesis gives an overview of the established training programs in general hospitals. Its purpose is to 1) identify the characteristics of all the selected training programs relevant to dementia (qualitative and quantitative studies), and 2) explore the effectiveness of each training program according to Holton’s Model (learning, individual performance, organizational changes), interpreting the outcomes in regards to its three constructs: ability, motivation, and environment.
METHODS
Search strategy
A systematic search of research literature was carried out with the help of four commonly used databases: PubMed, PsychInfo, CINAHL, and Coch-rane. The search strategy was conducted by using a combination of terms and subject headings for the following themes: Dementia, Hospital, and Education (Supplementary Material). The first systematic search was conducted in January 2017, and a second systematic search was conducted in September 2019 to identify papers published since January 2017.
Procedure, selection process, and data extraction
This paper follows the PRISMA Statement guidelines [26]. After removing duplicates, articles were separately screened by title, abstract, and relevance by two reviewers, namely MG and JS. Full-text articles that seemed relevant for inclusion in this study, were screened. The following inclusion criteria were implemented: 1) all studies took place in general hospital(s)’ settings/wards; 2) studies were all reported as interventions in the framework of a training or educational program about dementia for staff members involved in the care of PwD; and 3) all studies were written in English. Papers that met the following criteria were excluded: 1) training interventions targeting mainly in hospital staff who were specialists or working in special dementia care units (or psychiatric wards) in hospital settings; 2) reports/projects without intervention/recommendations for projects; 3) reviews/case studies; 4) programs that focus predominantly on staff training for delirium or other geriatric syndromes or issues irrelevant for dementia. Disagreements concerning the criteria for inclusion were resolved by a third party (BT). Data extraction was performed independently by the same two reviewers (MG, JS) using a standard table with the following data: 1) country of the study; 2) type of program; 3) study design; 4) participants (characteristics) and setting; 5) method of intervention (procedure and content); 6) frequency and duration of the program; 7) its evaluation; 8) main results; 9) quality rate of the study.
Quality assessment
A quality assessment of the selected studies was conducted. The quality scores are derived from Spector et al. [27]. Kmet et al. [28] introduced 14 criteria for assessing higher or lower quality of study designs. In this review, eleven items were used (Table 1), as in Scerri et al. [17], since only one included study was a randomized control trial (RCT) and three out of 14 items in this checklist focused on randomization and blinding studies. Each study was rated according to whether it fully met the criteria (2 points), partially met the criteria (1 point), or did not meet the criteria at all (0 points). A calculation was made and the total score summary was divided by the maximum score of 22. By this calculation three levels were categorized: low (<0.6), medium (0.6–0.8), and high (>0.8) quality studies [27]. In the current work, after grouping the studies according to their quality, the researchers set a tighter inclusion criterion, because of the great heterogeneity of the studies and to strengthen their results. Thus, only studies of medium and high quality were included.
Quality rating assessment. From Kmet et al. [28]
Data synthesis strategy
The synthesis of the results was divided in two parts. In the first part, characteristics of studies, participants, and content of training were described. In the second part the evaluation and effectiveness of each training program was described, using the three primary domains of Holton’s Model [23], analyzing also the suggested factors of influence according to its three construct domains ability, motivation, and environment in an attempt to interpret the outcomes.
RESULTS
The search resulted in 6,735 hits. After removing duplicates, title and abstract were initially screened to identify relevant articles. 301 full-text articles were scrutinized. 14 articles met the inclusion criteria, also taking into consideration the quality assessment (Fig. 1).
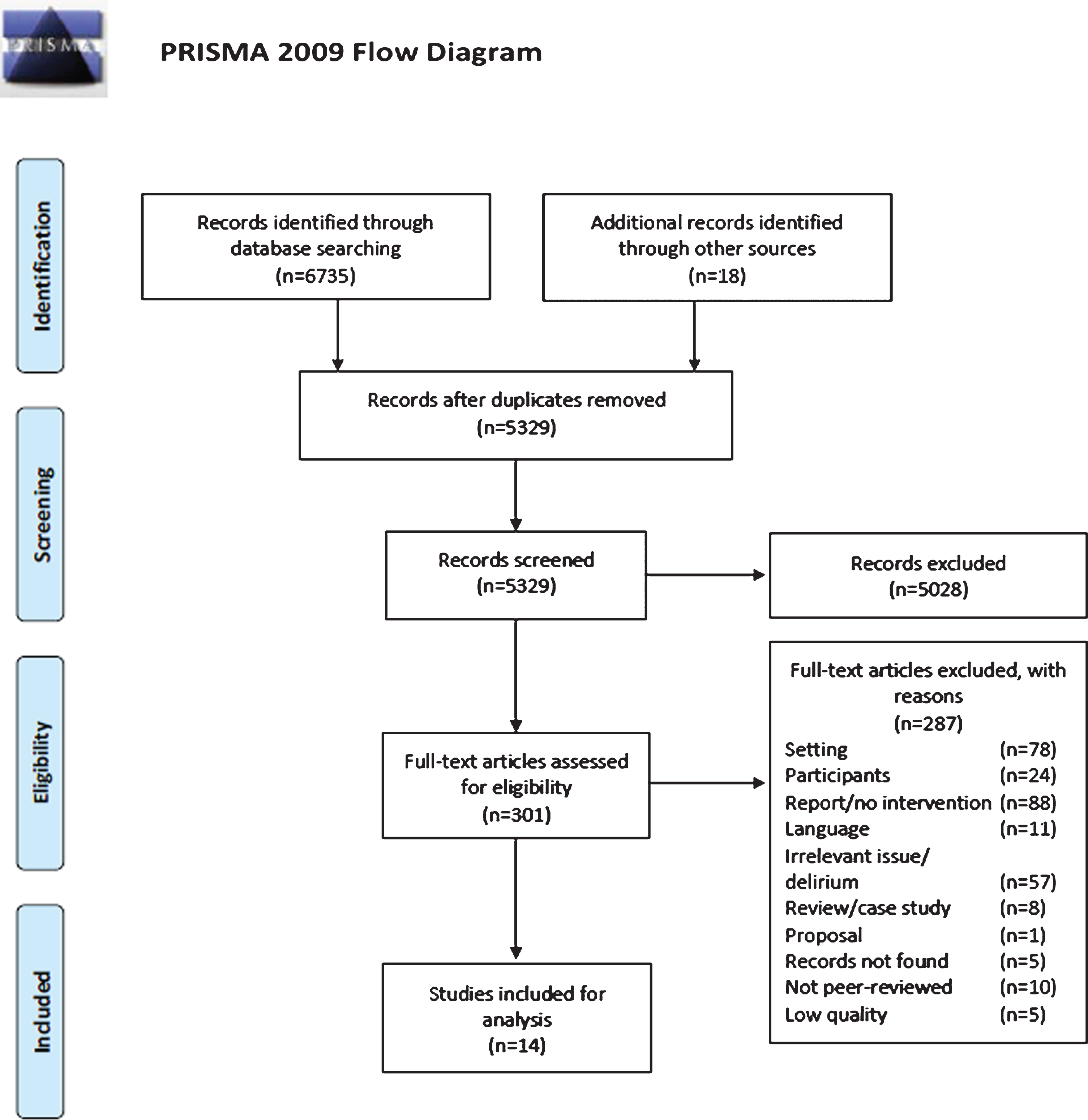
PRISMA flowchart of the search strategy. From Moher, Liberati, Tetzlaff, and Altman [74].
Table 2 presents an overview of the data extraction, with the main focus lying upon the outcome measures and the results of the selected studies.
Data extraction
Characteristics of studies
Eight of the studies were of medium and six of high quality. The quality scores ranged from 0.64 to 0.91. Seven out of the 14 articles came from the UK, while four came from the United States, two from Canada, and one from Malta. Eight studies used pre-post measurement designs, five used pre-post-follow-up measurement designs, while one used only post measurements. Most of the studies used a mixed-methods approach (quantitative and qualitative measurements, n = 10), and four of them used only quantitative measurements. While almost all studies (n = 14) used self-report measurements, two of them conducted observations [29, 30] (Supplementary Table 1).
Characteristics of participants
The study samples ranged from a small group of 25 participants [31] to 2,020 participants [29]. Most of the studies reported interdisciplinary groups of attendees from a wide range of professions. The majority of participants came from the nursing profession. One study included only certified nursing assistants [32], while two studies did not report participant characteristics in detail [30, 32]. Six studies reported the participant’s previous education in dementia [33–38].
Characteristics of the training programs
The included studies described eleven different training programs. The duration of training programs varied from one hour [32] to five and half days [39, 40].
There was a great variation of different teaching methods. Almost all studies used in-classroom or face-to-face-training, four combined this traditional training approach with online resources [39–42], and one used an online training only [31]. Interactive approaches were a crucial component of methodology for the majority of trainings. In specific, videos were among the most frequent/dominant approaches (n = 9), followed by group activities (n = 5) and case studies/scenarios (n = 4). Reflections/reflective diaries (n = 2), roleplaying (n = 2), brainstorming (n = 1), and learning exercises (n = 1) were also used. One study offered one to one coaching in practice [29]. Some studies additionally invited either speakers and guests [39, 40], or integrated actors [41]. To continue learning or to read up what has been learned, participants received learning materials [35] or manuals/booklets at the end of the training [33, 36, 37, 33, 36, 37].
The content of trainings varied. The majority of trainings included content regarding the various aspects of knowledge about PwD, such as topics about general knowledge of dementia (n = 10), communication (n = 11), impact of the physical/hospital environment (n = 5) and fundamentals of dementia care (n = 4), dealing with challenging behaviors (n = 6), working with relatives (n = 5), separate modules relevant to PCC (n = 8), topics about screenings and assessments (n = 5), discharge planning (n = 4), and modules about knowing the person (n = 3). However, two of them were based only on one basic module relevant to PwD’s perspective (Barbara’s story) [29] or a narrative story [30].
Evaluation and effectiveness of training programs according to Holton’s model
Learning
Learning outcomes were assessed in all selected studies (n = 14). The most common learning outcome was dementia knowledge (n = 8, 3 validated tools), followed by outcomes relevant to dealing with challenging behavior (n = 3, all validated tools), measured mostly by self-reports. Level of knowledge is argued to be linked to confidence (n = 10, 6 validated tools) or self-efficacy/competence (n = 3, all validated tolls) as successful learners are expected to feel confident and therefore more motivated to transfer the acquired knowledge. Moreover, knowledge has an influence in trainee’s attitude toward dementia (n = 7, 3 validated tools). Learning behavior is also affected by trainee reactions or perception in the learning environment through the complex interaction between motivation to learn and learning. Thus, satisfaction with the program (n = 8, none validated tool), contributed also to learning evaluation, and were measured by self-reported scales.
Most of the studies used pre-post measurements to evaluate learning outcomes, and the majority of post measurements were conducted immediately after the training. However, sometimes participants’ understanding and perceived behavioral changes are not captured effectively as they often overestimate their knowledge before the training, making measurements of change suspect [43]. Thus, in one study both pre and post measurements were assessed after the program to capture the perception of learning more effectively [32], while other studies collected the post data one or three months after the end of the training program [29, 41]. All included studies with pre-post measurement or only post-measurement design demonstrated significant changes in learning outcomes (n = 9). However, one medium quality study, using a not validated tool, showed a significant increase of knowledge (80%) in the post measurement (after 8 days), but this was not the case by all of the participants in the sample. 12% of the participants indicated a decrease in knowledge related to dementia care, and none possible explanation for that decrease was provided by the authors [31]. According to Holton’s model, the factor of participant’s “ability” to learn may have been influenced by the heterogeneity in job or differences in cognitive ability. Besides, some “environmental” influences such as the lack of a control group, the small sample size (N = 25), and no formal psychometric testing of the knowledge scale, may explain that decrease in knowledge.
It has been suggested that only pre-post and follow-up measurements can directly evaluate real changes through reports/questionnaires or specific tools, otherwise reports about changes immediately after the training may be less strong [30, 33]. Concerning our included studies, sustainability of changes through pre-post-follow-up measurements was tested only in five training programs. Two medium and one high quality programs suggest positive changes in staff attitudes, or/and satisfaction with care, or/and confidence and sense of competence were sustainable, over three months [30, 38]. Two of them used validated tools [30, 38] while one study used tools which were not validated [35]. In one study, despite the overall increase of knowledge, attitudes, and confidence, a decline in one item of the attitudes scale was observed in the follow-up measurement [35]. The “environmental” factor of low psychometric properties of the scale (Cronbach’s alpha is 0.39), may have influenced this result. It is possible that participants misunderstood this PCC item. In two high quality studies, a decline in confidence, knowledge [34], and self-efficacy [33] was observed after four and two months respectively. In Galvin et al. [34] that decline happened only in one out of three included hospitals and the used tools were not validated. Among the possible reasons of those declines may be the uncontrolled “environmental” factors or participants “ability”. According to demographic variables of participants responding to the follow-up measurements, heterogeneities in job, different education background, full or part time job, working in different medical departments including work experience, and high attrition rate may have influenced the sustainability of learning changes [33, 34]. A further possible reason for the decline, according to the applied model, is the staff’s “motivation” to learn. In one study, a high percentage of those who answered the follow-up measurements had received previous dementia education. Participants who received such training may have relied on previously learned information and had limited uptake of new knowledge or they had low expectations/interest in a similar training topic. Thus, receiving three or more hours of dementia training in the last two years before the intervention was one of the strongest predictors of this decrease in knowledge [34].
Furthermore, the workplace as an “environmental” factor may have an impact on the person capacity to “transfer design” by using new learned care approaches. Thus, the limited or lack of time and staff [34, 42], the unpredictable nature of the workload in acute care [33, 42], and variations in the way individuals implement strategies, appeared to be barriers to implement knowledge and sustainable results [42].
Performance outcomes
Learning is expected to lead to individual changes in performance. Changes in attitude can motivate participants to transfer knowledge and implement it into clinical practice. Thus, 13 studies measured changes in individual performance or in clinical practice after the training program. Use of communication techniques (n = 7, 2 validated tools), shift to PCC (n = 6, 5 validated tools), and clinical skills (n = 5, 1 validated tool) were among the most common changes in individual performance. Action plans (n = 4), creating champions/mentors (n = 3), use of tools (n = 3), and decrease of chemical or physical restrains (n = 1) were also included in individual performances outcomes. The majority of these were based on self-reported measurements (n = 12), while a few of them relied on direct observations of care practices (n = 2).
Four medium and one high quality studies stressed an overall change in participant’s clinical skills (n = 5) [30, 35]. Open-ended questions or Likert scales were often assessed to explore the use or possible use of skills in clinical practice immediately after the training, after one/three/or more months [31–33, 41]. Only one study used a validated tool of patient-staff interactions [30].
Further changes in practice were brought about action plans or individual initiatives in clinical practice [30, 39]. Setting action plans or goals for newly acquired knowledge, are important factors, according to Holton’s model, to “transfer the design” of the program into the practice. It may also be a linkage between individual performance and organizational outcomes, according to the applied model. In one study, participants evaluated their own clinical area using a workbook [39].
Most of the studies (n = 6), including almost all high-quality studies (n = 5), reported an overall positive impact of person-centered approaches so as to demonstrate changes in attitudes or in behavior and values. Changes shifted to PCC measured either directly, through open-ended questions [33] or indirectly, being part of validated questionnaires [36–38] or through observation by validated tools [29, 30]. In a pre-post design, PCC shifts were minor [36] and in another pre-post-follow-up study, the observed activities were not always based on PCC [30]. A possible explanation of this may be that the participant’s “ability” regarding job, education, and cognitive abilities varies, and maybe the “motivation to learn” also varies due to their different personalities’ characteristics. Moreover, PCC as a “transfer design” approach may need more time to be adapted by trainees or achieved through consistent long-term relationships with patients [44]. Thus, immediately after the training or few months later is actually a short-term period to implement what they have learned.
Staff also reported that they used the most effective strategies regarding appropriate communication with PwD, in four medium and three high quality studies (n = 7). In some studies, communication changes were evaluated through validated observation tools [29, 30] or through blind rating of simulated assessments [41]. In other studies, the outputs were presented through reports, like open-ended questions [32–34] or reflection reports [39]. In one pre-post experiential learning design there were neither changes of making requests, nor changes in voice’s tone after the training but there was an increase of controlling, bossy, and dominating communication [41]. Again, a possible explanation may be the PCC approaches used in the communication techniques. However, PCC is important to “transfer design” in order to motivate participants, time is needed to change individual performances. The period of one month may be insufficient for participants to demonstrate all the new communication skills learnt on the course. Moreover, there was no agreement in rating, demonstrating a poor inter-rater reliability, which may possibly be an “environmental factor” that influences the outcomes.
Champions or mentors are important for the transfer of knowledge. Although five studies included champions or mentors, only two medium and one high quality studies had an outcome in this respect. Champions or mentors have an influence to the “Learning Transfer System” as part of the “transfer climate” of learning in order for staff to change practice. Champions express a willingness to teach others, to strengthen relationships between services [39] to support and lead changes in the workplace, to improve the experience, care treatment and outcomes [40], and this impacts the way they work with PwD and contributes to the overall training sustainability [29].
Changes in clinical practice may be also reflected by an increased use of assessment or practical tools, measured by open-ended questions and reports in two high and one medium quality studies. Tools may facilitate the “Learning Transfer System” through the “transfer design” according to Holton’s model. In some studies, the routine of screening for delirium, dementia, pain assessment [29, 34], and the gathering of patient information through documentation forms [29, 39] were increased, providing changes in clinical practice. In one high quality study, the use of chemical and physical restrains decreased, demonstrating the applicability of training on their daily practice [33].
Organizational outcomes
Outcomes at the organizational level have been suggested as a consequence of changes in individual performance. Outcomes on the organizational level were identified in four studies. Changes in the hospital environment (n = 3) and setting care polices (n = 3) were among the main outcomes.
Environmental changes affected the organizational outcome in one medium and two high quality studies [29, 39]. Thus, the creation of special rooms for PwD, pictures and signs on bathroom doors for patients with orientation difficulties or useful information on how to adjust physical environments (e.g., light, noise) to the needs of PwD, led to organizational changes immediately after training [39]. However, some participants, in the follow-up measurement, reported significant challenges for implementation, including lack of resources and inflexible plans, all “environmental” factors that can affect the organizational outcomes [39]. Some trainees, using self-report questionnaires in a follow-up measurement, experienced positive changes by using better signage and eating/drinking utensils or by using different colored crockery when offering food to PwD, but some discrepancies have arisen when observations conducted in the wards. Specifically, neither the use of colored cups and jugs or specialist cutlery changed, nor the signage or labels around the ward according to observers’ notes [29]. Moreover, due to some “environmental” influences of the complex hospital workplace, the decrease of noise level could not be managed [29].
A number of changes were reported in the frame of culture, care pathways, and policies in three high quality studies. Some hospitals planned to use activity kits about dementia and one hospital established volunteer teams to assist the care of hospitalized PwD or to place patient at risk in “green gowns” in order for staff to respond appropriately in a dementia-friendly behavior [34]. Besides, some hospitals developed care pathways such as the “carer passport” (allows carers visits out of the normal visiting hour), and non-drug approaches [29]. Other reported organization initiatives were the delivery of the program to all clinical managers and to all acute sites of hospitals, and a refresh of training as a mandatory annual skills review for staff [33].
The expected utility or payoff within an organization can also affect training outcomes. Although there were some reports about cost effectiveness of the programs [39] or indirect impact of cost effectiveness due to decreased physical, and/or chemical restraints [29, 33], there were no specific qualitative and quantitative measurements identified.
DISCUSSION
The aim of this narrative synthesis is to discuss the outcomes of dementia training programs according to an effectiveness model. Outcomes were evaluated according to Holton’s three outcome levels (learning, individual performance, and organizational results) taken into consideration its three basic construct domains: ability, motivation, and environment.
Among other reviews in dementia trainings [15, 45–50] only two examined training programs in hospitals according to an evaluation model like Kirkpatrick’s [17, 18]. Although this model is widely applied, it has been criticized for the incomplete and oversimplified understanding of the transfer process from learning into practice [18, 23]. Recognizing the complexity of trainings in environments such as hospitals is difficult. Thus, Holton’s model includes an independent and highly relevant “organizational level” as an additional outcome.
According to our results, four studies fulfilled the three outcome levels of Holton’s model, while only two of them were of high quality [29, 33]. A learning effect could be observed in all studies, as well as changes in individual performance, which were observed in almost all studies. PCC approaches, interactive and varied teaching methods, champions/mentors and generally supporting conditions, action plans and implementation of care policies, all seemed to be among the successful characteristics of training programs for employees, facilitating “Motivation to Learn” and “Learning Transfer System” according to Holton’s model. However, all these factors are effective only if linked with organizational goals and evaluated across the organizational environment. According to our results, there is a lack of adequate cross-level evaluations (n = 4), perhaps due to the fact that long-term changes on the organizational level are time consuming and longitudinal evaluations are needed. Interestingly, none of the studies directly measured patient outcomes as a result of education and training for staff, which is in accordance with recent review results [16]. Only few of the studies measured interactions between staff and patients through observations [29, 41] and some of their outcomes indicated that patients had a passive engagement, conducted no activities or were socially withdrawn after the trainings [29, 30].
Although there was a gain in learning for all included studies, acquiring knowledge or facts about dementia is not enough to capture practice change resulting in improved care experiences. Given that only 20% of what is taught during training is successfully applied in the working environment [51], a great challenge for researchers is to bridge the gap from knowing to doing.
Applicability of good practices in caring for PwD is one of the most important elements of a successful implementation. Providing PCC approaches, support by champions/mentors, use of specific tools (like dementia/delirium screening, documentation forms), strategies or initiatives like action plans, could lead to changes in staff’s individual performance by “environmental” and “ability” influences like “transferring condition and design” of the training into practice. Moreover, organization factors like transferring knowledge or strengthening the collaborative spirit in third parties (e.g., among providers, expert associations, academics), reducing psychotropic medication and physical restraints, creating a special environment for PwD and applying care policies across organizations, all lead to a high training impact according to our results. In an attempt to formulate a pragmatic “community of practice” approach, one study included an evaluation for the organization (hospital trust) level [29] which seems to be linked with the organization goal according to Holton’ s model.
Moreover, the design, content, and delivery of trainings are all features that influence its applicability. The use of interactive and varied teaching methods, such as action learning, experiential learning, supervision and support seemed to be a strength among the effective trainings [52, 53]. Most of our included studies used blended methods and were face-to-face programs including interactive parts, which are more successful than online programs. Videos, group activities, and case studies relevant to general knowledge about dementia, communication, dementia care, and managing challenging behaviors were the most frequent training characteristics. “Motivation” factors like “participants’ readiness” and “fulfillment of content” are also important for successful learning and implementation. Apart from the exploration of educational needs expectations, caregivers experiences, interviews, discussions, and reflective accounts with and from staff members are always effective, taking into account their experience and perception, which is in agreement with other studies [53].
Some of our results correspond with recent reviews, demonstrating specific features of effective dementia training programs, such as trainings relevant to specific roles and duties in the workplace, learning through group activities/interactive approaches, face-to-face learning, and the development and support of in-service “experts” who facilitate training implementation [18, 54].
Although there is no doubt that PCC approaches are effective in changing the clinical practice [33] with more than half of the studies including person-centered components, in some cases [30, 41], the shift was not strong or PCC was not implemented well, because it presupposes to know the person at a deeper level which needs time. Additionally, organization priorities usually are the rapid diagnosis and therapeutic intervention with short lengths of stay. This highlights the idea that PCC cannot be implemented with a one-off “quick fix” [55] but requires a change in the values of both the acute healthcare system and the individual practitioner [44]. This can be achieved if a “whole system approach” [56] links all the persons concerned, including the PwD, their family members, direct care workers, and administrative and managerial staff. A strategy to this direction is the Appreciative Inquiry approach, used by three studies [30, 40] and was related to organizational development for transformative change.
Dementia champions have been identified as one of the best models for providing higher-quality care in general hospitals. Champion’s role is an attempt to “transfer climate” influencing the “environment” factors of training. Champions promote good practices making them sustainable, and ensure that staff is fully supported to provide PCC [57–59]. Five studies in total included champions in their training programs. Moreover, the use of action plans, can support the sustainability of champion’s role as a change agent in further improving the care of PwD in their practice area [40]. Nevertheless, it has been suggested that while champions may be effective in the early stages of introducing a change in local settings, their influence may become diminished over time as the spread of change goes organization-wide and incorporates different disciplines [60]. Thus, the factor of work environment, cannot be easily influenced [40] suggesting the great impact of the organization in sustainable programs. Moreover, visits by the trainer to continue implementation may not be sufficient [61]. Training providers or stakeholders must find other solutions for long-term implementation such as extending training possibilities to clinical wards and departments [33, 62]. This is in agreement with the fact that workplaces of hospital systems are complex and to transfer learning into practice needs not only supporters but many other organizational, environmental, and cultural factors [5].
Thus, sustainability seems to require more than just a good implementation. The supporting environment/conditions in the frame of strong leadership, care culture, initiative approaches, connections among people including teamwork [29, 30], continuous action, and vision are the most valuable factors for successful implementation [42, 63]. Without continued in-service training and hospital wide changes, the changes achieved through trainings will be short-lived [34]. Dementia trainings cannot solve all the problems of failing services. Thus, limited time, lack of staff or the unpredictable nature of the workload in acute care, lack of financial resources, all appeared to be barriers to sustainable changes [29, 65]. Moreover, bureaucracy [65] and hierarchical culture focused on internal stability, models of working with adherence to rules being resistant to flexibility, innovation, and openness are all factors that make the change difficult in organizations [66]. No matter how good a dementia training is, changes in the organizational level, and a transformation of care culture are imperative for training sustainability over time.
Limitations
This review has some limitations. There was a high heterogeneity of study methods. The inclusion of both quantitative and qualitative study designs made the data extraction and conclusions difficult, but quantitative measurements alone are not always sensitive to changes [67] and some changes are only reflected in qualitative measurements [68]. The bias of the small sample size of participants, the lack of RCTs [33], and discrepancies in evaluation methods [29] further made the conclusions difficult. However, there is still a debate on whether RCTs should be considered as the “gold standard” in health education research [69, 70] because the complexity of health care settings may require simpler solutions or other types of randomization [71]. Furthermore, most of the studies used pre-post measurements immediately after the training making the outcomes suspect or less strong. Participants sometimes overestimate their understanding and perceived behavioral changes are not effectively captured [43]. Thus, the additional lack of follow-up measurements makes it difficult to conclude which programs were successfully in changing long-term clinical practice. Lastly, only articles written in English were included.
Conclusion and future research
This narrative synthesis demonstrates the characteristics and effectiveness of dementia training programs in general hospitals according to Holton’s model. Effective trainings focused not only on individual changes, such as learning and performance, but also on changes on the organizational level. Moreover, PCC approaches, a variation of teaching methods including an interactive face-to-face design, supporting conditions like champions and mentors, and action plans are all invaluable characteristics of effective trainings. In addition, trainings where stakeholders adopted initiatives, plans or care policies to continue systematic changes and foster long-term implementation in the organization or across organizations were more effective.
The high heterogeneity of studies regarding the content and delivery of trainings leads us to make further suggestions for the design of future training programs. Guidance or frameworks such as the Medical Research Council (MRC) for developing complex training interventions are necessary for future interventions [72]. Moreover, trainings must use multi-level evaluations not only among hospital wards, but also across the organization in order to measure the sustainability of changes in learning, staff behavior/attitudes, and clinical practice towards caring for PwD. More follow-up designs and longitudinal evaluations of the programs are required in order to conclude which programs were successfully able to make a difference in long-term clinical practice. Sustainable changes in clinical practices means more than just having well-trained and qualified employees. Dementia staff education should be adapted to specific training goals (raising awareness, train experts, and commissioners) with flexibility in the content, length, and type of intervention.