
Abstract
Our aim was to assess whether in vivo 11C-PIB negative memory-impaired subjects may nonetheless exhibit brain Alzheimer’s disease (AD) pathology. We re-evaluated the PET images and systematically characterized the postmortem neuropathology of six individuals who had undergone clinically indicated amyloid PET. The single case with negligible amyloid-β (Aβ) pathology had Lewy body disease, where concomitant AD changes are often seen. Further, the subject’s plaques were predominantly diffuse. The predictive value of a negative 11C-PIB scan appears to be good, even in memory-impaired populations. Our results suggest that considerable neuritic Aβ plaque pathology in the absence of specific/cortical 11C-PIB binding upon PET is unlikely.
INTRODUCTION
Amyloid imaging with positron emission tomography (PET) has established itself as a supplementary diagnostic tool in the differential diagnosis of Alzheimer’s disease (AD) from other dementias [1]. However, a Cochrane review stressed that it is important to clearly demonstrate its accuracy before it can be widely applied [2]. Another review pointed out that as amyloid deposition is not unique to AD, PET amyloid imaging agents cannot be said to be diagnostic of AD, although they may have utility in excluding it in suspected cases [3].
A number of case reports and studies have assessed correlates of 11C-labeled Pittsburgh Compound B (11C-PIB) and other amyloid fibril binding PET tracer uptake values in postmortem or in vivo biopsy brain tissue [4–19]. PET imaging with these agents has high sensitivity and specificity for the presence of moderate or frequent neuritic plaque densities, but none of them are sensitive enough to reliably detect the presence of sparse neuritic plaques. The amyloid tracers 11C-PIB, 18F-florbetapir, 18F-florbetapen, and 18F-flutemetamol have relatively similar fibrillar Aβ binding site affinities [3]. Robust associations between regional amyloid tracer uptake and neuritic plaque density as well as immunohistochemically measured Aβ have been reported [4–9, 19].
Some studies have also provided sensitivity and specificity estimates for binary visual assessment of amyloid PET images in relation to postmortem brain tissue Aβ detection. For 18F-flutemetamol, they have been 88–91% and 88–90%. respectively [15, 16]. With 18F-florbetaben, sensitivity of 98% and specificity of 89% have been reported [18]. For 18F-florbetapir, the corresponding values for detection of moderate to frequent plaques (as opposed to none or sparse) were 92% and 100% [13]. Overall, false negatives by amyloid imaging do occur, and it still remains unclear whether notable Aβ or other AD pathology could exist in brain tissue when prior in vivo 11C-PIB PET has been negative.
Only a few single case reports [20, 21] have specifically focused on amyloid imaging negativity. One described a subject who underwent 11C-PIB PET as cognitively intact but experienced memory impairment afterwards, and autopsy performed approximately 2.5 years thereafter revealed foci of frequent neocortical diffuse amyloid plaques but only sparse neuritic plaques and neurofibrillary tangles [20]. Another report assessed a subject who had clinical diagnoses of probable dementia with Lewy bodies and possible AD, 11C-PIB PET-scanned 17 months prior to death [21]. Aβ1 - 40 levels in several cortical regions were comparable to the values of an 11C-PIB positive comparison case. The authors concluded that Aβ pathology may be associated with low or undetectable 11C-PIB uptake upon in vivo PET.
Distinct from previous end-of-life and clinically heterogeneous studies, the aim of this study was to specifically address whether individuals with a memory impairment but an 11C-PIB negative clinically indicated amyloid PET scan may exhibit AD neuropathology upon postmortem brain tissue examination.
SUBJECTS AND METHODS
Permission for the study was granted by the research sites according to local legislation. The study plan and the created privacy policy, in line with the Personal Data Act (Finland, 22.4.1999/523), were reviewed and accepted by the national Data Protection Ombudsman.
Subjects
The subjects were identified by screening the list of the deceased who had undergone neuropathological examination at the Turku University Hospital during 2006–2015 and had previously been in a clinically indicated 11C-PIB PET scan at the Turku PET Centre.
Six individuals had been 11C-PIB negative according to visual assessment (see Fig. 1). The images were re-evaluated and 11C-PIB negativity was visually confirmed. The age at imaging ranged from 54 to 81 years, the interval between 11C-PIB PET and death from 15 to 67 months (Table 2). All cases had had subjective memory problems corroborated by their relatives. In addition, cognitive testing (CERAD test or detailed neuropsychological investigation) had been performed for everyone.
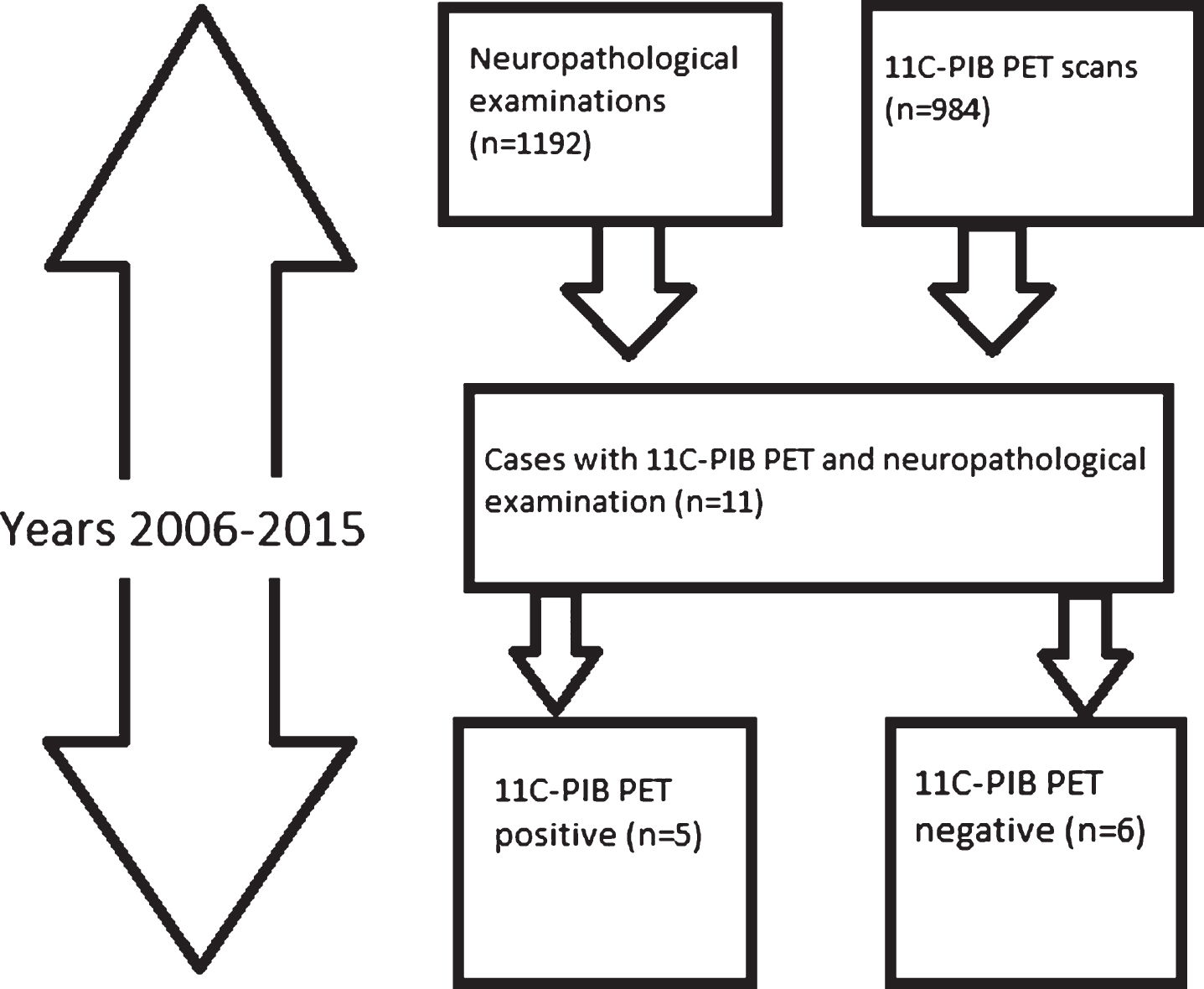
The identification of study subjects. The final sample is in the lower right corner.
Neuropathology
The neuropathological reports and slides were re-examined to determine potential AD pathology. The material included H&E and Bielschowsky silver stainings in sections from a minimum of 12 brain regions. Immunohistochemical stainings for Aβ, phospho-tau, α-synuclein, TDP-43, and p62 were performed using a Ventana Benchmark XT Immunostainer (Ventana Medical Systems, Tucson, AZ). The used antibodies, clones and manufacturers are listed in Table 1. Scoring of AD changes was carried out according to NIA-AA guidelines for neuropathological assessment of AD using the ABC principle [22] with minor modifications, except for one case (#6, Table 2) for whom only the neuropathologist’s report was available. The A stands for Aβ plaque Thal phase [23], B for neurofibrillary stage by phospho-tau staining according to Braak [24], and C for neuritic plaque scoring modified from CERAD [25]. The Neuropathological diagnostic criteria for frontotemporal lobar dementia (FTLD) and FTLD+ motor neuron disease (MND) were used as proposed by the Consortium for Frontotemporal Lobar degeneration [26]. Lewy body disease (LBD) was diagnosed according to guidelines of the DLB Consortium [27, 28].
The antibodies, clones and manufacturers used in the immunohistochemical stainings
Clinical and neuroradiological features and neuropathological findings of the subjects. Subjects #1-2 and #5-6 were female
MMSE, MRI and possible 18F-FDG PET had been conducted close to 11C-PIB PET. All six had exhibited only non-specific white matter 11C-PIB binding in amyloid PET according to visual assessment.
RESULTS
All subjects had been 11C-PIB PET imaged according to appropriate use criteria for amyloid PET [29, 30] or in the case of one subject (#6), as a part of screening for an AD drug trial. Only non-specific white matter 11C-PIB uptake was seen upon image re-evaluation. The Mini-Mental State Examination (MMSE) scores as a proxy for severity of cognitive impairment, as well as the MRI and 18F-FDG PET findings of the subjects, where available, are given in Table 2.
Histologically, two cases had an A0B0C0 and two cases had an A0B1C0 score according to NIA-AA guidelines [22], i.e., the level of AD pathology was considered insufficient to explain cognitive impairment. AD neuropathological changes of level “low” were found in only one (#3) of the six cases. This subject had neuropathological findings diagnostic for LBD, limbic type with concomitant mild AD changes (A1B1C1), meaning that mainly diffuse Aβ plaques were present in isocortical areas. AD neuropathological changes are common in LBD [27, 31]. In retrospect, the medical records of patient #3 had mentions of motor signs of LBD. These had been interpreted as a side effect of decades of antipsychotic agent use. AD had been suspected for the cognitive decline.
The principal pathologies are summarized in Table 2. They include one TDP-43 positive FTLD with mild concomitant α-synuclein pathology, and another case with TDP-43 positive FTLD + MND, and one case of small vessel disease. One patient had no neurodegenerative disease, only acute trauma related findings. This case had several years’ history of progressive memory impairment, verified in neuropsychological testing. The subject died because of a traffic accident and the trauma related changes seen in neuropathological examination are attributable to this. Another (#6) had neurodegenerative findings that were not specific of any neuropathological disease; phospho-tau positive neurofibrillary change was seen in neurons but Aβ immunohistochemistry was negative. This was the case for whom only the neuropathologist’s report was available.
DISCUSSION
To summarize our results, none of the 11C-PIB negative memory-impaired patients had such AD changes upon neuropathological examination that would have been sufficient to explain their cognitive decline. The subjects exhibited no Aβ (n = 5) or a low level of Aβ plaques (n = 1). The single case with any Aβ pathology had LBD, where concomitant AD changes are often seen [27, 31].
In a recent end-of-life PET-autopsy study with 18F-flutemetamol, 7 out of 106 subjects were false negatives by imaging, of whom 4 had unequivocally abnormal Aβ burdens in histopathology. The authors discussed the possibility of severe cortical atrophy being partly responsible for the misclassifications, although they acknowledged that equivalent atrophy was seen in many patients whose images were correctly interpreted [16]. In comparison, only one of our subjects exhibited widespread atrophy (#4). In another end-of-life study, two false negatives by imaging (in relation to having moderate or frequent Aβ plaques as opposed to none or sparse) occurred [13].
Overall, the literature on 18F labeled amyloid tracers and subsequent neuropathology is vaster than that on 11C-PIB, and strong associations between regional tracer uptake and brain Aβ have been reported [8, 32]. However, the associations could be driven mostly by high amyloid tracer uptake and high levels of Aβ in brain tissue. Further, the studies have often been conducted with end-of-life subjects and not necessarily memory-impaired patients. Moreover, the reports have not discussed in further detail the amyloid PET negative subjects.
The one subject with low level AD pathology in our study could suggest that the predictive value of a negative 11C-PIB PET scan is less than perfect. However, this LBD case exhibited mainly immature/diffuse Aβ plaques that are often present even in non-demented elderly individuals [33], and very few core plaques, where 11C-PIB would typically bind. The interval between the PET scan and the autopsy was long (67 months, i.e., 5.6 years) and thus, the plaques may have developed after the amyloid imaging, which has also been suggested for the false negatives in previous studies [13, 16]. Our LBD case is also in line with Aβ being often seen in LBD [27, 31], as well as partly comparable with a previous 11C-PIB positive LBD case report, where greatest tracer retention corresponded with Aβ density in the same regions in postmortem neuropathology, but overall, neocortical neuritic plaques were sparse whereas diffuse plaques were frequent. The subject had low likelihood of AD by NIA-Reagan criteria [14].
Up to 10–30% of cognitively healthy elderly individuals exhibit positive amyloid PET [34–37] and Aβ pathology can be seen in up to 45% or more of elderly healthy subjects. On the other hand, some degree of tangles or tau pathology is universal in elderly subjects [38, 39]. It has not been established whether the former (Aβ) findings mean pending AD; this also motivated us to focus on amyloid PET negativity.
The modest sample size is an acknowledged limitation. Almost 1,000 11C-PIB PET studies had been conducted in 2006–2015 at the Turku PET Centre, but very few of these individuals had gone on to postmortem neuropathological examinations. No end-of-life amyloid imaging studies had been performed at our site during the study period, i.e., only a small proportion of our 11C-PIB PET imaged subjects have deceased to date. Also, as this was a register study, the subjects had not specifically been enrolled for neuropathology. To the best of our knowledge, ours is, however, the largest sample to date, in a study that focuses on the subsequent neuropathological findings of 11C-PIB negative cases in a clinical sample. In one earlier study, a postmortem neuropathological examination was conducted in six individuals with various clinical diagnoses and previous 11C-PIB imaging. Three of the individuals were 11C-PIB negative, and these were later neuropathologically found to have sparse diffuse amyloid plaques or a low amount of dense core plaques. The neuropathological diagnoses were sporadic Creutzfeldt-Jakob disease, Parkinson’s disease dementia, and minimal senile change (the last case being a healthy volunteer) [19]. Granted that the primary objective of that study was to correlate 11C-PIB imaging findings and amyloid plaque density across diverse clinical diagnoses and not in addressing the use of 11C-PIB imaging in the differential diagnostics of suspected AD, we find the results supportive to the conclusions of the present study. Small amounts of amyloid plaques remain undetected by 11C-PIB imaging, but AD is in this setting an unlikely cause for cognitive decline.
As a strength, we were able to characterize the subjects not only in terms of amyloid PET and thorough neuropathology, but also had information on the clinical features, MRI findings as well as 18F-FDG PET data on some of the individuals. Of note, all three patients that had undergone 18F-FDG PET exhibited cortical temporal or temporoparietal hypometabolism, together with negative 11C-PIB suggesting the presence of a non-AD etiology. Another notion pointing in amyloid PET’s added value in investigating clinically undetermined cognitive decline is the fact that some of our subjects also exhibited marked hippocampal atrophy, a cardinal MR imaging feature of AD [40].
Overall, our findings suggest that in clinical settings, when cognitive decline is evident and 11C-PIB PET is negative, efforts should be directed at investigating other less common causes of dementia. This is especially encouraged when the patient is relatively young, as the likelihood of 11C-PIB positivity increases with age [41], and when severe cortical atrophy is not present, as it might preclude correct PET image interpretation [16]. 11C-PIB PET negativity is associated with not having clinically relevant Aβ pathology, and this further validates the use of amyloid PET also in subject stratification in treatment trials targeting Aβ. For instance, in the bapineuzumab (anti amyloid antibody) PET substudy, 6.5% of APOE ɛ4 carriers and 36.1% of noncarriers had a baseline global cortical 11C-PIB average less than the prespecified threshold for amyloid positivity [42]. This could have partly contributed to the negative clinical results. An important caveat should however be remembered: it is still not possible, even with PET amyloid imaging, to reliably detect subjects with sparse neuritic plaques. PET amyloid imaging may thus still not be feasible for selecting subjects at the very earliest stages of Aβ deposition, when anti-amyloid therapy might be expected to be most useful.
Footnotes
ACKNOWLEDGMENTS
The staffs of the Turku PET Centre, Department of Pathology of the Turku University Hospital and of the Welfare Division of Turku City are thanked for their dedicated work and co-operation. The funding for this study was provided by Sigrid Juselius Foundation and the Finnish Governmental Research Funding for Turku University Hospital (ERVA).