
Abstract
The Covid-19 pandemic has highlighted the need to address health literacy as a critical priority for public health. Health literacy is crucial during a pandemic for understanding and following health advice and for navigating vast amounts of information and misinformation. However, public health communication globally has inadequately met the needs of low literacy and culturally and linguistically diverse groups. This review examines the role of health literacy and how it is related to Covid-19 related outcomes, as well as how public health communication has routinely failed to follow basic health literacy principles. Lessons from the pandemic about health communication and recommendations for how health literacy needs can be addressed in the future are discussed. Improving public health communication requires an immediate short-term response and longer-term investment to build the health literacy responsiveness of public health units, health organisations, and government departments to meet health literacy population needs.
Background
The COVID-19 pandemic has led to unprecedented health, social and economic consequences. These were not only considerable, they continue to be unevenly spread, disproportionately falling on those already socially and economically disadvantaged [1]. The data from numerous high-income countries suggest there are important differences in COVID-19 mortality for people from different socioeconomic and cultural and/or linguistic backgrounds [2–5] (Table 1). Much of these differences are attributable to pre-existing social and structural inequalities including limited access to education, healthcare, housing, and employment, exposure to occupational and environmental risk factors, and higher rates of comorbid diseases known to affect COVID-19 symptom severity [1,6,7]. However, health literacy also may have played a role. There is increasing evidence that the extant health information environment poorly met the needs of people with lower health literacy and the same populations showed lower levels of understanding and engagement with COVID-19 health advice.
Racial and ethnic differences in COVID-19 mortality in selected countries
Racial and ethnic differences in COVID-19 mortality in selected countries
Note. It is important to note that racial and ethnic COVID-19 mortalities were generally larger during the earlier waves of the pandemic, reflecting the effect of COVID-19 being disproportionately experienced first among minority ethnic and racial groups. a Selected migrant groups presented with worst COVID-19 outcomes. Large heterogeneity across all migrant groups. b Highest mortality rates seen in Pakistani and Bangladeshi ethnic groups [93]. c Non-Hispanic White.
Health literacy refers to the personal skills and capacities as well as the informational and organisational environment that enables people to find, understand, and use health information and services to manage their health (See Fig. 1) [8,9]. This paper describes the accumulating evidence of the role that health literacy played during the pandemic in the public’s understanding, attitudes, and engagement with COVID-19 public health advice, as well as the health literacy burden created by the informational environment during a crucial time for effective public communication.

Health literacy.
The prevalence of lower health literacy is socio-economically patterned. Low health literacy is consistently associated with markers of social and economic disadvantage, including lower education, lower income, and unemployment. It also is associated with indicators of language fluency and migration, such as lower English fluency in English speaking nations or fluency of the dominant national language of residence [10–15]. As a construct, health literacy has been advanced as a potential mid-stream and modifiable social determinant of health. This means there is potential to improve health outcomes through investment in interventions to build personal health literacy skills and capacities, and in efforts (such as policies, systems, and processes) to reduce the complexity and demand of the healthcare environment to enable better access to health information and services [16].
Health literacy and COVID-19 public communication: a complex health environment
Early in the pandemic, there was pressure to respond rapidly to the COVID-19 outbreak and communicate quickly to the public. Although there are established health literacy principles to guide public health communication - such as ensuring health information is readable and actionable, avoids medical jargon, and uses simple language - these often were not well integrated into communication by government and prominent health organisations [17–23]. This resulted in much of the COVID-19 public health advice being highly complex and requiring a high level of personal health literacy skills.
For example, early in the pandemic (mid-2020), Mishra and Dexter analysed COVID-19 information produced by 15 prominent national and international health websites [19]. They found a very high level of complexity in written government and health organisation texts regarding COVID-19. Mishra and Dexter found written health information did not meet recommended guidelines for reading level grade (e.g. Grade 8 reading age for readers of average population literacy). Instead, the reading grade level exceeded average reading ability ranging from 2–10 grades higher than the recommended grade 8 level. The authors found no resources that were written at the level advised as suitable for people with lower literacy (Grade 6) [19].
In the past three years, there have since been dozens of studies examining the complexity of written health information about COVID-19 [20,24–33]. The authors’ research in July 2021 assessed communication when COVID-19 vaccine communication dominated public communication. It suggested there was little improvement in the readability of written information on official government websites [20].
Of ten websites assessed in July 2021, the median reading grade of the health information was age 12, (four grades higher than the recommended grade 8 level) [20]. Only two sites had resources developed for low literacy readers. While these analyses do not consider infographic and audio-visual communications to the public, they address the written communication provided to the public by major health organisations and governments internationally.
Health literacy and its relationship with COVID-19 understanding, attitudes, and intentions
Health literacy has been linked to a range of knowledge and behavioural outcomes related to COVID-19 (see Box Box 1) [34–39]. Australian research from early in the pandemic (April 2020) suggested people with lower health literacy and those who spoke a language other than English at home had poorer knowledge and understanding of COVID-19 health advice and reported greater difficulty in finding reliable health information. The national survey of >4000 Australian adults suggested the same groups also perceived the risk of COVID-19 as lower and rated COVID-19 prevention behaviours as less important than people with higher health literacy. Similarly, Australians with lower health literacy were less willing to be vaccinated, either for flu or a potential COVID-19 vaccine (note: no COVID vaccine was available in Australia at the time of the study) [40]. There also were important differences in knowledge, attitudes, and reported adherence to COVID-19 prevention behaviours by age and gender, which suggested messaging was not reaching population sub-groups, such as young people and men [39,41].
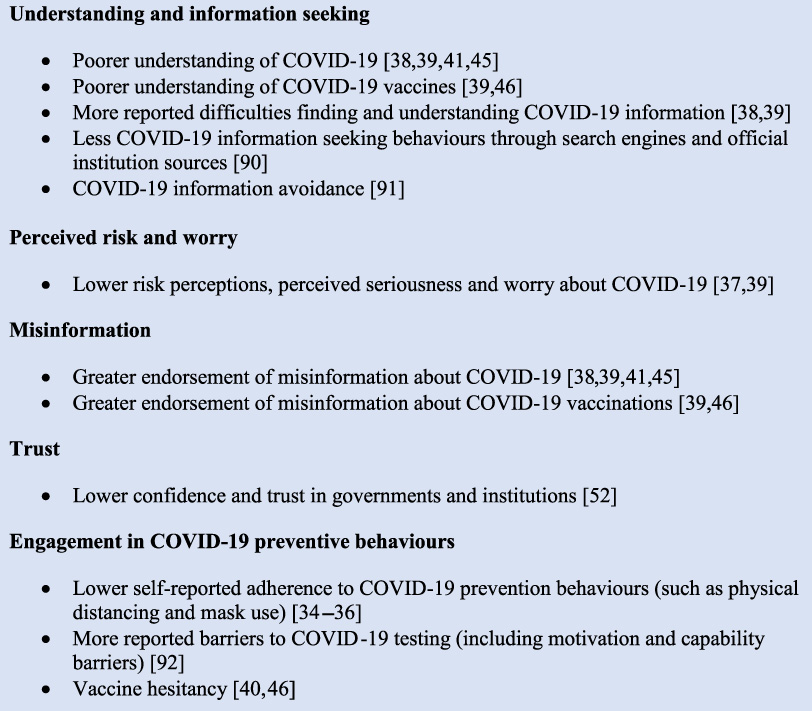
Summary of associations between health literacy and COVID-19 related outcomes.
Research from France around the same period (April 2020) assessed COVID-19 knowledge using a COVID-19-specific measure of health literacy and reported similar findings. Low health literacy was associated with lower self-reported compliance with mask wearing and physical distancing [35]. Research in Germany, also using a COVID-19-specific health literacy measure (HLS-COVID-Q22), identified 15 percent of the population with ‘problematic’ COVID-19 specific health literacy and 34 percent with inadequate levels. They found low COVID-19 health literacy was associated with feeling less informed and more confused about COVID-19 [38].
In the U.S., adults with one or more chronic conditions who had low health literacy, or were African-American and low income, were less worried about COVID-19 and less likely to believe they would become infected. These groups also felt less prepared for an outbreak [37,42]. Similarly, a lower perceived risk of COVID-19 (assessed at the pandemic outset) among people with lower health literacy was associated with a greater likelihood of COVID-19 infection in a subsequent 12-month period. The latter study was conducted at potentially the most risky time to catch COVID-19, before vaccination and evidence-based treatments were widely available [43].
The pandemic also has been characterised by an explosion of online information (an ‘infodemic’) presenting new and formidable challenges for finding reliable COVID-19 information [44]. Skills for thinking critically about health information have become increasingly important as the digital health information environment has transformed.
For example, lower health literacy, numeracy (the ability to understand and use numeric information including probabilities) and analytical thinking, all have been associated with increased endorsement of COVID-19 misinformation beliefs [41,45–49]. In the authors’ Australian research (including three national surveys between April to July 2020), stronger endorsement of misinformation was associated with: younger age, male gender, lower education level, and speaking a language other than English at home. After controlling for these variables, misinformation beliefs were significantly associated with lower levels of health literacy and digital health literacy [39,41].
Another study of younger adults in Australia aged 18–49 years not yet vaccinated (July–August 2021) found up to two thirds of participants agreed with at least one misinformation belief about COVID-19 vaccines. Misinformation beliefs were significantly associated with lower health literacy, lower education, less knowledge about vaccines, lower perceived personal risk of COVID-19, and lower confidence and trust in government and scientific institutions [46].
In aggregate, these findings are similar to a systematic review that investigated COVID-19 conspiracy beliefs from around the world [50]. Across 85 studies, the review found consistent associations between misinformation, education, and income level; with lower education and income associated with higher endorsement of misinformation. Although health literacy is not reported in the review, its socio-demographic measures of disadvantage are commonly associated with lower health literacy [11–15,51].
Health literacy is associated with trust related to the COVID-19 response
Trust in governments, institutions, scientists, and medical researchers are an important correlate of misinformation beliefs and vaccine hesitancy, and vary by health literacy and other markers of social disadvantage and marginalisation [39,45,50,52,53]. The authors’ Australian research across a nationally representative sample showed lower confidence and trust (in scientists, researchers, and medical institutions) were associated with low health literacy [41,54]. Lower trust also was associated with use of non-official information as a leading source of information about COVID-19 [52]. In contrast, U.S. research among a chronic disease cohort found people with low health literacy expressed increased trust in the federal government’s response. However, the study participants perceived they were less prepared for a COVID-19 outbreak and there was no association with trust in vaccines (leading up to their availability) [55].
COVID-19 communication for culturally and linguistically diverse populations
Migrants, people from different cultural and ethnic minority groups, and First Nations populations often have lower levels of health literacy - particularly when there are language barriers, low income, fewer years of education, and experiences of racism and marginalisation within these groups [14,15,55–61]. These same populations also experienced increased COVID-19 infection, hospitalisation, and mortality, and simultaneous high levels of social, psychological, and financial burden during the pandemic [1–7,62]. Many also experienced further racism and xenophobia associated with COVID-19 [63]. As such, it seems imperative to provide culturally safe and appropriate public health communication that is tailored to specific communities’ needs, and assist disadvantage groups that are already marginalized.
The health information environment for culturally and linguistically diverse populations
COVID-19 public health communication in many countries around the world frequently did not meet the needs of cultural and linguistic minorities [22,64]. In Australia, the government released information about COVID-19 in English alone, with translations in other languages coming many weeks later, or sometimes not at all [22,65,66]. Translated COVID-19 health information on government websites was often of low quality and sometimes relied only on automated machine translations so the information was inaccurate or culturally inappropriate [65,67]. Although there were examples of community-based education initiatives, these often were not widespread and may have left people from culturally and linguistically diverse backgrounds vulnerable to low quality or inaccurate health information and misinformation [64,68]. As the pandemic progressed, initiatives to improve the availability of translated and plain language COVID-19 health information increased worldwide, however, this often ignored timely public communication strategies and occurred later than needed [69].
COVID-19 understanding, attitudes, misinformation beliefs and behavioural intentions among culturally and linguistically diverse populations
This inadequacy of the health information environment has led to further marginalisation of culturally and linguistically diverse communities. Poor outcomes including lower knowledge and understanding about COVID-19, negative attitudes and behaviours related to COVID-19, have been observed among different cultural and linguistic groups in many countries, including Australia [37,39,70–73]. In the authors’ Australian national survey, people who spoke another language at home reported: a greater perceived difficulty in finding health information; a lower perceived risk of COVID-19; a lower understanding of COVID-19 prevention behaviours; a higher endorsement of misinformation; and a lower willingness to be vaccinated compared to people who spoke English [40].
Similar patterns additionally vary widely across different communities. A subsequent study of >700 participants whose first language was not English suggested significant variations among different cultural groups regarding COVID-19 knowledge, misinformation beliefs, risk perceptions, interest in testing and vaccination, and diverse patterns of how COVID-19 information is sourced [71]. Health literacy also was associated with increased difficulty accessing easy to understand health information. Evidence from a systematic review suggests higher endorsement of COVID-19 conspiracy beliefs among some racial and ethnic minority groups when this parallels socio-economic disadvantage [50].
Some communities also exhibit a compromised trust in government advice, based on a history of racism in medical research and care, uncertainty about visa status, and a lack of government support for those in precarious or hazardous employment. For instance, whilst Light et al. reported that some Latino Americans trusted COVID-19 vaccines, others worried the vaccines had been manipulated [73]. Fear about attending a vaccine site also was reported due to immigration status as well as concerns about missing work due to short-term vaccination side effects. Together, this body of research highlights why non-tailored mass communication efforts are unlikely to be effective within some communities.
What can we do better in the future?
Improving public health communication requires an immediate short-term response and longer-term investment in building the health literacy responsiveness of public health units, health organisations, and government departments to meet the health literacy needs of the population. In addition, investments in supporting health literacy skill development in the community is imperative.
Short term actions to address health literacy
Efforts are needed to improve public health communication to meet the needs of lower literacy and culturally and linguistically diverse populations, and to do so in a timely, systematic fashion. Below the authors list four evidence-based activities for focused attention to health literacy:
1.
2.
3.
4.
There are numerous guidelines for effective pandemic communication which should be considered alongside health literacy e.g. see: Hyland-Wood et al., West et al., Leask et al. [79–81]. Information must be urgently promoted using diverse mass media channels, including established and emerging social media (e.g. Facebook, TikTok, Twitch) as well as diverse traditional media channels (e.g. radio, TV). The use of appropriate and trusted spokespeople for different communities also is critical and needs to be combined with the aforementioned measures to optimize outreach to diverse communities [82].
Longer term efforts to address health literacy
In the long term, international efforts are required to build health literacy skills and capacities among community members and the health workforce as well as systems and processes for health organisations to embed into practice. This means investing in programs for individuals and communities to build functional, communicative, and critical health literacy including digital and numeracy skills. For the healthcare workforce, enduring efforts need to provide leadership and training in good health literacy communication practices that promote enhanced understanding among diverse healthcare users. For organisations, it means developing policies, practices, and leadership in health literacy to require attention to health literacy as an integral part of business. There is a large and growing literature on interventional strategies to build health literacy in health organisations and services, which supports the development of health literacy among children, community members, patients, and health professionals [83–89].
A systems-based approach is needed
Attention to health literacy is only a start and is unlikely to succeed if it relies on individual behavioural or organisational change alone. For genuine and sustainable improvement across the health sector and beyond, a systems-based approach is needed so health literacy can be systematically and sustainably addressed in crisis situations at speed, as well as an integral part of every-day activities. Sørensen et al. outline a comprehensive framework to build health literacy system capacity [9]. Sørensen et al. identify eight targets for actions including: a health literate workforce; health literate health organisations; health literate data governance; partnerships and intersectoral collaborations; people-centred services based on user engagement; health literacy informed technology/innovation; health literacy investments/financial resource; and health literacy leadership. This recommended approach suggests changes at the micro level among people and professionals, at the meso level among organisations, institutions, markets, and technologies and at the macro level, in policy, political, social values, and priorities.
Conclusion
COVID-19 exposed the inadequacies of many government, health, and community organisations and services to address health literacy and the needs of culturally and linguistically diverse communities. These inadequacies had deleterious consequences on public and individual health during the COVID-19 pandemic. Since health literacy is a modifiable determinant of health, there is a responsibility to address it. The latter means investing in services that meet the needs of people with lower health literacy, especially those from different cultural and linguistic backgrounds.
The efforts to build health literacy will be more successful if they are part of a broader policy to develop strategies to address the structural inequalities that directly impact public health. COVID-19 has shown how all citizens are impacted by each other’s understanding of health and health decisions. As we move forward with an aging society, increasing digitalisation, and disruption of traditional forms of media, we are likely to see increasing climate-related emergencies including further pandemics. In turn, investing in health literacy efforts among organisations and communities may need to be seen more as a first line of defence rather than something desirable to attain.
Footnotes
Declaration of interest statement
JA, DMM, CB, and KJM are directors of a health literacy consultancy (Health Literacy Solutions Ltd, Pty). The company provides health literacy advice to health services/organisations to support increased access to health information for low literacy adults. Any revenue raised is used to support the development of tools to support health literacy document design. No personal income is received by JA, KJM, DMM or CB.
MSW has had paid consultancies, unrelated to this work with Abbvie, Lundbeck, Pfizer, and Sanofi as well as with Luto UK. In addition, he has received institutional grants from Eli Lilly, Merck, Sharpe & Dohme, Pfizer and Lundbeck. MW is also supported by the National Institute on Aging (P30AG059988).
Authors’ contributions
KJM conceived and drafted the manuscript, which was reviewed and edited by all other authors. All authors approved the final version of the manuscript.