
Abstract
Background
Given increasing technology reliance, there is a need for a deeper understanding of individual and community-level comfort with technology as it pertains to basic and more complex healthcare-related skills.
Methods
The objective of this quasi-experimental study was to engage participants in conversations about digital health literacy to facilitate awareness and to compare digital health literacy for community members, healthcare providers, non-clinical navigators, and community health advisors and county coordinators (henceforth referred to as CHAs) in the Deep South (AL, MS, FL). Interactive community conversations on digital health literacy were given in community (n = 16) and clinical (n = 5) settings. Participants completed pre- and post- surveys assessing personal comfort performing technological tasks on a 5-point scale. Mixed models estimated both within- and between-role changes in self-reported comfort.
Results
Of 248 participants, 56% were community members, 18% healthcare providers, 17% CHAs, and 8% non-clinical navigators. Community members had the lowest personal comfort performing every task assessed (all p < .05). In the pre-test, the largest differences in reported personal comfort performing tasks were seen for basic skills including scanning QR codes (mean comfort score: community members 2.7 [SD 1.5] vs. non-clinical navigator 4.5 [1.0], p < .001) and sharing a website (mean comfort score: community members 2.9 [SD 1.6] vs. non-clinical navigator 4.5 [1.0], p < .001). Pre- vs. post-community conversation, community members experienced significant increases in their personal comfort scanning QR codes (β=0.8, 95% CI 0.5–1.0), creating an online account (general use) (β=0.4, 95% CI 0.2–0.6), and using a smartphone (β=0.3, 95% CI 0.1–0.5).
Conclusions
As technological advances continue to be implemented, gaps in digital health literacy must be addressed. Non-clinical navigators may play a future role in teaching patients technology skills.
Introduction
In recent years, there has been a dramatic increase in the use of technology in healthcare, which is changing the landscape of how patients engage with healthcare teams both in and outside the clinic and necessitates comfort with using technology. 1 Even before the rapid shift toward telehealth and digital care associated with the emergence of the COVID-19 pandemic, 2 electronic kiosks were commonly used across care settings for collecting clinical measurements and accessing web-based health services. 3 In addition, since the 2020 publication of the Cures Act Final Rule, which increased patient and provider access to health data, 4 electronic patient portal use has grown substantially.
In a survey of US adults completing the 2022 Health Information National Trends Survey, 3 of 4 respondents reported being offered the ability to access medical records online, an increase of 24% compared to 2020. Furthermore, 4 of 5 of those offered access to the patient portal in 2022 actually used it in the previous year. 5 In addition, numerous interventions are being developed and deployed that leverage technology. Digital health trackers that measure physical activity levels (e.g., steps completed in a day, heart rate monitoring) are commonly used both by individuals to self-monitor their health outside of the healthcare setting and by clinical teams for real-time data to guide care management. 6 For patients undergoing cancer treatment, electronically-delivered surveys used to capture patient-reported symptoms and facilitate proactive management by clinical teams as part of remote symptom monitoring programs have shown decreases in symptom burden and healthcare utilization (ER visits, hospitalization) and increases in quality of life and, in some cases, even survival.7–13 These digital tools are expected to grow in importance over the coming years and a deeper understanding of how patients use technology is critically important.
Despite the potential for both increased access to healthcare through technology and downstream improvements in patient outcomes based on technology-based interventions, the pace of technology integration may pose a substantial threat to health equity. 14 There is a known digital divide first-level gaps in infrastructure, second-level gaps in skills, and third-level lack of equal benefits to participants from digital tools. 1 In a large study of older adults in California, access to the internet, ability to use the internet, and ability to email differed by race and ethnicity. Furthermore, Black and Latino patients were less likely than White patients to utilize the patient portal. 15 In addition, even when access is available, many individuals lack the requisite skills to engage with technology to access electronic health information and patient resources, a concept known as digital health literacy. 16
Furthermore, low digital health literacy disproportionately impacts under-resourced patients. 17 At the University of Alabama at Birmingham (UAB) and University of South Alabama Mitchell Cancer Institute (MCI), Black patients with cancer were more likely than White patients with cancer to decline participation in our digitally-based remote symptom monitoring program. This raised concerns among our patient navigators that technological barriers may have played a role in the inability to engage patients in the program. 18 Ultimately, the inequitable uptake and application of tools and interventions that rely upon technology could exacerbate existing health disparities if attention is not given to improve all patients ability to benefit from these interventions.
Lack of comfort with technology in healthcare is a barrier that is unlikely to be solved with a single solution. It is important to recognize that digital health literacy includes the amalgamation of both digital literacy (ability to use technology) and health literacy (the ability to use health information and resources). 19 As such, foundational technological skills, including use of smart phones and tablets, sending and receiving emails, and using internet search engines, may be needed prior to the uptake and use of more complex technological skills, such as navigating appointments and test results within a patient portal. The availability of trained individuals who can teach these skills to patients may vary across healthcare settings. Additionally, patients may be uncomfortable requesting or receiving help from others to overcome technological barriers.
Given the increasing reliance on technology in healthcare, there is not only a need for a deeper understanding of individual and community-level comfort with technology as it pertains to both basic and more complex healthcare-related skills, but there is also an important need to identify individuals within communities who can help bridge the technological divide emerging in contemporary society. We hypothesize that differences would be observed between community members and health care teams in personal comfort levels with technology, perceptions of community comfort, and comfort teaching technology skills. In order to begin to understand community needs, resources, and ability to improve comfort with technology, an evaluation of differences in comfort levels across healthcare teams and communities is needed to be able to meet people where they are. The objective of this study was to engage participants in conversations about digital health literacy to raise awareness and to assess the level of comfort with various foundational technological skills of community members and healthcare teams in the Deep South, as well as changes in personal comfort and comfort teaching technological health-related skills after participation in an interactive skill-building and digital health literacy-focused community conversation.
Methods
Study design
This quasi-experimental study, conducted from August 2023 to April 2024, examined reported comfort levels with foundational technological skills for community members, healthcare providers (including nurse navigators), non-clinical navigators, and community health advisors (CHAs) serving individuals living in the Deep South, which included participants predominantly from Alabama, Mississippi, the panhandle of Florida. The groups were compared to understand differences in comfort in order to prepare for future intervention tailored to each group. This pragmatic design was selected to facilitate participant engagement in digital health literacy conversations and minimize participant burden. These skills included sending your care team a message on your patient portal, viewing medical test results on your patient portal, viewing upcoming appointments on your patient portal, logging into your patient portal, filling out a survey online, scanning QR codes to access a website, searching online for health-related information, using google or other search engines, sending an email, reading an email, sharing a website link, using social media, creating an account (username and password) on a website, connecting to the Internet/Wi-Fi, using an iPad or Tablet, using a Smartphone, and using a Computer. Additionally, this study assessed the change in personal comfort by using and teaching relevant technological skills (filling out a Survey Online, scanning QR codes to Access a Website, searching Online for Health-Related Information, using Google or other Search Engines, creating an Account (Username and Password) on a Website, and using a Smartphone) after engaging in a community conversation focused on digital health literacy. This study was approved by the UAB Institutional Review Board (IRB-300010079).
Intervention: digital health literacy community conversations
Development: This project was initiated due to recognition of digital health literacy challenges related to patients with cancer who were asked to participate in remote symptom monitoring using a technology interface at UAB and MCI and subsequent recognition of gaps in basic digital skills. The community conversation was developed by a team of individuals with experience in oncology, public health, education, anthropology, and community engagement in partnership with a community organization, the Cancer Awareness Network. This community partner provides education about telehealth and computer literacy skills for seniors, with a focus on supporting patients with cancer. The content was informed by literature review, as well as interviews with community health advisors exploring perspectives related to technology use and digital health literacy. The topic areas for the community conversation included (1) defining digital literacy, health literacy, and digital health literacy; (2) examples of technology in healthcare and its impact on patient outcomes; (3) equity concerns and identification of at-risk populations; (4) teaching participants how to scan a QR code as an example of how an individual might teach another person a technology skill; and (5) strategies to address digital health literacy barriers for patients within the healthcare system.
Setting: This initiative targeted communities served by UAB and MCI's cancer centers. These institutions are the only two academic cancer centers in Alabama and they serve large populations of Black or African American patients (>25% at each institution). A total of 21 community conversations were hosted in clinical settings (n = 5) or in community-based locations (n = 16), such as schools, community centers, and libraries in conjunction with the Cancer Awareness Network. Clinical setting participants included physicians, nurses, navigators (nurse and non-clinical individuals working in a clinic-based setting), social workers, medical assistants, and administrators. In the community setting, participation was open to any community member but targeted Black individuals and older adults through engagement with the Cancer Awareness Network which prioritizes the needs of the Black community.
Recruitment: For the community conversations within healthcare settings, the Principal Investigators approached senior leadership within participating cancer centers (e.g., manager, administrative directors, community outreach leadership), who invited clinical staff and community members with established relationships to the health center via email to participate. Invitations were made at the discretion of the health system leadership. For the community conversations, participants were either affiliated with the UAB Office of Community Outreach and Engagement, MCI Cancer Control and Prevention Division, or the Cancer Awareness Network. Individuals participating in a community conversation who were older than 18 years old were eligible to participate in this study. Otherwise, there were other exclusion criteria. A waiver of written informed consent was obtained as survey completion implied consent.
Delivery: The community conversation was facilitated using a slide presentation (similar across all lectures) by a UAB research staff member (KH) originally from a rural Alabama community with a master's degree in public health. All community conversations lasted approximately 1 h and were conducted in-person, with some also including a virtual option to participate based on the availability of a virtual option for clinical settings. No incentives were provided, and food was made available at some locations if the conversation occurred during mealtime.
Outcome: evaluation of digital health literacy
Surveys were administered pre- and post-digital health literacy community conversations, via paper hardcopy for those in-person and digitally via REDCap 20 for those participating virtually. Pre-community conversation surveys included 17 items assessing technological health-related skills, such as logging into a patient portal or searching online for health-related information. Respondents self-reported their comfort with each of these 17 tasks within three domains (51 items in total): (1) personal comfort in performing, (2) personal comfort in teaching, and (3) perception of comfort for community members within their respective counties. The research team generated these tasks to include common technology tasks used both in general and specifically for interacting with members of the healthcare team. Comfort levels were rated on a 5-point Likert scale (not at all comfortable, slightly comfortable, somewhat comfortable, moderately comfortable, completely comfortable). Six of the 17 items assessing technological health-related skills were repeated on the post-community conversation survey as they assessed the technological health-related skills included in the community conversation. Respondents self-reported their comfort with each of these 6 tasks within two domains on the post-survey (12 items in total): (1) personal comfort performing, and (2) personal comfort teaching.
Other study-specific survey items assessed respondent satisfaction with home internet connection for health-related needs, confidence in their ability to find health resources online, confidence in their ability to differentiate between trustworthy and non-trustworthy health information online, and thoughts about how much health information online is false or misleading (none, a little/some, a lot). Satisfaction and confidence levels were rated on a 5-point Likert scale and grouped into three categories (extremely/very, somewhat, and not very/not at all). Surveys also collected respondent demographic information (age, sex, race, education level) and professional or personal role, including community member (includes patient advocate), healthcare provider (nurse navigator or nurse, advanced practice provider, social worker, physician), lay (non-clinical) navigator or coordinator working in a healthcare setting, or CHA; (community health advisors, county coordinators, community health workers), as we were interested in differences between participants. All surveys were completed on the same day as the intervention with instructions about the survey prior to the community conversation and post-survey administered immediately following completion of the lecture.
Statistical analysis
Respondent demographic characteristics and health-related internet access satisfaction and confidence in online resources were reported as medians and interquartile ranges (IQR) for continuous measures and frequency and percentages for categorical measures. Mean (standard deviation [SD]) comfort with technological skills was reported by role within each of the three domains of (1) personal comfort performing, (2) personal comfort teaching, and (3) perception of comfort for community members within their respective counties. Differences in mean reported comfort with technological health-related skills were compared by role using one-way ANOVA tests. Marginal means, beta estimates (β), and respective 95% confidence intervals (CI) from repeated measures mixed models with a random intercept were used to assess both within- and between-role changes in reported comfort with technological health-related skills pre- and post-digital health literacy community conversation. Models were adjusted for respondent age, sex, race, and education level. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
No formal power calculation was completed as the sample for this study was based on the number of participants attending events. The number of events was selected based on availability of community partners during this time-period.
Results
Study sample and characteristics
Twenty-one community conversations on digital health literacy were held; 248 participants in total completed the pre-community conversation survey. With a median age of 68 (IQR 57-73), the sample was majority female (91%), Black, or a person of color (83%), with an associate's degree or higher (75%; Table 1). Over half of the respondents were community members (56%), 18% were healthcare providers, 17% were CHAs, and 8% were non-clinical navigators. Community members (median age 70, IQR 66-76) and CHAs (median age 66, IQR 53-71) were more often older than healthcare providers (median age 56, IQR 36-69) and non-clinical navigators (median age 55, IQR 35-68). Healthcare providers were more often white (48%) compared to CHAs (7%), community members (10%), and non-clinical navigators (25%). Healthcare providers (69%), non-clinical navigators (65%), and CHAs (47%) were more often college-educated compared to community members (27%).
Pre-lecture survey respondent sociodemographic characteristics by role (N = 248).

N = a230, b246, c247, d244, e245, f243.
Health-related internet access satisfaction and confidence in online resources
Non-clinical navigators (84%) and healthcare providers (67%) more often reported being extremely or very satisfied with their home internet for health-related needs compared to community members (45%) and CHAs (44%; Table 1). Similarly, non-clinical navigators (68%, 61%) and healthcare providers (66%, 60%) more often reported being extremely or very confident in their ability to find health resources online and to differentiate between trustworthy and non-trustworthy health information online compared to community members (47%, 33%) and CHAs (56%, 44%), respectively. Finally, one in three healthcare providers (33%) reported there being a lot of false or misleading health information online compared to one in five community members (20%) or CHAs (17%), and 5% of non-clinical navigators.
Comfort with technological health-related skills
Overall, respondents reported they were personally most comfortable with reading an email (mean [SD] comfort levels: non-clinical navigators 4.8 [0.6], healthcare providers 4.5 [0.9], CHAs 4.3 [1.2], community members 3.8 [1.4]) and using Google or other search engines (non-clinical navigators 4.7 [0.8], healthcare providers 4.4 [1.1], CHAs 4.3 [1.1], community members 3.6 [1.4]; Figure 1A). Respondents reported feeling the most comfortable teaching others how to read an e-mail (mean [SD] comfort levels: non-clinical navigators 4.8 [0.4], healthcare providers 3.8 [1.4], CHAs 3.7 [1.5], community members 3.3 [1.6]), as well as how to send an e-mail (non-clinical navigators 4.8 [0.4], healthcare providers 3.8 [1.4], CHAs 3.7 [1.5], community members 3.2 [1.6]; Figure 1B).

Baseline personal comfort performing technological health-related skills by role.
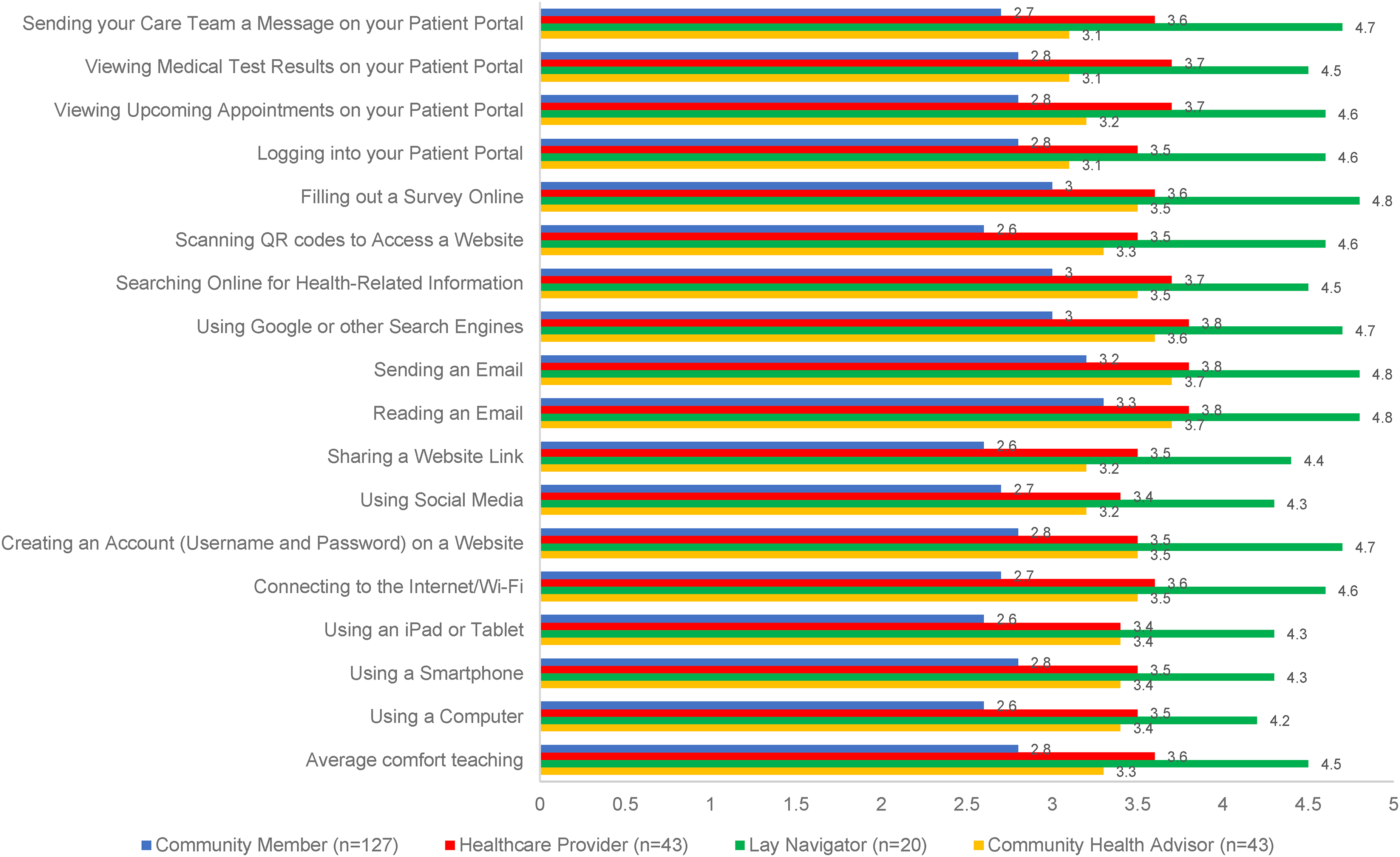
Personal comfort teaching technological health-related skills by role.
Conversely, community members and healthcare providers reported personally feeling the least comfortable with scanning QR codes (general use) to access a website (mean [SD] comfort levels: 2.7 [1.5] and 3.9 [1.7], respectively), while CHAs felt the least comfortable with using social media (3.6 [1.3]). Though non-clinical navigators reported high personal comfort levels with all technological skills assessed, their lowest scoring comfort level was with sending their care team a message on the patient portal (4.4 [1.2]). With respect to comfort teaching technological skills, community members felt the least comfortable teaching others how to use a computer or iPad/tablet, how to share a website link, or how to scan a QR code to access a website (mean comfort levels of 2.6 for all). CHAs were least comfortable teaching others how to use their patient portal, including how to view upcoming appointments or medical test results, or sending their care team a message (mean comfort levels of 3.1 for all). Healthcare providers were least comfortable teaching others how to use an iPad/tablet or social media (mean comfort levels of 3.4 for both). While generally very comfortable teaching others, non-clinical navigators reported the least comfort with teaching others how to use a computer (mean comfort levels of 4.2 [SD 1.1]).
When assessing differences in comfort with technological health-related skills by role (Supplemental Tables 1–3), non-clinical navigators reported the highest comfort and community members the lowest comfort both personally and with teaching every skill assessed (Figures 1A–B; all p < .05). The largest differences in reported personal comfort were seen for scanning QR codes to access a website (mean comfort levels of 4.5 [SD 1.0] for non-clinical navigators vs. 2.7 [1.5] for community members) and sharing a website link (mean comfort levels of 4.5 [1.0] for non-clinical navigators vs. 2.9 [1.6] for community members). The largest differences in reported comfort teaching were seen for sending their care team a message via the patient portal (mean comfort levels of 4.7 [0.6] for non-clinical navigators vs. 2.7 [1.6] for community members) and scanning QR codes to access a website (mean comfort levels of 4.6 [0.8] for non-clinical navigators vs. 2.6 [1.6] for community members).
Perceptions of community comfort with technological health-related skills
Overall, those with prior healthcare engagement (providers, non-clinical navigators, CHAs) perceived their community's comfort with the majority of technological skills to be higher than community members’ evaluation of the comfort that would be found within their communities (Figure 1C). Healthcare providers and CHAs had similar perceptions of the community comfort with technology overall (mean [SD] comfort levels: 2.8 [0.9] and 2.9 [1.2], respectively), which was modestly lower than the estimations by non-clinical navigators (3.3 [0.8]) and the reported personal comfort of the community members themselves (3.2 [1.3]).

Perception of comfort with technological health-related skills for community members within their respective counties by role.
Change in comfort with technological health-related skills
Of pre-community conversation survey respondents, 86% (N = 214) completed both the pre- and post-community conversation survey (Table 2). Compared to those completing both surveys, respondents who completed the pre-community conversation survey only were more often community members (76% vs. 53%), Black or a person of color (94% vs. 81%), and lower educated (41% with less than high school education or high school degree vs. 23%; Supplemental Table 4).
Pre- and post-lecture survey respondent sociodemographic characteristics by role (N = 214).
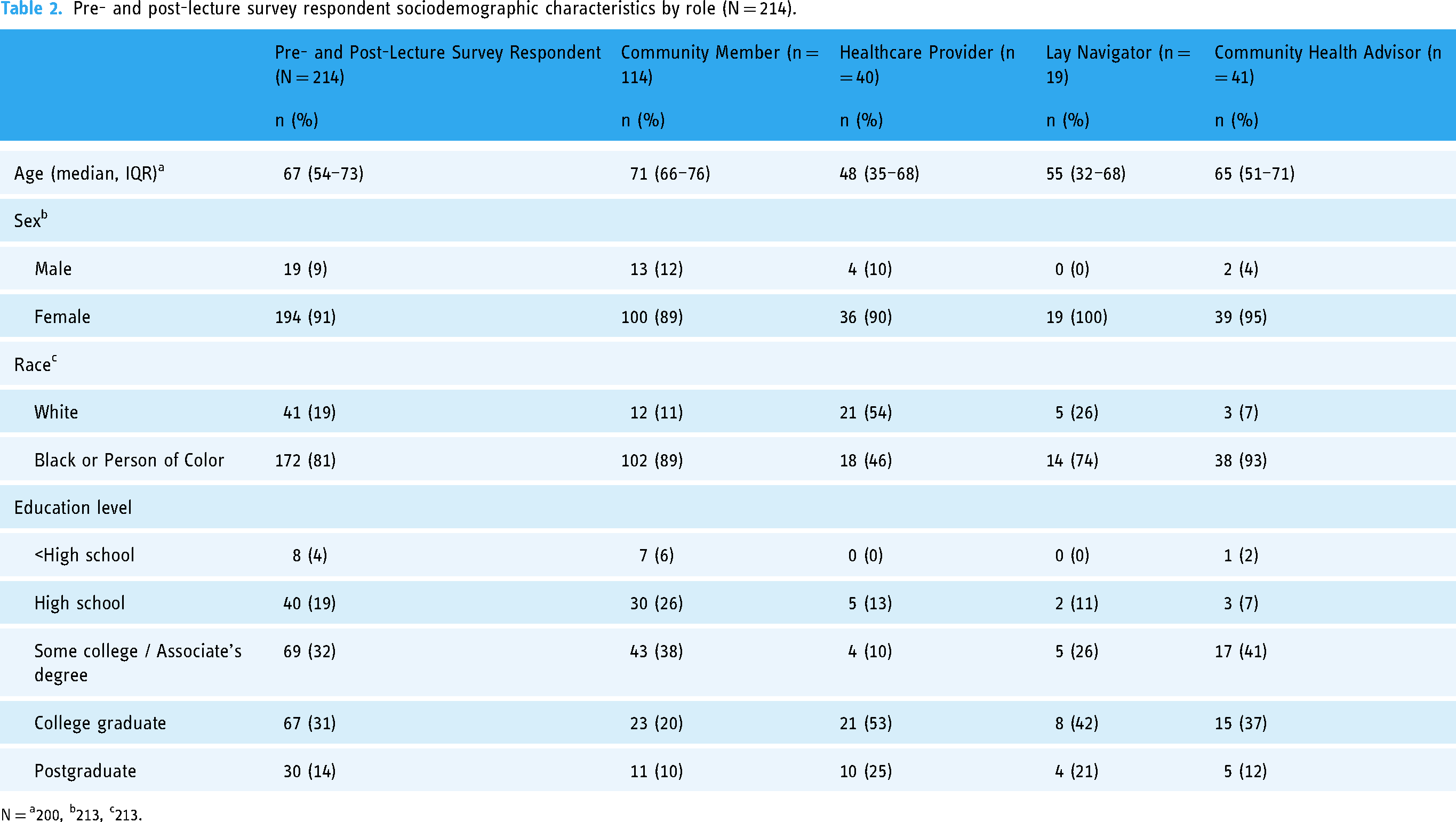
N = a200, b213, c213.
After the community conversation on digital health literacy, the majority of respondents increased their personal comfort with technological health-related skills (Figure 2A). Community members experienced significant within-role increases in their personal comfort scanning QR codes to access a website (β=0.8, 95% CI 0.5–1.0), creating an account on a website (β=0.4, 95% CI 0.2–0.6), and using a smartphone (β=0.3, 95% CI 0.1-0.5; Supplemental Table 5a). When comparing change in comfort scores between roles, community members also experienced significantly greater increases in their personal comfort scanning QR codes to access a website compared to healthcare providers (β= −0.7, 95% CI −1.2- −0.2) and CHAs (β= −0.5, 95% CI −1.0- −0.02; Supplemental Table 5b).

Change personal comfort performing technological health-related skills.
While the majority of community members, healthcare providers, and CHAs also increased their comfort teaching technological health-related skills post-community conversation, non-clinical navigators felt less comfortable across all assessed skills (Figure 2B). Non-clinical navigators experienced significant within-role decreases in their comfort teaching others how to fill out a survey online (β= −0.8, 95% CI −1.3- −0.3), create an account on a website (β= −0.6, 95% CI −1.1– −0.1), and using Google or other search engines (β= −0.6, 95% CI −1.1- −0.2; Supplemental Table 6a). Conversely, community members and healthcare providers experienced significant within-role increases in their comfort teaching others how to scan a QR code to access a website (β=0.6, 95% CI 0.3-0.8 and β=0.5, 95% CI 0.1-0.8, respectively) and use a smartphone (β=0.3, 95% CI 0.1-0.5 and β=0.4, 95% CI 0.01-0.7, respectively). CHAs also experienced significant within-role increases in their comfort teaching others how to fill out a survey online (β=0.5, 95% CI 0.1-0.8). When comparing the change in comfort scores between roles, non-clinical navigators also experienced significantly greater decreases in their comfort teaching others all technological health-related skills assessed compared to community members, healthcare providers, and CHAs (Supplemental Table 6b).

Personal comfort teaching technological health-related skills by role (N = 198).
Discussion
This study considers the reality of implementing technology-based interventions within the Deep South. It identifies the gap in technology comfort for members of the community and healthcare teams, which will be critical to address in order to maximize the benefits available in the digital era related to technology. At the same time, it is important to recognize these gaps also include basic, foundational technology skills such as using smart phones, leveraging QR codes, and communicating via email. Healthcare teams need to consider how to not only include basic training on how to use its healthcare system's patient portal to improve comfort in using technology in healthcare, but also consider broad training that includes many of the tasks assessed in this study. Further, they must learn how to maximally leverage members of the teams such as non-clinical navigators who are poised to educate patients on digital health literacy.
In this study, healthcare providers, CHAs, and non-clinical navigators showed higher personal comfort with both general and healthcare-related technological tasks compared to community members. While the intervention was brief, we hypothesize that the engagement with other participants and time spent thinking about digital health literacy enhanced the comfort considering key task. One contributing factor may be the structured training that they have received to become a CHA and non-clinical navigator which includes a curriculum that builds capacity and empowers community/non-clinical individuals to engage with healthcare providers differently from those who have not gone through this prescribed training. Furthermore, healthcare providers have advanced degrees required at part of their employment and use digital healthcare tools as part of their daily practice. 21 Higher education levels are known to correlate higher health literacy, digital literacy, and digital health literacy.16,22,23 Additionally, healthcare providers are less likely to be of marginalized populations (e.g., Black, Hispanic, Native American) than the population at large. According to the American Association of Medical Colleges (AAMC), only 5% of physicians are Black and 5.8% are Hispanic. 24 This compares to the US Population where 13.7% and 19.5% of the population are Black and Hispanic, respectively. 25 Furthermore, low digital health literacy disproportionately impacts marginalized populations. 17 In a large study of older adults, Black and Latino patients were less likely than White patients to utilize the patient portal. Access to the internet, ability to use the internet, and ability to use email differed by race and ethnicity. 15 Thus, both education and experiences with technology in healthcare may contribute to healthcare providers underappreciating the challenges others face with technology-based healthcare tools.
The impact of the health system and community conversations varied by group. The community members had the lowest pre-community conversation comfort and had the greatest improvement, narrowing the gap between the community members and the other groups. This suggests that dialogue, raising awareness, and skill building (components of the community conversations) are strategies that may empower community members. In contrast, the healthcare team started at a higher comfort level and saw minimal change, potentially due to already having baseline technology skills. For this group, rather than learning the specific skills, it likely is more important to recognize challenges with digital health literacy and the importance of technological skill building in the communities they serve. 26
Within this study, the non-clinical navigators not only felt the most comfortable with technology, but also reported feeling the most comfortable teaching technological skills. This may be secondary to the younger age of this group, given that younger age is correlated with better digital health literacy. 16 The non-clinical navigators also had the best estimates of community member's comfort with technology skills. This group represents an important workforce to educate patients about how to use technology, a task that aligns with a key non-clinical navigator role of helping patients overcome non-clinical barriers to healthcare. 27 Notably, non-clinical navigator comfort with teaching technological skills declined after the community conversations, whereas it increased for other roles. This is suspected to be related to both increased awareness of gaps in skills within the community and the non-clinical navigators developing an increased appreciation for the challenge in teaching others (as was done within the community conversation). We believe additional training is needed for non-clinical navigators to increase their ability to teach patients a broad array of technology skills. Provision of technology support has the potential for substantial impact, as Nejati et al. found that better digital health literacy was associated with trust in the healthcare system, communication, self-efficacy, and shared decision-making. 28
This study has limitations. The study used convenience sampling, recruiting participants from specific community organizations and clinic settings, focusing on a specific geographic region in the US, and our sample of community members was predominantly Black, thus findings may not capture the entire target population and are not generalizable. Additionally, the self-reported comfort levels are subjective and prone to bias, and using a greater number of survey instruments and more objective measures of digital health literacy would strengthen the findings. The intervention was also brief and is likely less effective than interventions that span longer time periods. Moreover, the post-community conversation survey administered immediately after the intervention may also result in bias, and longer-term follow-up to assess sustained levels of comfort would be beneficial.
Conclusion
As technological advances continue to be developed and implemented in healthcare, gaps in digital health literacy, particularly in the Deep South, can be exacerbated among community members. Baseline technology skills must be addressed as healthcare increases reliance on technology. Non-clinical navigators may play a future role in teaching patients the technology skills that are needed to fully access available healthcare services, but they will need additional support to recognize and address digital health literacy challenges.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-3-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-4-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-5-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-6-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-7-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-7-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Supplemental Material
sj-docx-8-dhj-10.1177_20552076251325581 - Supplemental material for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study
Supplemental material, sj-docx-8-dhj-10.1177_20552076251325581 for Exploration of digital health literacy among community members and healthcare teams in the deep south: A quasi-experimental study by Gabrielle B Rocque, Nicole L Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I Chu, Connie C Shao, Claudia Hardy, Timiya S Nolan, Chelsea McGowan, Jennifer Young Pierce and Courtney P Williams in DIGITAL HEALTH
Footnotes
Contributorship/author contributions
Conception and design: Gabrielle B. Rocque, Nicole L. Henderson, Stacey Ingram, Courtney P. Williams, Jennifer Young Pierce, Daniel Chu, Claudia Hardy Administrative support: Gabrielle B. Rocque, Nicole L. Henderson, Stacey Ingram, Courtney P. Williams Provision of study materials or patients: Gabrielle B. Rocque, Keyonsis Hildreth, Loretta Herring, Stacey Ingram Collection and assembly of data: Keyonsis Hildreth, Loretta Herring, Omari Whitlow Data analysis and interpretation: Gabrielle B. Rocque, Nicole L. Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I. Chu, C. Shao, Claudia Hardy, Timiya S. Nolan, Chelsea McGowan, Jennifer Young Pierce, Courtney P. Williams Manuscript writing: Gabrielle B. Rocque, Nicole L. Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I. Chu, C. Shao, Claudia Hardy, Timiya S. Nolan, Chelsea McGowan, Jennifer Young Pierce, Courtney P. Williams Final approval of manuscript: Gabrielle B. Rocque, Nicole L. Henderson, Keyonsis Hildreth, Noon Eltoum, Omari Whitlow, Loretta Herring, Stacey Ingram, Daniel I. Chu, C. Shao, Claudia Hardy, Timiya S. Nolan, Chelsea McGowan, Jennifer Young Pierce, Courtney P. Williams
Consent to participate
Consent for participation was waived by the UAB Institutional Review Board.
Consent for publication
Not applicable
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
This study received ethical approval from the UAB IRB (approval #300010079).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the American Cancer Society Navigation Capacity-Building Initiative Grant (#85751). We would like to acknowledge support for Dr Henderson on the Cancer Prevention and Control Training Program Grant, NIH T32 (CA47888), Dr Eltoum is supported by grant T32HS013852 from the Agency for Healthcare Research and Quality (AHRQ) and Mr Whitlow with the RACE21 Program (R25-CA244092). We also would like to acknowledge the O’Neal Comprehensive Cancer Center (P30 CA013148).
Cancer Prevention and Control Training Program Grant, NIH T32, Agency for Healthcare Research and Quality, American Cancer Society, RACE21 Program, O’Neal Comprehensive Cancer Center, (grant number CA47888, T32HS013852, 85751, R25-CA244092, P30 CA013148).
Guarantor
Gabrielle B. Rocque
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.