
Abstract
BACKGROUND:
Scapular dyskinesis (SD) is a modification of the positioning and movement of the scapula and is associated with shoulder pain. Exercises to strengthen the shoulder and scapular muscles have been proposed as a therapeutic strategy to reduce pain and improve function.
OBJECTIVE:
We aimed to investigate the electromyographic activity of the periscapular and trunk muscles in individuals with shoulder pain and SD in different multi-joint exercises.
METHODS:
Thirty-two subjects with subacromial pain, of both sexes, with the presence or absence of SD, participated in this study. Volunteers performed five repetitions in five exercises (Closed Row; Pronated Row; Push-up; Scapular Push-up; T-push-up). The activity of the upper trapezius, middle trapezius, lower trapezius, serratus anterior, external oblique, and rectus abdominis muscles was recorded using electromyography.
RESULTS:
Our results showed a decrease in the electromyographic activity of the serratus anterior and external oblique during the T-push-up exercise in individuals with shoulder pain and SD. No differences were observed between groups for the trapezius and the rectus abdominis.
CONCLUSIONS:
Rehabilitation programs may initially prioritize rowing and push-up exercises to strengthen periscapular muscles. More complex exercises with greater mechanical demand on the kinetic chain, such as the T-push-up, may have to be implemented in later phases.
Introduction
Subacromial pain represents a critical musculoskeletal complaint in the adult population that affects 44 to 65% of people with shoulder pain [1]. This condition is often associated with withdrawal from work activities, decreased productivity, and increased costs with health services consumed [2, 3, 4]. Several aspects have been highlighted as factors that may increase the risk of developing subacromial pain, including scapular dyskinesis [5, 6].
Scapular dyskinesis is characterized by modification of the positioning and movement of the scapula [5]. Although scapular dyskinesis is associated with shoulder pain, it is unclear whether it is the cause or consequence of shoulder pain [6]. Although more evidence is needed to confirm a possible cause-and-effect relationship, several studies have reported that individuals with shoulder pain have decreased superior rotation and posterior tipping of the scapula, often associated with increased electromyographic (EMG) activity of the upper trapezius (UT) and reduced EMG activity of the serratus anterior (SA), lower trapezius (LT), and middle trapezius (MT) [7, 8, 9]. However, these kinematic and EMG changes are almost always observed when raising and lowering the arms. There is a knowledge gap in possible differences in EMG activity during exercises frequently used in rehabilitation programs.
Exercises that aim to correct the positioning of the scapula and strengthen the shoulder girdle’s stabilizing muscles have been proposed as a therapeutic strategy to reduce pain and improve functionality in individuals with shoulder pain [10, 11]. Specifically, for the periscapular muscles, different push-ups, and rowing exercises have been used to strengthen the SA and parts of the trapezius and rhomboids, respectively [12, 13]. These multi-joint exercises with axial load provide increased muscle coactivation, proprioceptive stimuli, and neuromuscular demand in different muscle groups, including abdominal muscles [12, 13].
Some studies have recently demonstrated that there seems to be a relationship between the EMG activity of the periscapular and abdominal muscles [14, 15] and that asymptomatic subjects with scapular dyskinesis have decreased EMG activity of the abdominal, SA, MT, and LT muscles [16, 17, 18, 19, 20]. However, the differences in muscle activity in people with subacromial pain and scapular dyskinesis during the performance of variations of rowing and push-up exercises are still poorly explored. In addition, knowing the level of EMG activity and identifying whether there are differences in muscle function during movements can help in the prescription and progression of rehabilitation programs for individuals with shoulder pain and scapular dyskinesis.
Therefore, this study investigated the EMG activity of the periscapular and trunk muscles in individuals with shoulder pain and scapular dyskinesis in different multi-joint exercises. Thus, our study hypothesizes that people with shoulder pain and scapular dyskinesis have decreased EMG activity of the abdominal muscles, MT, LT, and SA, compared to people without dyskinesis.
Materials and methods
Sample
Thirty-two subjects with subacromial pain, of both sexes, with the presence (sixteen) or absence (sixteen) of scapular dyskinesis participated in this study. All volunteers were recruited from university campus students and staff. Participants were considered eligible for the study if they presented shoulder pain with intensity
Anthropometric and pain intensity assessment
Anthropometric measurements (body mass andheight) were performed according to the International Society for the Advancement of Kinanthropometry (ISAK) standardization [22]. At baseline, the participants’ present pain intensity was evaluated using the Numeric Pain Rating Scale (NPRS) [23]. They were instructed to report the NPRS score with the arms resting at the body’s side. In this study, only participants with an intensity of pain lower than three points were included. A previous study suggested that pain
Scapular dyskinesis evaluation
Scapular dyskinesis was evaluated by the observational method. The volunteer was asked to remain in the orthostatic position and perform eight repetitions of the bilateral arm elevation movement in the scapular plane to the maximum possible amplitude, with dumbbells approximating 3% of body weight. The execution of the movement was recorded in posterior view by a 60 Hz sampling frequency digital camcorder (SONY model DCR-SX21), positioned on a tripod with a height of 1.00 meters from the ground and two meters from the volunteer.
Two orthopedic physiotherapists performed all evaluations independently. The categorization of the type of scapular dyskinesis was performed according to Rossi et al. [25]. Volunteers were divided into the “YES” category, which considers all partners of scapular asymmetry and dysrhythmia, and the “NO” category, which considers the symmetric scapular motion. Asymmetry assumes the prominence of the inferior angle of the scapula, an increase in medial border prominence, and excessive elevation of the upper angle. All volunteers classified as “NO” were included in the SP group. Volunteers classified as “YES” were included in the dyskinesis group.
Surface electromyography
Electromyography was performed using an EMG800C-1632 signal acquisition system (bandwidth, 16–500 Hz; CMRR, 80 dB; input impedance exceeding 1000x; 16 A/D converter board; EMGSystem do Brasil Ltda
The skin was shaved and cleaned with alcohol to reduce skin impedance at the electrode positioning sites. EMG signals were collected unilaterally. The symptomatic shoulder was selected in both groups. The UT, MT, and LT electrodes were positioned according to the recommendations of the Surface Electromyography for the Non-Invasive Assessment of Muscles – The SENIAM project [26]. The electrodes placed on the SA muscle followed the advice of Park and Yoo [27], and the recommendations proposed by Escamilla et al. [28] were followed to position the electrodes on the external oblique (EO) and rectus abdominis (RA) muscles.
Experimental procedures
The experimental protocol was divided into two stages. The first consisted of filling out the personal data questionnaire, assessing pain intensity, and measuring body mass and height. Then, scapular dyskinesis was evaluated.
The second step consisted of assessing the maximum voluntary isometric contraction (MVIC) and performing the exercises. Three MVICs for each muscle were performed, holding the contraction for six seconds, with a one-minute interval between each execution, and three minutes between each muscle. The MVIC was performed in a random sequence, according to the recommendations of Kendall et al. [29].
A1: Closed Row starting position; A2: Closed Row End Position; B1: Pronated Row starting position; B2: Pronated Row End Position; C1: Push-up starting position; C2: Final position of the Push-up; D1: Scapular Push-up starting position; D2: Scapular Push-up End Position; E1: T-push-up starting position; E2: T-push-up end position.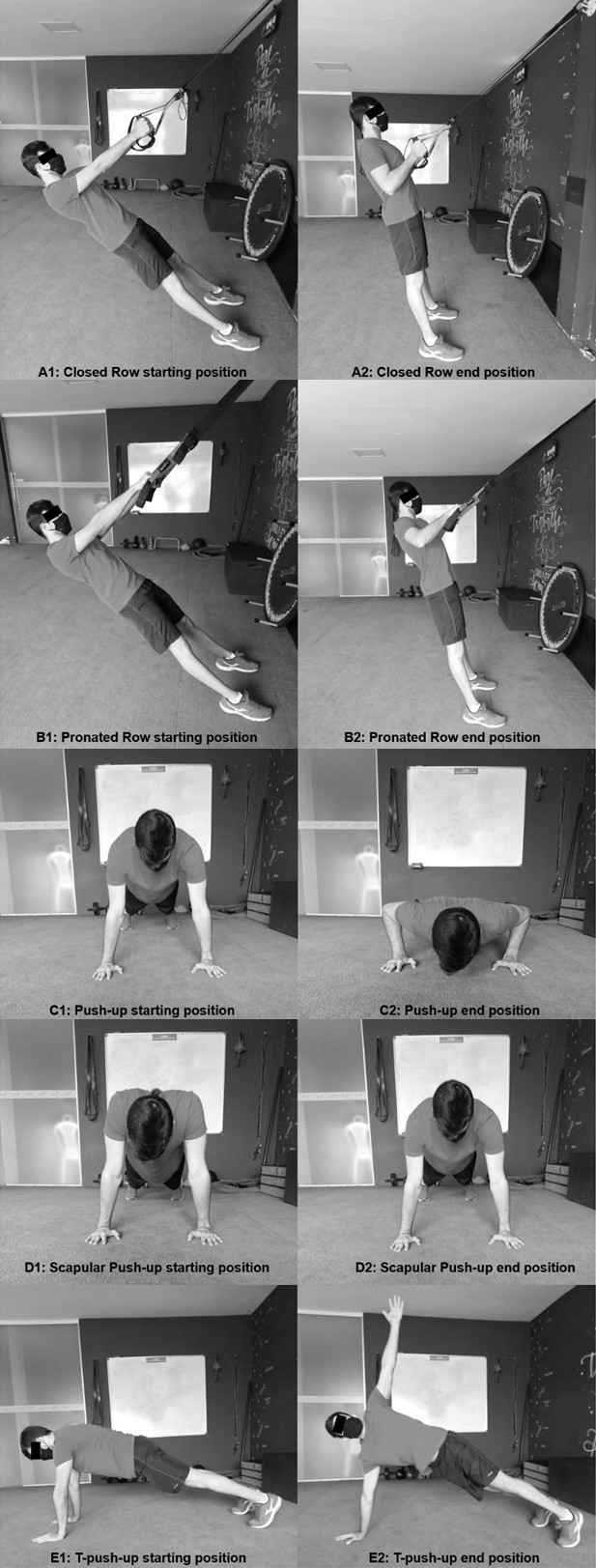
After the MVIC procedures were completed, a 30-minute interval was applied to start the exercises randomly selected:
Closed Row: In the initial position, the volunteer stood up, holding the suspension straps with the feet in the place marked with an adhesive tape that allowed a 40 Pronated Row: In the initial position, the volunteer stood up, holding the suspension straps with the feet in the place marked with an adhesive tape that allowed a 40 Push-up: In the initial position, the volunteer positions the trunk prone with the knees and elbows extended. In the final part, the volunteer brings his body towards the floor, performing the eccentric movement of elbow flexion and horizontal abduction of the shoulders. Scapular Push-up: In the initial position, the volunteer positions the trunk prone and the elbows extended. In the final part, the volunteer performs a protraction of the scapulae. T-Push-up: In the initial position, the volunteer positions the trunk prone with the knees and elbows extended. In the intermediate position, the volunteer brings his body towards the floor, flexing the elbows and horizontal abduction of the shoulders, and ends by performing a trunk rotation, raising the arm high towards the ceiling. EMG activity was recorded on the support arm (Closed Kinetic Chain) during the five repetitions.
The volunteers performed five repetitions lasting two seconds (one second for the concentric phase and 1 second for the eccentric phase) at a metronome-controlled speed. Two-minute rest intervals were adopted between each exercise series. Verbal commands were also used to emphasize the execution speed of the task when necessary.
All data were processed using EMGLab v2.0 software for acquisition and analysis and sampled by a 16 A/D converter board with a 2 kHz frequency. Raw EMG data were digitally filtered at a frequency bandwidth between 16–500 Hz, and the root mean square (RMS) was calculated to represent the amplitude values of the EMG. The EMG data collected during each exercise was normalized by the RMS maximum value obtained in three MVICs collected during manual muscular testing for each muscle.
Statistical analysis
Data were processed and analyzed using the JAMOVI (version 2.3). Generalized Mixed Models were used to analyze the dependent variables in each exercise. We tested several models, considering different types of covariance matrices, types of data distribution, and link functions. The choice of the most appropriate model was guided by the analysis of the normality of the residues and by the lowest values of Akaike’s Information Criterion (AIC) and Bayesian Information Criterion (BIC).
An unstructured covariance matrix was considered. The groups and exercise conditions were considered fixed factors, and the volunteers were considered random factors. The model was fitted with a Gamma distribution and log link function. Bonferroni post hoc was used given the significant reason for the isolated effect of the group and exercise or interaction between them. Descriptive data are presented as estimated marginals mean
Results
Description of the demographic and anthropometric variables of the subjects who participated in the study
Description of the demographic and anthropometric variables of the subjects who participated in the study
Legend: BMI – Body Mass Index; NPRS – Numeric Pain Rating Scale. Data are presented as mean (SD) or absolute (%) values.
Normalized RMS (% MVIC) values of the EMG activity of the muscles were analyzed during the five exercises for both groups (Estimated Marginal Means (standard error))
Legend: SA – Serratus Anterior; UT – Upper Trapezius; MT – Middle Trapezius; LT – Lower Trapezius; EO – External Oblique; RA – Rectus Abdominis.
Table 1 shows the demographic and anthropometric data of the sample. In addition, information regarding the intensity and duration of symptoms of shoulder pain is reported. No statistical difference was observed between groups.
Table 2 illustrates the normalized EMG activity values of the muscles analyzed during the five exercises for both groups. The analyzes regarding the EMG activities of the MT muscles did not reveal group effects (
No group (
There was an effect on the type of exercise (
Similarly, we did not find a group effect (
The study hypothesis considered that symptomatic volunteers with scapular dyskinesis would present decreased EMG activity of the abdominal muscles, MT, LT, and SA, during the performance of the proposed exercises. However, our results only showed a decrease in the EMG activity of the SA and EO during the t-push-up exercise. No differences were observed between groups for the different portions of the trapezius and the RA, which partially confirms our initial hypothesis.
In general, the literature has reported that individuals with scapular dyskinesis present increased activity of the upper trapezius (UT), delayed activation, or decreased activity of the lower trapezius (LT) and serratus anterior (SA) when performing movements with the upper limbs, However, in our study, no differences between groups were observed in the EMG activity of UT, MT, and LT. This finding suggests that dyskinesis was not a moderating factor for the EMG activity of the trapezius muscle. Considering that the population studied had subacromial pain, possibly no differences were observed between the groups because pain is identified as a factor capable of influencing the EMG activity of the MT and LT [30].
Regarding the RA, our results showed low levels of EMG activity, demonstrating small participation of this muscle in the stabilization of the trunk during the exercises performed. A recent systematic review [31] showed that the RA muscle has more significant EMG activity when performing upper limb exercises with free weights (rotational loads) and in unstable conditions. Considering that our exercises did not have significant instability components and the applied loads presented an axial direction, we can infer that the demand for core stabilization was not so high as to require a greater neuromuscular demand for the RA. In this case, the participants did not receive any guidance for maintaining the core. However, previous studies have shown that guiding and monitoring the conscious contraction of the abdominal muscles can increase their EMG activity. As well it can increase the EMG activity of the periscapular muscles [16, 32, 33, 34, 35].
The main finding of our study refers to the between-group differences in the EMG activity of the EO and SA. We observed that volunteers with pain and scapular dyskinesis decreased the EMG activity of the referred muscles. These findings support the theory of myofascial connections that reinforce an anatomic and functional relationship between EO and SA [33] and previous results that point to the influence of abdominal muscles on SA EMG activity [16, 32, 34, 35].
In addition, previous studies have shown a positive correlation between the EMG activity of the EO and SA [17] during the push-up, and subjects with dyskinesis have impaired EMG activity in both muscles [18]. The presence of scapular dyskinesis contributes as a moderating factor in EMG activity, suggesting that there may be an influence on the transmission of forces and energy along the kinetic chain that connects the trunk to the upper limbs. However, this influence seems to occur only in situations with increased mechanical demand for trunk stabilization, and the complexity of the task, since no differences were observed in the exercises performed with both arms. On the other hand, when combining a task with unilateral support and trunk rotation, we observed a negative impact on the activity of both muscles.
This argument of mechanical or neuromuscular complexity seems to make sense and to be reinforced by previous findings that reported no negative impact on EO and SA activity in subjects with dyskinesis during bench press and crucifix exercises in which the trunk is stabilized on the bench [19] or in a push-up exercise performed on stable bases or with unidirectional instability [20]. However, when multidirectional instability devices are used, it is possible to observe a significant decrease in the EMG activity of the SA and EO in subjects with scapular dyskinesis [17, 18].
From a practical point of view, these findings introduce questions to the decision-making process regarding the choice and progression of exercises throughout the rehabilitation program of patients with shoulder pain and associated scapular dyskinesis. It may be necessary to consider conditioning the core muscles before deliberately introducing closed kinetic chain exercises with high mechanical demands or levels of complexity to the shoulder joint complex. In addition, the results suggest that, in the initial stages, it may be interesting to prioritize the closed row exercise to strengthen the MT and LT muscles. As well as the scapular push-up for strengthening the AS. In both exercises it was possible to observe low EMG activity for the UT. These findings corroborate several previous studies that recommend the use of exercise programs that promote greater EMG activity in the SA and LT and less activity in the UT [10, 36, 37, 38, 39].
However, the present study has some limitations. First, the absence of kinematic data does not allow us to assess whether changes in scapular movement accompany EMG changes. Next, our findings refer to volunteers who reported not exercising in the last three months. Thus, these findings cannot be extrapolated to athletes or physically active subjects. In addition, we evaluated tasks performed with body weight, and it was impossible to make any inference about the influence of the intensity or load used in the exercises on the analyzed outcomes. Thus, we suggest that future studies simultaneously analyze kinematic and EMG data, in subjects with different levels of physical activity, during other tasks and control the intensity or load.
Conclusion
We conclude that scapular dyskinesis in subjects with subacromial pain did not influence the EMG activity of the trapezius and rectus abdominis. Therefore, rehabilitation programs may initially prioritize rowing and push-up exercises to strengthen the middle trapezius, lower trapezius, and serratus anterior muscles. On the other hand, the execution of more complex exercises with greater mechanical demand on the kinetic chain, such as the T-push-up, may have to be implemented in later phases.
Author contributions
CONCEPTION: Ana Carolina Pitangui and Rodrigo de Araújo.
PERFORMANCE OF WORK: Laís Santos, Gabriel Batista, Felipe Oliveira, Ana Carolina Pitangui and Rodrigo de Araújo.
INTERPRETATION OR ANALYSIS OF DATA: Ana Carolina Pitangui and Rodrigo de Araújo.
PREPARATION OF THE MANUSCRIPT: Laís Santos, Gabriel Batista, Felipe Oliveira, Ana Carolina Pitangui and Rodrigo de Araújo.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ana Carolina Pitangui and Rodrigo de Araújo.
SUPERVISION: Ana Carolina Pitangui and Rodrigo de Araújo.
Ethical considerations
The study was conducted according to the principles of the Declaration of Helsinki, in compliance with the Brazilian legal and regulatory framework for research involving human beings (NR 466/12) and approved by the Ethics and Research Committee of the University of Pernambuco (CAAE: 89885318.5.0000.5207).
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors thank the participants for their contribution to the study.
Conflict of interest
The authors have no conflicts of interest to report.