
Abstract
BACKGROUND:
The scapular dyskinesis has been described as a sign of scapular instability due to weakness or imbalance of scapular muscles.
OBJECTIVE:
The aim of this study was to compare the EMG activity of the periscapular and abdominal muscles of asymptomatic subjects without and with scapular dyskinesis type II during a push-up exercise performed on different surface stability conditions.
METHODS:
Twenty-seven physically active men were allocated into two groups: the Control group (
RESULTS:
The control group showed an increase in MT activity (mean difference
CONCLUSION:
The insertion of unstable surfaces increased MT activity in the control group only. The insertion of the unstable surface, either the hands or the footrest, did not provide significant effects for the other muscles.
Introduction
The scapula has received much attention from several researchers in recent years who have evaluated normal and altered kinematics and periscapular muscle activity in different contexts [1]. Interventions focused on periscapular muscles have been proposed and tested in patients with shoulder pain [2]. This attention has been justified by the premise that an “unstable” or dyskinetic scapula” is related to shoulder disorders. Several authors claim that the scapula provides a stable basis for upper limb motor function and that the scapular muscles would be responsible for promoting the stability and mobility of the shoulder joint complex [1, 3]. At the same time, the scapulothoracic joint acts as a connection between the trunk and core muscles and the upper limbs, ensuring the necessary synergy for movement and transmission of forces [4].
Altered scapular position and movement, a change called scapular dyskinesis, has been described as a sign of scapular instability due to weakness or imbalance of scapular muscles [5]. However, McQuade et al. [6] presented a theoretical and critical perspective questioning the reasonableness of the concept of instability applied to the scapula. The scapulothoracic joint is not a true joint, and therefore the biomechanical concepts that describe synovial joints cannot be directly replicated. The authors suggest that the tensegrity model could better explain the mechanical role of the scapula and that it would therefore be unreasonable to expect a balance of forces between the scapular muscles. Also, variations in the scapular position and movement are demonstrative of some normal variability, exposing periscapular muscles to variations in the length-tension relationship which modify their movement arms and their mechanical advantages [6].
Clinical evaluation of scapular dyskinesis aims to identify altered scapulothoracic joint movement, but definitions are inconsistent among different diagnosis propositions. In this sense, analyzing whether individuals with scapular dyskinesis by the YES or NO classification [7] or the Scapular Dyskinesis Test [5] have different EMG responses than control individuals seems to be inadequate. Such comparisons may result in some bias since both the YES or No and the Scapular Dyskinesis Test classifications do not consider biomechanical aspects such as in the IV-Types Classification. Moreover, a recent study [8] proposed to shift the paradigm from assessing local and isolated muscle activity in scapular dyskinesis to a broader context, considering the muscle activation of the kinetic chain and the facilitation potential of adding challenges to whole body instability.
Regarding the relationship of shoulder dyskinesis to shoulder disorders and diagnostic inconsistencies, the present study aimed to compare the EMG activity of the periscapular and abdominal muscles of asymptomatic subjects with and without scapular dyskinesis Type II (clinical observation of projection of the medial border of the scapula during shoulder flexion) during a push-up exercise performed on different surface stability conditions. The push-up is a closed kinetic chain exercise that involves transferring forces between body segments, and it is expected that the insertion of instability devices in support of the hands and feet will lead to increased instability of the system as a whole.
In fact, De Araújo et al. [9] observed in asymptomatic subjects that the insertion of the unstable surface in the push-up exercise caused an increase in the EMG activity of periscapular and abdominal muscles. On the other hand, a decrease in EMG activity was observed in subjects with scapular dyskinesis. In both groups, significant correlations were observed between the EMG activity of the serratus anterior and abdominal oblique muscles, demonstrating an anatomical and functional relationship. We hypothesized that the instability would increase the neuromuscular demand on the periscapular muscles in the unafflicted control group while participants with type II scapular dyskinesis would have decreased EMG activity of periscapular and abdominal muscles.
Methods
Participants
An a priori, the sample size was calculated with a statistical F-test with repeated measures analysis of interactions within and between groups, with
The sample consisted of 27 male volunteers, recruited by disclosure and verbal invitation at the University Campus. Eligibility criteria were age of 18–35 years, practicing similar strength training for at least one year without interruption at the university school gym, and no history of injury, surgery, or upper limb pain complaints. Volunteers with scapular dyskinesis types I and III [10] were excluded.
Volunteers who were unable to perform the proposed tasks; started using medications that could interfere with performance; affected by a limited health condition or started another exercise program would be excluded from the study.
The volunteers were allocated into two groups: (control group:
Description of the anthropometric variables of the subjects who participated in the study
Description of the anthropometric variables of the subjects who participated in the study
SD: standard deviation.
The experimental design was a cross-sectional study with a quantitative approach and group comparison. All participants attended the laboratory on a single day. Initially body mass, height, arm length, and body mass index (BMI) calculations were recorded. Then scapular dyskinesis was evaluated, and the participants were allocated to their respective groups.
After skin preparation and electrode placement, the maximal voluntary isometric contraction (MVIC) of the serratus anterior (SA), upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), external oblique (EO) and rectus abdominis (RA) muscles were evaluated. After all the MVICs were completed, the participants were allocated 30 minutes of rest before performing the three variations of the push-up exercises. A randomized draw defined the order of the exercises. Two-minute rest intervals were adopted between each exercise series.
Scapular dyskinesis evaluation
Scapular dyskinesis was evaluated by the dynamic observational method. The volunteer was asked to remain in the orthostatic position and perform eight repetitions of the bilateral arm elevation movement in the scapular plane to the maximum possible amplitude, with dumbbells approximating 3% of body weight [11]. Movement speed was standardized at three seconds for the concentric phase and three seconds for eccentric by the standardized verbal command of the examiners. The execution of the movement was recorded in posterior view by a 60 Hz sampling frequency digital camcorder (SONY model DCR-SX21), positioned on a tripod with a height of 1.00 meters from the ground and at a distance of two meters from the volunteer. Ground markings were used to standardize camcorder and volunteer positioning.
Two orthopedic physiotherapists performed all evaluations independently. The categorization of the type of scapular dyskinesis was performed according to common guidelines [10]. Visualization of the prominence of the inferior angle of the scapula was interpreted as type I; type II represents the increase in medial border prominence; type III is characterized by excessive elevation of the upper angle; and type IV indicates the absence of scapular dyskinesis. Once asymmetry was identified in several planes, the evaluator classified dyskinesis into one of these four types based on the predominant pattern [7]. All volunteers classified as type IV were included in the control group. Volunteers classified as type II were included in the dyskinesis groups, and the others (types I and III) were excluded.
Surface electromyography
Trichotomy and mild abrasion with alcohol were performed to clean the skin at the electrode positioning sites. Simple differential and self-adhesive electrodes (Ag/AgCl – Meditrace 200 Adult, Covidien
The UT, MT, and LT electrodes were positioned according to the recommendations of the Surface Electromyography for the Non-Invasive Assessment of Muscles – The SENIAM project [12]. The electrodes placed on the SA muscle followed the recommendations of Park and Yoo [13], and the recommendations proposed by Escamilla et al. [14] were followed to position the electrodes on the OE and RA muscles. The electrodes were placed on the dominant side of each volunteer (self-reported in relation to the limb used to perform functional tasks).
Normalized RMS (%MVIC) values of the EMG activity of the muscles analyzed during the three push-up plus exercise conditions for both groups (mean
SD)
Normalized RMS (%MVIC) values of the EMG activity of the muscles analyzed during the three push-up plus exercise conditions for both groups (mean
SA: serratus anterior, UT: upper trapezius, MT: middle trapezius, LT: lower trapezius, EO: external oblique, RA: rectus abdominis. PU: push-up, PU-HI: push-up with hand instability, PU-HFI: push-up with hand and feet instability.
Stable Push-up (SPU): (A) starting position and (B) Final position; Push-up with hand instability (PU-HI): (C) starting position and (D) Final position; Push-up with hand and feet instability (PU-HFI): (E) starting position and (F) Final position.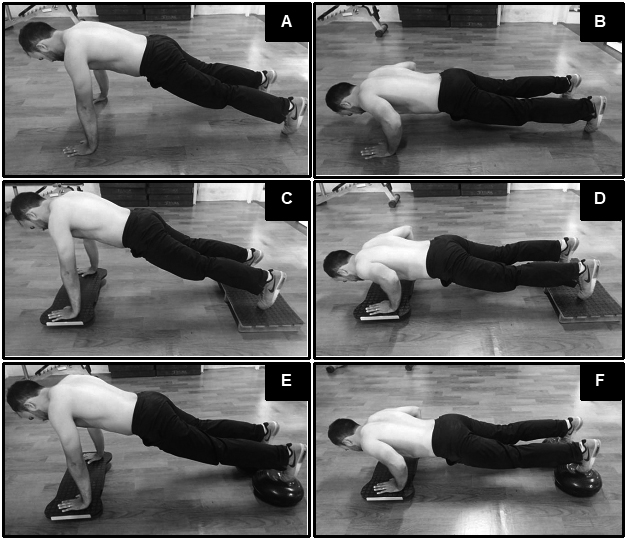
All electrodes were connected to six channels of the EMG800C-1632 Signal Acquisition System (EMGSystem do Brasil Ltda
Two MVICs for each muscle were performed, holding the contraction for six seconds, with a one-minute interval between each execution, and three minutes between each muscle. The MVIC was performed in a random sequence, according to the recommendations of Kendall et al. [15].
After the MVIC procedures were completed, a 30-minute interval was applied to start the specific push-up exercises under three randomly selected conditions: 1) Stable Push-up (SPU): hands and feet on the ground; 2) Push-up with hand instability (PU-HI): Unstable platform applied to upper limbs (subject’s hands resting on a biaxial proprioceptive board); 3) Push-up with hand and feet instability (PU-HFI): Unstable platform was under upper and lower limbs (hands resting on biaxial proprioceptive board and feet resting on Pro Action Fitness
The volunteers performed two sets with six repetitions with metronome-controlled velocity, with a time of two seconds for each repetition cycle (one second for the concentric phase and 1 second for the eccentric phase). Verbal commands were also used to emphasize the execution speed of the task when necessary. Two-minute rest intervals were adopted between each exercise series.
Seventy-five percent of the participant’s height was calculated for the hand and feet length positioning. The positioning of the hands and feet during the exercise was standardized by placing markers with adhesive tapes on the floor. The participants were requested to keep their chest at a height of 10 cm (a 10 cm pile of cups were positioned at the midpoint between the hands) for controlling their movement in the eccentric phase [16].
Mean difference (95% CI) within and between groups of normalized EMG activity (%MVIC) in the different push-up conditions
Mean difference (95% CI) within and between groups of normalized EMG activity (%MVIC) in the different push-up conditions
PU: push-up, PU-HI: push-up with hand instability, PU-HFI: push-up with hand and feet instability. Shaded cells: significant difference.
Data were processed and analyzed using the SPSS (version 20.0; IBM Corp, Armonk, NY). Mixed linear models were used to analyze the dependent variables in each variation of the exercise. An autoregressive covariance matrix was considered. The groups and exercise conditions were considered as fixed factors, and the volunteers were considered random factors. A Q-Q plot was analyzed to attest to the normality of the residuals for all variables. The logarithmic transformation of the data was performed to adjust the model.
Bonferroni posthoc was used given the significant reason for the isolated effect of the group and exercise or interaction between them. Descriptive data are presented as mean
Results
Table 2 illustrates the normalized EMG activity values of the muscles analyzed during the three push-up exercise conditions for both groups.
Table 3 shows the mean differences within and between groups and their respective confidence intervals (95% CI). The control group showed an increase in MT EMG activity under both instability conditions compared to stable push-ups (PU
No significant effect on EMG activity was observed with the implementation of unstable conditions for the other periscapular (UT:
The comparison between groups showed that the control group had higher MT activity compared to the dyskinesis group under unstable conditions (PU-HI:
No differences were observed between the groups for the other periscapular (UT:
Discussion
The present study hypothesized that performing push-ups over an unstable surface would increase EMG activity in the control group but not in the dyskinesis group. In fact, the dyskinesis group showed no significant increase in EMG amplitude of any analyzed muscle when comparing stable and unstable push-ups. On the other hand, the control group only showed increased EMG for the MT activity during push-ups performed on an unstable surface (hands or hands plus feet) when compared to doing push-ups over a stable surface.
This is the first study that standardized some elements in the analysis of subjects with scapular dyskinesis with respect to the EMG activity of periscapular muscles. First, by considering that scapular dyskinesis should not be analyzed as a local problem, we evaluated EMG activity while performing a closed kinetic chain exercise. Also, we inserted instability conditions at the two fulcrum points of the kinetic chain [8]. Second, scapular dyskinesis may present different alteration patterns. Therefore, we decided to evaluate a specific subgroup, considering the movement dysfunction characteristic of scapular dyskinesis (type II) [8]. Finally, we used a device that provides mediolateral instability, as type II dyskinesis may be associated with a change in the control of the medial and lateral rotation movements of the scapula [7, 17].
Data from the present study demonstrate that there was no effect of the unstable surface in the SA EMG normalized amplitude, the main muscle targeted in push-ups, and assessed during EMG registers, irrespective whether the participants belonged to the control or the scapular dyskinetic group. Regarding the dyskinesis group, our findings corroborate previous studies [9, 18] which found no differences between groups in the SA EMG activity during push-ups on a stable surface. However, De Araujo et al. [9] and Pirauá et al. [19] verified that an unstable surface decreases the SA EMG activity of the dyskinesis group. These authors argue that the unstable surface may exacerbate differences in neuromuscular control to perform the task, and speculated that the presence of scapular dyskinesis would be associated with a specific impairment of the SA EMG activity. Another factor is that these authors included all types of scapular dyskinesis, whereas the present study only included type 2 dyskinesis. Thus, we can speculate that different scapular positions may generate varied control strategies. Also, De Araújo et al. [9] found that decreased SA activity was associated with decreased EO activity. According to the authors, a less effective EO would not provide a strong foundation for force transmission and support for SA action. We did not find significant changes in abdominal muscle activity in the present study, which may help to explain the divergent results. There were probably no significant challenges that altered trunk control and consequently did not affect the SA EMG activity.
The influence of unstable surfaces on the EMG activity of periscapular muscles during push-ups is conflicting. The devices used to generate instability, the way the task is performed, and the type of contraction analyzed are factors that can help explain this divergence in the literature. Studies using multidirectional instability devices such as BOSU or proprioceptive discs found increased EMG activity of SA [9, 13, 16, 18, 20, 21]. However, high levels of instability may impair muscle recruitment and consequently decrease EMG activity [22, 23, 24]. Our findings corroborate studies that evaluated the use of an unstable surface during isometric tasks [25, 26, 27, 28] and a study that evaluated dynamic execution with hands resting on a mini-trampoline [29]. The device used in the present study caused mediolateral instability exclusively which may not have provided a sufficient challenge to the neuromuscular system to require an increase in the SA EMG activity.
Instability with the hands and hands plus feet caused differences between groups in the MT EMG activity. There was an increase in MT EMG activity ranging from 3–9% in the control group for push-ups performed over an unstable support surface, whereas no modification was observed in the dyskinesis group. In two studies [23, 30] that reported no changes in EMG activity during push-ups performed over an unstable surface, the unstable surface was only inserted under the participant’s hands, and there was no correction of the feet height from the ground. The biomechanical reasoning for such a finding is the shift in the center of mass caudally to lower limbs due to the trunk inclination caused by the support put under the hands, decreasing the load over the upper limbs and consequently requiring less recruitment of the scapular muscles. Studies that maintained the same trunk height in both stable and unstable push-up conditions [20, 21] showed an increase in the MT EMG activity of healthy subjects. These authors suggest that the increase in MT activity would be related to the need for dynamic control of the scapula during medial and lateral rotation. Reinforcing this hypothesis, Torres et al. [20] found greater coactivation between SA and MT during push-ups performed over an unstable surface.
No changes in MT EMG activity were observed in the dyskinesis group, as aforementioned. The characteristic of the movement dysfunction in this subgroup combined with the unstable surface may have provided a mechanical disadvantage to the MT lever. We speculate the introduction of mediolateral instability may have reinforced any alteration in the MT synergy, typical of the type II scapular dyskinesis during medial and lateral scapular rotation. However, the role of MT in closed kinetic chain tasks performed over a stable and/or unstable support surface has been sparsely explored in the literature, limiting our conclusions. This is mainly because the amount of the observed differences in EMG activity found in the control group MT when comparing stable and unstable push-ups was small, and its clinical significance is still controversial. Furthermore, how the closed kinetic chain can influence the activation of the periscapular muscles, and whether it could be used as a motor impairment indicator related to different subgroups of scapular dyskinesis needs more investigation.
Finally, our data showed no differences in the EMG activity of the UT and LT, corroborating most studies published in the literature [25, 26, 27, 29, 30]. With respect to subjects without scapular dyskinesis, three studies found increased EMG activity of these muscles when performing push-ups over an unstable surface [23, 24, 31]. However, when analyzing the mean differences reported by these authors, they were below 10% of the EMG amplitude obtained in maximal voluntary contractions. According to Finsterer [32], values below 10% of the MVIC only represent spontaneous or resting muscle EMG activities. In this sense, in spite of the reported statistical differences, we believe that they have no practical significance.
The current study has several limitations that should be considered when interpreting the results. Although our sample consisted of individuals who differed in the presence or absence of scapular dyskinesis, all were asymptomatic, which limits the extrapolation of results to asymptomatic individuals. To our knowledge, this is probably the first electromyographic study that examines the influence of the support base on push-up exercises that considered a characteristic movement impairment of a more homogeneous sample of individuals with scapular dyskinesis (Kibler Type II). Therefore, future studies should explore different populations, as well as test other types of exercises and different instability strategies.
Conclusion
The only effect of insertion of unstable surfaces was to increase MT EMG activity in the control group. The insertion of unstable surface, either to the hands or to the footrest, does not seem to result in any significant effect for the other periscapular or abdominal muscles.
Author contributions
CONCEPTION: Rodrigo Cappato de Araújo.
PERFORMANCE OF WORK: Wevans Monthier de Farias and Diego Santiago de Freire Sousa.
INTERPRETATION OR ANALYSIS OF DATA: Wevans Monthier de Faria, Diego Santiago de Freire Sousa and Rodrigo Cappato de Araújo.
PREPARATION OF THE MANUSCRIPT: Wevans Monthier de Farias and Ana Carolina Rodarti Pitangui.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Anamaria Siriani de Oliveira, David Behm and Rodrigo Cappato de Araújo.
SUPERVISION: Ana Carolina Rodarti Pitangui and Rodrigo Cappato de Araújo.
Ethical considerations
The Research Ethics Committee of University of Pernambuco under the registration C.A.A.E approved the study: 629833316.1.0000.520, and all participants signed the informed consent form.
Funding
The authors report no funding.
Footnotes
Acknowledgments
We thank the participants for their contribution to the study.
Conflict of interest
The authors declare no conflicts of interest.