
Abstract
BACKGROUND:
Measurements of hip abduction (ABD) and adduction (ADD) are important in strength and conditioning as well as in clinical practice. However, there is no clear consensus on how ABD and ADD compare in strength in different populations.
OBJECTIVE:
The aim was to perform a quantitative synthesis of comparisons between the isometric strength of ABD and ADD in different populations.
METHODS:
ABD and ADD strength data were collected and pooled mean values for ABD:ADD strength ratio were calculated and expressed as standardized mean differences. Forty studies of healthy adults, 5 studies of healthy older adults and 14 studies of adults with various musculoskeletal injuries were included in the analysis.
RESULTS:
Healthy (non-athletic) males, healthy older adults, and adults with hip and groin pathologies or osteoarthritis tend to have the same ADD and ABD strength; male athletes tend to have a stronger ADD compared with ABD; healthy females and adults with patellofemoral pain tend to have a stronger ABD compared with ADD.
CONCLUSIONS:
These results can serve as a database to help compare and interpret measurements of ADD and ABD strength ratio in different populations.
Introduction
Measurements of motor abilities, such as muscular strength, are of paramount importance in strength and conditioning [1] as well in clinical practice [2]. While the knee joint is perhaps the most commonly assessed [3, 4, 5], the strength and power of the hip joint play an important role in a plethora of movements, including (but not limited to) vertical jumping [6, 7], running and walking [8, 9, 10], changes of direction [11] and balance tasks [12]. Furthermore, several studies have shown the importance of muscular strength in athletic performance [13] and association between inadequate hip and lower limb muscle strength and increased injury risk in different sports (soccer, ice hockey, rugby etc.) [14, 15]. Additionally, evaluation of hip and lower limb muscle strength is also relevant for prevention and treatment of frailty in older individuals [16]. For application of hip strength measurements in clinical practice, there is a need for a comprehensive database that clinicians and coaches can use for decision-making.
Raw normative values in the literature, apart from recent attempts pertaining to knee joint [5], are very scarce [17, 18]. In addition, using different measurement methods (isokinetic dynamometry – considered the gold standard, hand-held dynamometry, externally fixed portable dynamometry, manual muscle testing); different units of measurement (force or torque) and (non)normalization of the measurements to body mass represent a source of heterogeneity that makes it difficult to establish a consistent normative. Clinicians may thus turn their attention to inter-muscular strength ratios. Regarding the bilateral (i.e., inter-limb) asymmetries, more than 10–15 % difference is typically considered as clinically relevant [19, 20]. Additionally, agonist to antagonist ratios are specific to joint and movement tasks. In this case as well, the research has focused almost exclusively on the knee joint, wherein the hamstring-to-quadriceps ratio has been considered as injury predictor [21, 22]. However, less is known about optimal agonist to antagonist ratios for other joints, including the hip. In particular, the ratio between hip abduction (ABD) and adduction (ADD) could be of interest in research and practice in different populations. For instance, ABD strength has been suggested as a factor in running-related injury risk [23], the medio-lateral stability of unilateral balance tasks [24, 25] and landings [26]. ADD strength has been extensively researched in association with groin pain [27, 28, 29].
While hip ABD and ADD strength is clearly important for athletic performance and carrying out the activities of daily living, there is no clear consensus on how ABD and ADD compare in strength in different populations. Therefore, the purpose of this paper is to collect the available isometric strength data (measured either with isokinetic, hand-held, or externally fixed dynamometry) from the existing literature and perform a quantitative synthesis of comparisons between isometric hip ABD and ADD strength in different populations.
Methods
Search strategy
Two different search strings were used in PubMed database using the following key word combination in May 2021: (i) hip muscle strength; (ii) (hip muscle) AND (hand held dynamometer). A language filter (English) and a species filter (humans)) were applied. Additionally, reference lists of systematic reviews, identified during the search process, were also reviewed.
Inclusion criteria
The a priori determined inclusion criteria are outlined below in the form of PICOS search tool [30]:
Population (P): We included studies that involved participants of both sexes, independent of age. Participants from the general population, as well as professional and recreational athletes were considered. If a study investigated patient populations, we considered the data from the healthy control group when available.
Intervention (I): No interventions were considered in this study. In case of interventional studies, only baseline control group values were considered.
Comparisons (C): Not applicable.
Outcomes (O): Isometric hip strength, measured as force (N or N/kg) or torque (Nm or N/kg) during maximal voluntary contraction. Because only ratios were analyzed in this paper, we did not attempt to convert that data to a single unit. If multiple methods of measuring isometric strength were used in a study, we considered the results obtained by the method that we judged to be more valid (e.g. rigid isometric dynamometers with external fixation or isokinetic dynamometers were chosen over hand-held dynamometry).
Study design (S): All study designs were accepted.
Following the inclusion criteria, the extracted data included: (a) means and standard deviations for hip ABD and ADD strength; (b) participant demographics (gender, age, body height, body mass, body mass index, health status, athletic status); (c) measurement details (number of repetitions, duration of breaks, duration of sustained contraction). The data was extracted by the lead author (J.M.), with consultation of the other authors when needed. The data were collated in Microsoft Excel 2016 (Microsoft, Redmond, WA, USA). In a case of missing data, the corresponding author of the target article was contacted by e-mail and through ResearchGate website. If we received no reply to the second inquiry (14 days after the first inquiry), the data was considered unobtainable.
Data grouping, elimination, and analysis
A large majority of studies assessed the hip ABD and ADD strength in or very close to the neutral/anatomical position (i.e. 0–10
Results
Forrest plot showing the analysis for healthy older adults.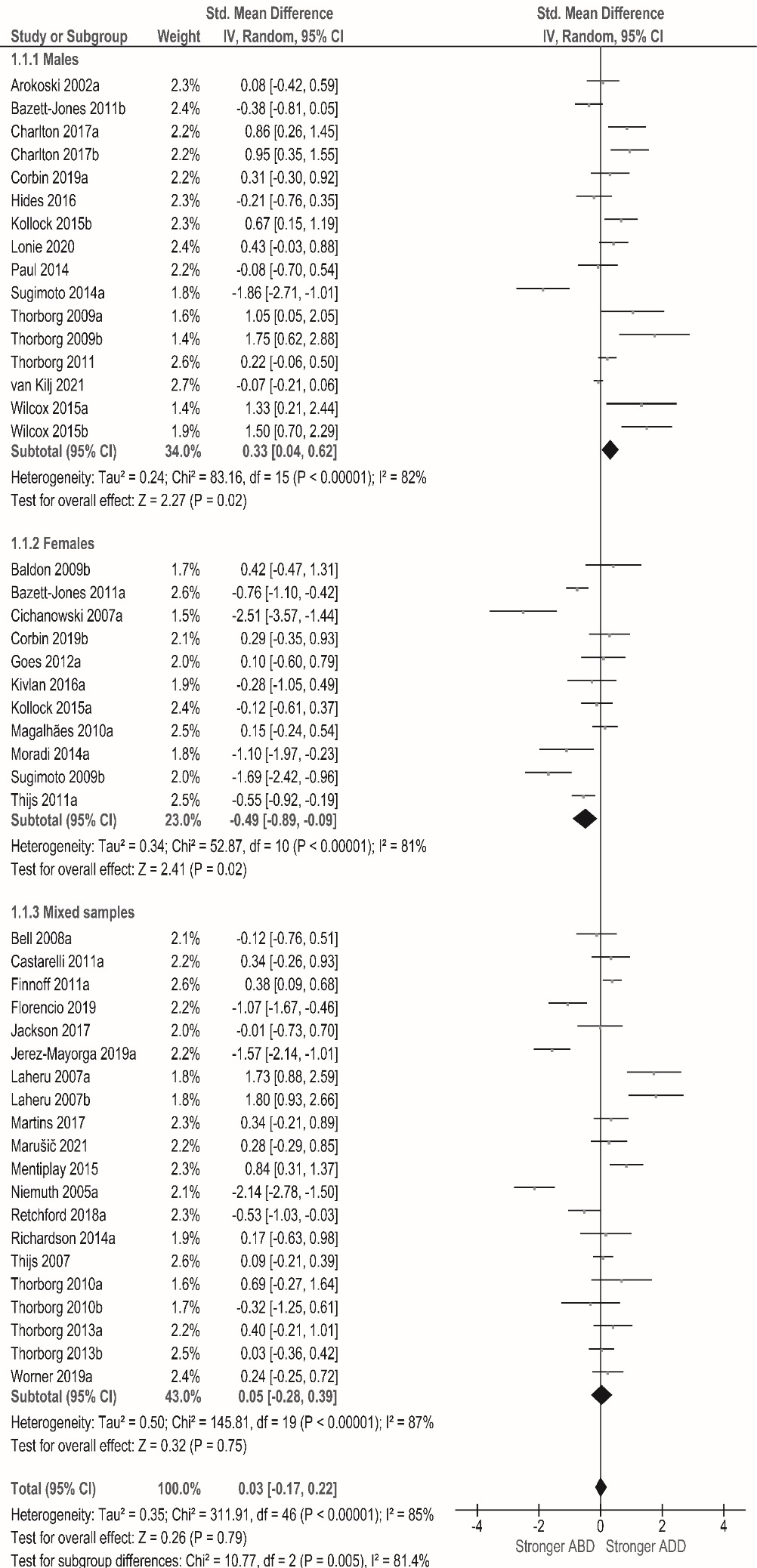
Forrest plot showing the analysis for healthy adults.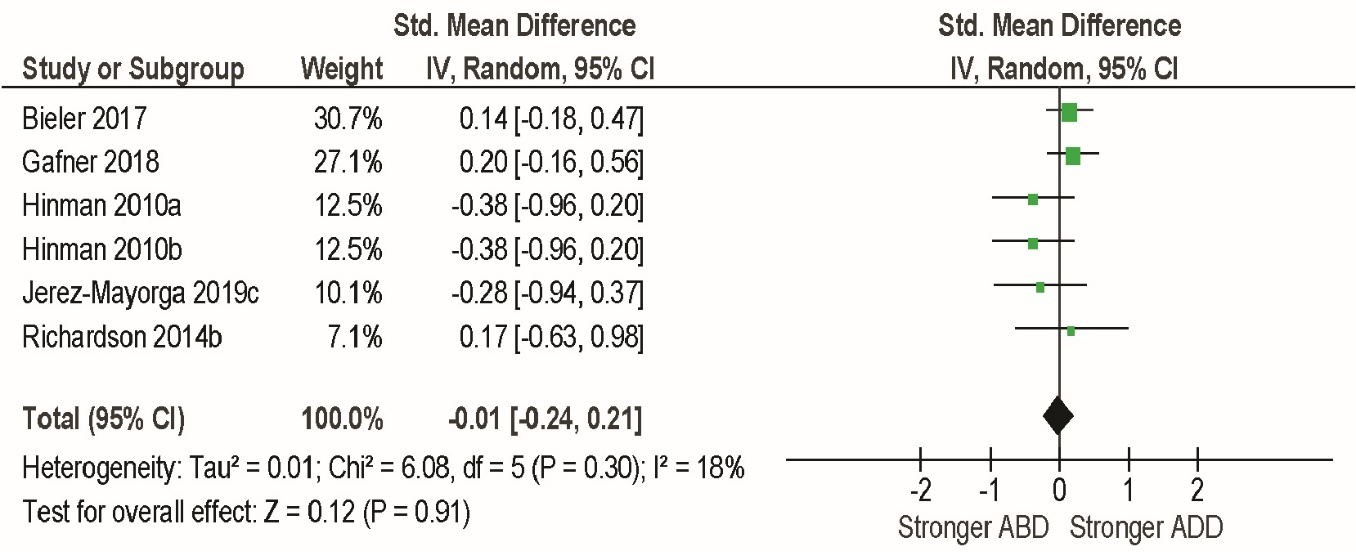
Forrest plot showing the analysis for adults with injuries/pathologies.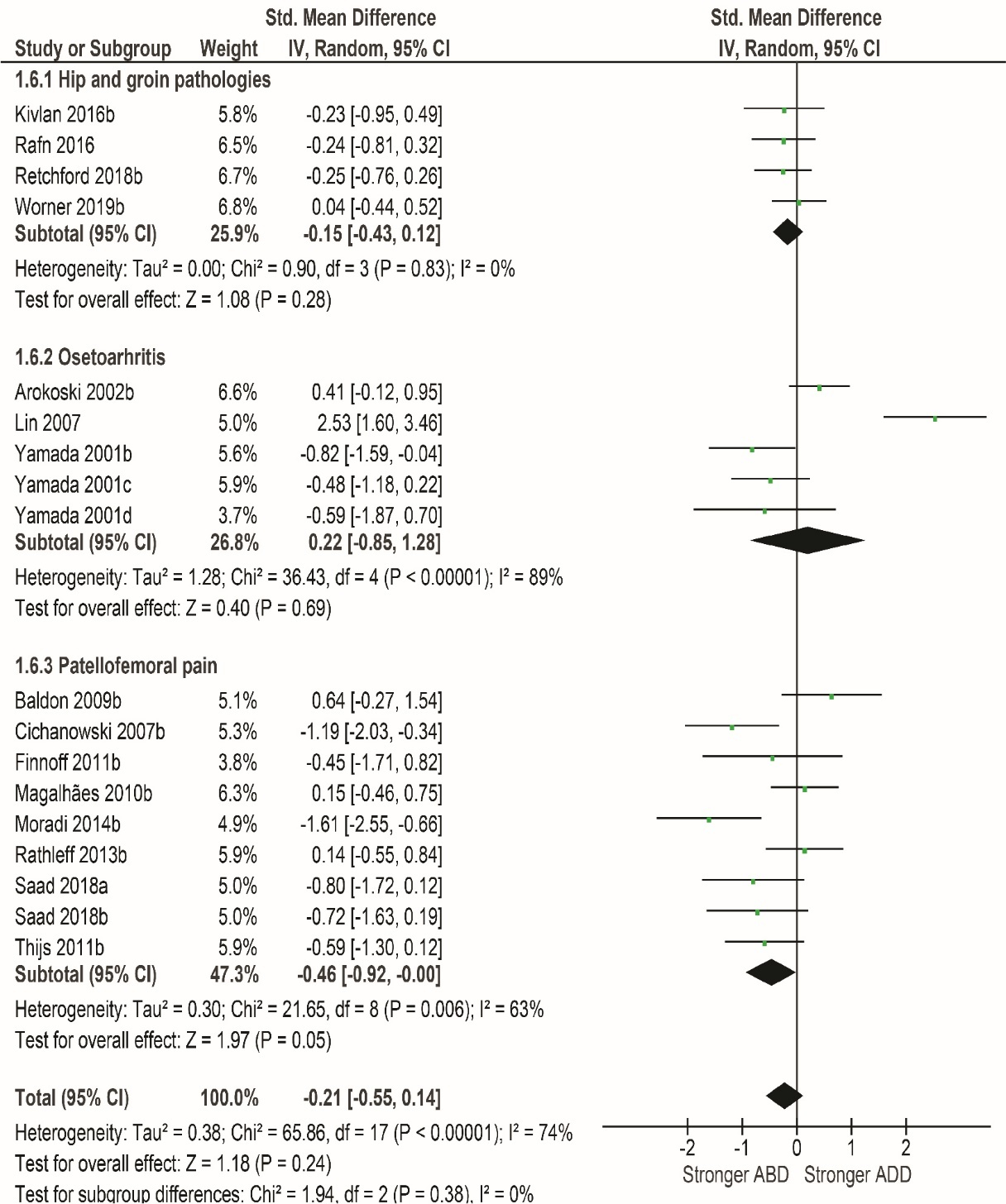
Through a literature review we found that hip ABD and ADD strength was mostly measured either in the supine (in 50% of studies) or in the side-lying position. Additionally, in the vast majority of studies, hip ABD or ADD strength was measured in neutral hip position in all anatomical planes with only minor differences in the frontal plane (0–10
We included 41 studies (47 groups) conducted on healthy adult populations (1756 subjects). The overarching analyses included 16 male groups (from 13 studies), 11 female groups (11 studies) and 20 groups with mixed gender (17 studies). The overall pooled difference between hip ADD and hip ABD was very close to zero (SMD
We performed further subgroup analyses based on the testing position (side-lying vs. supine). Within male groups, ADD was still stronger than ABD in side-lying position (SMD
If athletes were omitted from the main analysis, the pooled difference between ABD and ADD in male groups was reduced to essentially zero (SMD
An additional analysis was performed wherein we compared the subgroups of athletes and non-athletes. In total, 33 groups (29 studies) included non-athletes. For these studies, the pooled effect was not statistically significant (SMD
As with the main analysis above, we performed further subgroup analyses for athletes based on the testing position (side-lying vs. supine). The ADD was stronger in both positions, but the difference compared to ABD was statistically significant only in side-lying position (SMD
Strength ratios in healthy older adults
We included 5 studies (6 groups) that involved healthy older adults (208 subjects) (Fig. 2). The pooled difference between ADD and ABD was close to zero (SMD
Strength ratios in adults with injuries/pathologies
We also included 14 studies (18 groups) that contained adults with various musculoskeletal injuries (294 subjects), which were further classified into 3 subgroups: hip and groin pathologies (4 groups from 4 studies), osteoarthritis (5 groups from 3 studies) and patellofemoral pain (9 groups from 8 studies) (Fig. 3). In hip and groin pathologies, there was a slight (SMD
Discussion
The purpose of this paper was to collect the available data and perform a quantitative synthesis of isometric hip ABD and ADD strength ratios in different populations. To the best of our knowledge, this is the first attempt at pooling hip ABD and ADD strength data and obtaining ABD and ADD strength ratios by performing comprehensive review of the literature. Only one similar study [36] was conducted on hip muscle strength, which aimed to (i) systematically review studies assessing isokinetic hip muscle strength and determine their quality of evidence and (ii) summarize and pooled data of normative values for hip muscle strength. However, the authors concluded that the absolute reference values for hip muscle strength in isokinetic tests are mostly unclear and that pooling isokinetic data from the reviewed studies was not possible. Similarly, it has proven difficult to pool absolute (raw) hip ADD and ABD isometric strength values, mainly due to inconsistencies in the use of strength output units in different studies (authors mostly used either normalized or non-normalized force and torque [N, Nm, N/kg, Nm/kg]; to a lesser extent, results were also reported in % bodyweight).
We collected the data for the following groups: healthy adults (further sub-grouped by gender and athletic status) (40 studies, 47 groups), healthy older adults (5 studies, 6 groups) and adults with injuries/ pathologies (14 studies, 18 groups). Overarching analysis on healthy adult populations and healthy older adults showed no difference between the isometric hip strength of ABD and ADD. However, when subgroups were analyzed, there were significant differences between the sexes (male groups tended to have stronger hip ADD, whereas the opposite was true for females; consequently, the mixed-sample groups had the same ABD and ADD strength). Further analysis showed that only male athletes tended to have significantly stronger ADD muscles, while non-athletic males generally had the same ADD and ABD hip muscle strength. In addition, the testing position has also been shown to affect the comparison of hip ADD and ABD strength, both in healthy athletic and non-athletic populations. The difference is generally greater (in favor of ADD) in the side-lying position compared to supine position due to the effect of gravity. This indicates that the results from side-lying position need to be gravity corrected to make them more relevant and comparable to measurements in other testing positions. In clinical practice, the supine position is therefore probably preferable, as the examiner does not need an additional measurement to gravity correct the result afterwards. However, only a few studies in our review mentioned that the results were actually gravity corrected. To sum up, results of our study suggest that the gender, athletic status and testing position of the subjects should be considered when interpreting the results of hip ABD and ADD strength measurements.
There may be several reasons why athletes tend to have stronger ADD than ABD. First, different sport movement demands could alter the hip ADD:ABD strength ratio in athletes. For example, in soccer, a large number of kicks are performed with the inside part of the foot, which cause high muscle force and stress of the hip adductors [37]. A large accumulation of muscle-specific load throughout the season(s) could preferentially increase hip ADD strength and consequently increase the hip ADD:ABD ratio. Secondly, athletes are advised to specifically strengthen the hip adductors as part of injury prevention training [38], as weakness of these muscles has been shown to be one of the key contributing factors for (adductor-related) groin injuries [39]. Groin injuries are a major problem in sports, especially ice hockey and soccer [40, 41, 42]. Specifically, a 15-year long prospective study involving 47 elite European soccer teams and 3055 players showed that groin pain accounts for 14% of all injuries and affects
An important new finding of this study is that females generally tend to have stronger ABD compared to ADD in isometric conditions. One possible reason for such strength ratio in the female sports population may be a greater emphasis on hip ABD strengthening to reduce valgus stress and thus the risk of anterior cruciate ligament injuries (the incidence in females can be
It is not clear whether the aforementioned differences in hip ABD and ADD strength ratio between studies with similar populations (in terms of gender, age, athletic status, etc.) are due to different types of muscle contractions (concentric vs. eccentric vs. isometric), different measurement positions (standing vs. side-lying), different measurement devices, or something else. In clinical practice and research, hip strength is measured using different methods (manual muscle testing, hand-held dynamometry, isokinetic dynamometry), use of novel devices [34, 35], in a variety of body positions (supine, prone, side-lying, standing, seating), unilateral or bilateral. Even in the same body position, the positions of the measured and unmeasured joints may differ significantly (e.g., isometric strength of hip ADD may be measured supine with hip and knee in neutral/anatomical position, hip in 10–30
A limited number of studies have investigated hip ABD and ADD strength in patients with musculoskeletal injuries. While we found no indication that either ABD or ADD is stronger in patients with groin/adductor injury, groups with patellofemoral pain tended to have moderately larger hip ABD than ADD strength values. Although hip abductors are paramount for the control of the hip in the frontal plane as well as knee valgus [53, 54], which could be related to knee injury risk [55], epidemiological data seem to agree with our results. Specifically, isometric hip ABD was moderately associated with patellofemoral pain incidence in adolescents, but not in adults [56]. It was suggested that increased ABD strength could be an adaptation to the increased physical demands, that also contribute to injury [57]. Further prospective studies are needed to elucidate if hip ABD and ADD strength, and the ratio between the two, are significant risk factors for musculoskeletal injuries.
Some limitations of this review must be acknowledged and discussed. First, although the authors conducted the review with the utmost care and scrutiny, the relevant body of literature is extensive, and it possible that some studies were omitted. In addition, only one database was searched. Nevertheless, we believe that a substantial proportion of the relevant studies were included in the review, and that the addition of further individual studies would have little or no impact on the pooled results. Another limitation of this study is that the sample included only adult and elderly populations. Therefore, the results cannot be used to infer the relationship between hip ABD and ADD strength in younger populations.
Author contributions
CONCEPTION: Nejc Šarabon.
PERFORMANCE OF WORK: Jan Marušič, Žiga Kozinc, Nejc Šarabon, Vedran Hadžič.
INTERPRETATION/ANALYSIS OF DATA: JanMarušič, Žiga Kozinc.
PREPARATION OF MANUSCRIPT: Jan Marušič, Žiga Kozinc.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Nejc Šarabon, Vedran Hadžič.
SUPERVISION: Nejc Šarabon.
Ethical considerations
Not applicable.
Funding
This research was financially supported by the University of Primorska through internal research programme KINSPO (Kinesiology for movement performance and musculoskeletal injury prevention in sport; grant number: 2990–1-2/2021).
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors report there are no competing interests to declare.