
Abstract
BACKGROUND:
Most previous studies have focused on increasing hamstring flexibility when knee extension range of motion (KE ROM) is restricted. However, it was demonstrated that the tensile force generated in the upper body could be transmitted to the contralateral lower extremity.
OBJECTIVE:
This study examined the effect of novel diagonal stretching combining trunk rotation and trunk flexion on the contralateral KE ROM.
METHODS:
Two different positions (sitting with a neutral pelvis position and sitting with trunk rotation) were randomly selected and the contralateral and ipsilateral KE ROM was measured in each position. As for the stretching intervention, trunk rotation and slight trunk flexion were applied in sitting with a neutral pelvic position.
RESULTS:
On the contralateral side, KE ROM was significantly different in all pairwise comparisons (
CONCLUSIONS:
The tensile force in the upper body significantly affects tissue extensibility in the lower extremity in the contralateral side, leading to the restriction of active maximum knee extension. Diagonal stretching techniques may successfully enhance mobility in the contralateral leg.
Introduction
During gait, knee extension range of motion (KE ROM) is important for both optimal kinetics and kinematics [1]. Limited knee extension can cause step length to become shorter during the swing phase because the shank is unable to advance fully [2]. Additionally, during mid-stance, a flexed knee joint will interfere with full extension of the hip joint [2]. Slightly flexed hip and knee joints will reduce stability and require additional compensatory muscle activity, leading to a reduction in gait economy [3]. Restricted KE ROM has frequently been observed in the faulty posture or soft tissue tightness that occurs after injury [4]. Particularly, hamstring tightness can induce a reduced ROM of the pelvis during forward bending by causing a posterior tilt [5, 6], and also restrict full knee extension, limiting the mobility of the pelvis and trunk. When sustained over a long period of time, these changes can induce low-back pain [7]. In this case, higher EMG activity of the hamstrings is observed in comparison to controls [6], which can cause unnecessary additional loading of paraspinal tissues and the vertebral column [6, 8]. Pelvic rhythm and sagittal mobility of the spine during trunk flexion are also affected [9, 10, 11]. In clinical practice, various intervention methods have been applied to improve the restricted KE ROM.
To date, most previous studies have focused on increasing hamstring flexibility through stretching [12]. The hamstrings originate from the ischial tuberosity and insert onto the medial and lateral side of the tibial head and fibular head. As bi-articular muscles, the hamstrings can have direct effects on hip and knee ROM. In previous studies, a significant increase in active and passive knee extension ROM was observed after both static and active stretching [13, 14, 15]. In addition, KE ROM is also affected by thoracic and cervical flexion [7], because the passive connective and/or neural tissues that travel a longer distance as well as muscle tissues that directly control by attaching to the pelvis and femur (or tibia) affect [16]. While there have been several studies on the effects of promoting passive connective tissue extensibility on KE ROM, most studies were focused on motion in the sagittal plane.
However, the posterior upper body and lower limb are obliquely cross-linked by the thoracolumbar fascia (TLF). An experiment with cadavers revealed that even low levels of tensile force caused by traction were transmitted across several segments through the TLF [17]. In addition, it was proven that the latissimus dorsi was connected to the contralateral gluteus maximus and hamstrings by the posterior oblique sling (POS) system [18, 19, 20, 21]. This leads to an assumption that tensile force generated in the upper body could be transmitted to the contralateral lower extremity. However, there have been few studies on rotation in the transverse plane. A recent case study reported a significant improvement in hamstring flexibility after stretching together with trunk rotation [22]. However, the study was limited in that rotation in the transverse plane was used as a part of a comprehensive intervention; it was therefore impossible to examine the pure effect of trunk rotation.
The purpose of this study was to investigate 1) the effects of passive tension in the upper portion of the POS induced by trunk rotation on the mobility of the contralateral extremity, and 2) to examine the effect of novel diagonal stretching combining trunk rotation and trunk flexion on the contralateral KE ROM.
Methods
Subjects
G*Power version 3.1.9.7 (Heinrich-Heine-Univer-sität Düsseldorf, Düsseldorf, Germany) was used for sample size estimation. Based on an effect size of 0.40, the estimated
Procedures
Subjects were instructed to sit with the neutral pelvis position. Two positions for measurement (sitting with a neutral pelvis position and sitting with right trunk rotation) were randomly selected before the stretching intervention by using the RAND function of Microsoft Excel 2019 (Microsoft, Redmond, WA, USA). In each position, KE ROM and visual analogue scale (VAS) in the right leg (contralateral side) and left leg (ipsilateral side) were randomly measured. If the contralateral lower extremity was first measured in the initial position, the ipsilateral lower extremity was first measured in the opposite position. Ten minutes of rest was provided between position changes.
In sitting with a neutral pelvic position, there was a slight gap between the back of the knee and the edge of the treatment table, and a back support was in place to help maintain an ideal position. During active maximum knee extension (KE), KE ROM was measured by using a Bluetooth embed IMU sensor (Re-live Inc., Kimhae, Korea), and pain was simultaneously measured with VAS.
In sitting with trunk rotation, a therapist with 15 years of experience in musculoskeletal physical therapy practice rotated the upper trunk with the right hand of the subject being placed on the left shoulder. During trunk rotation, a neutral pelvic position was maintained, preventing pelvis-induced change in the length of the hip extensors. In addition, the hamstrings were relaxed by sitting with 90
As for the stretching intervention, trunk rotation and slight trunk flexion were applied in sitting with a neutral pelvic position in consideration of the morphological properties of the POS. The therapist rotated the upper trunk with the right hand of the subject placed on the left shoulder and generated slight trunk flexion at the same time. The therapist performed a total 3 trials of static stretching (10-s/trial, 5-s rest between trials) with external force in a diagonal direction. After passive diagonal stretching, KE ROM and VAS were measured in sitting with a neutral pelvis position.
Data analysis
The Shapiro-Wilk test was used for testing data normality. The Friedman test was used to compare KE ROM and VAS in the left and right leg, separately, followed by Wilcoxon signed-rank tests with Bonferroni correction. The significance level was set at
Sitting with the pelvis in a neutral position (a) and with trunk rotation and trunk flexion.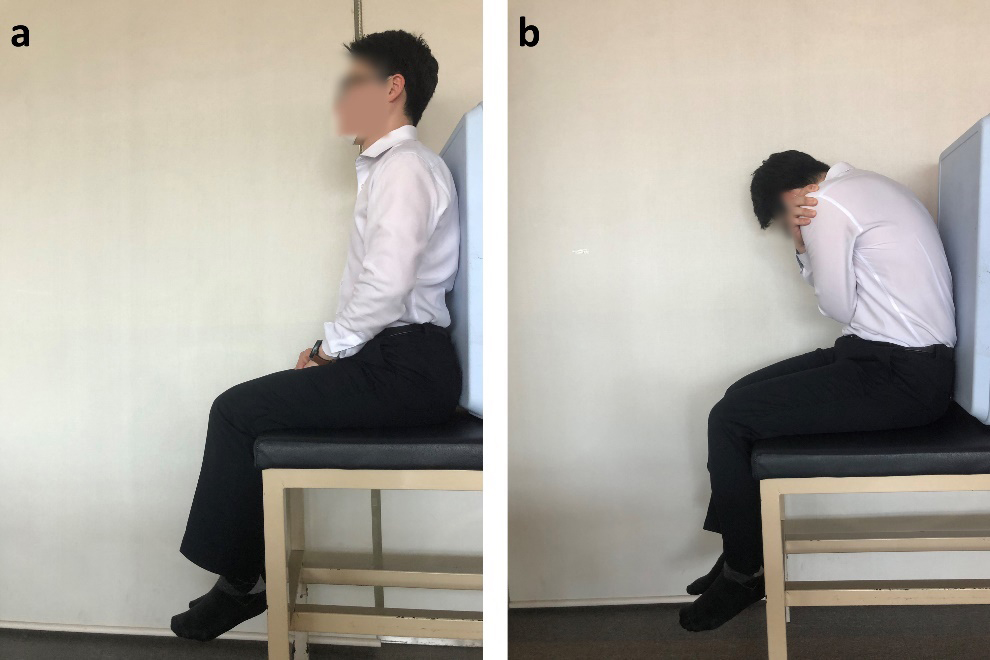
On the contralateral side, KE ROM during sitting with a neutral pelvis position, sitting with right trunk rotation, and sitting with a neutral pelvis position after stretching were 158.4
Changes in Knee extension ROM in contralateral lower extremity. ROM, range of motion; VAS, visual analogue scale; Bar charts show Knee Extension ROM and dots with broken lines show VAS; * statistically significant difference in Knee Extension ROM; §statistically significant difference in VAS.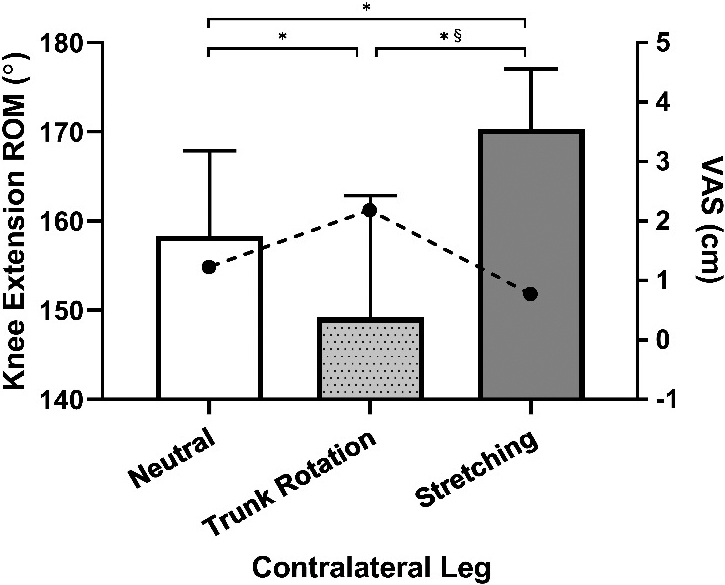
On the ipsilateral side, KE ROM during sitting with a neutral pelvis position, sitting with right trunk rotation, and sitting with a neutral pelvis position after stretching were 162.9
Changes in Knee extension ROM in ipsilateral lower extremity. ROM, range of motion; VAS, visual analogue scale; Bar charts show Knee Extension ROM and dots with broken lines show VAS; * statistically significant difference in Knee Extension ROM; §statistically significant difference in VAS.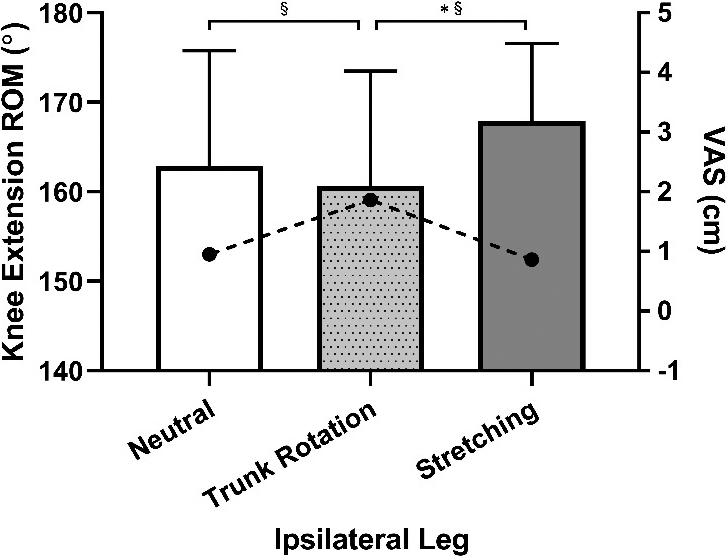
In the contralateral leg, KE ROM significantly decreased during trunk rotation in comparison to a neutral position, and significantly increased after stretching. In contrast to KE ROM, pain was at the highest during trunk rotation and significantly decreased after stretching. These results indicate that the upper portion of the POS is linked to the contralateral lower extremity. Previous studies have shown that muscle activities of the upper body are synchronized with muscle activities of the contralateral lower extremity [20]. In a healthy adult, EMG activity of the gluteus maximus changed based on different shoulder positions of the contralateral side [23]. Similarly, this relationship was also observed during gait showing an increase in muscle activities of both upper body and lower body, obliquely matched, with increasing gait speeds [24]. Previous studies have demonstrated linkage of muscle activity, whereas the present study showed the linkage of passive connective tissues. During trunk rotation to the right, contractile protein and non-contractile protein in the latissimus dorsi of the left-back; the perimysium, endomysium, and epimysium that surround the muscles; and fascia that covers the surrounding tissues increased in tension together. The tensile force generated here was transmitted to the contralateral lower extremity via the TLF [19, 25]. One vital aspect is interpretation between the restriction of KE ROM by the passive tension generated by trunk rotation and the increase in KE ROM by temporally elongated soft tissues after stretching must be differentiated. The extensibility increases after stretching suggest not only connection of the POS to the lower extremity, but also an additional increase in KE ROM by extension of the length of the upper portion of the POS. This implies that full KE would require not only the extensibility in the lower extremity but also the extensibility in the upper body to some extent.
Previous studies have reported that less extensible skin at scar tissues affected distal joint ROM, and the extensibility of tissues both proximal and distal to the joint is required for full joint ROM [26, 27, 28]. In this study, the pelvis was fixated in a neutral position during trunk rotation. Additionally, the knee joint was flexed by 90
Normalized knee extension in contralateral and ipsilateral lower extremity.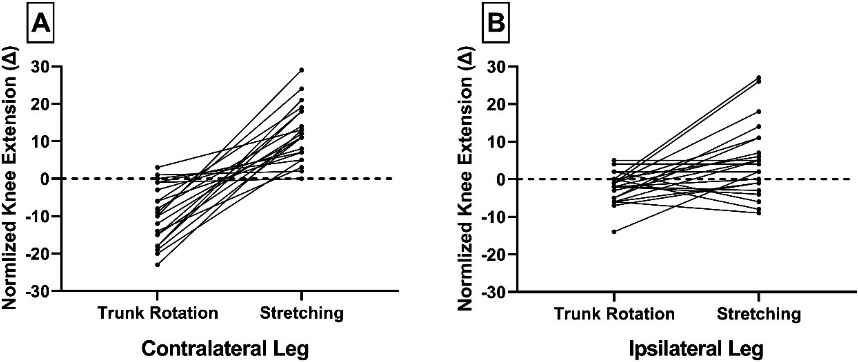
In the ipsilateral leg, there was no significant difference in KE ROM between trunk rotation and neutral position and between stretching and neural position. However, there was a significant difference when comparisons between trunk rotation and post-stretching were made. Pain was significantly greater during trunk rotation than during the other two conditions. Unexpectedly, there were changes on the ipsilateral side to some extent in addition to the contralateral side, which might be due to multiple layers of passive connective tissues and the distinctive direction of each layer [25]. In fact, the TLF connecting the upper and lower bodies is composed of three layers, each with different fiber directions. In the aforementioned structure, an ‘x’ shape is observed in the superficial lamina of the posterior layer of TLF, and fibers are spread in a fan-shape in the deep lamina, some of which is near vertically aligned [17, 29, 30]. The present study we have simultaneously performed trunk rotation and slight flexion for the effective stretching of the upper portion of the POS. Trunk flexion might have elongated the passive connective tissues of the posterior upper body on the ipsilateral side to some extent. A number of other studies have already demonstrated the effect of stretching in the sagittal plane on KE ROM [7, 10, 31]. In addition, it is also known that neural tissues as well as passive connective tissues affect KE ROM [16]. In normalized KE ROM, values measured in a sitting position with trunk rotation and those measured after stretching are normalized to the value measured in sitting with a neutral pelvic position. It was observed that KE ROM generally increases after stretching in comparison to trunk rotation (Fig. 4). Intriguingly, KE ROM decreased from 21.1
This study has some limitations. First, EMG activity was not measured. Second, all the subjects in the present study were healthy adults. Third, some studies have suggested that ROM increases after stretching may be due to increased pain tolerance instead of increased tissue extensibility [34, 35, 36], which should be further verified through testing passive stiffness and torque [37, 38].
In this study, the tensile force in the upper body significantly affected tissue extensibility in the lower extremity in the contralateral side, leading to the restriction of active maximum KE. In addition, the stretching effect was observed not only in the contralateral leg, but also in the ipsilateral leg to some extent. In clinical practice, stretching can be applied to the upper portion of POS on the contralateral side when KE ROM is restricted. Additional stretching on the ipsilateral side, if possible, may enable substantial increases in KE ROM.
Ethical considerations
All study procedures were approved by the Institutional Review Board of Woosong University (approval number: 1041549-200107-SB-82, approval date: January 8
Funding
This research was supported by 2020 Woosong University Academic Research Funding.
Footnotes
Acknowledgments
The author has no acknowledgments.
Conflict of interest
The author has no conflicts of interest to report.