
Abstract
BACKGROUND:
Postural control deficits are prevalent in children with hemiplegic cerebral palsy (CwHCP). Therefore, the best rehabilitative strategies for remediating these deficits are warranted, which could then enhance function.
OBJECTIVE:
To examine effects of a block versus an alternating sequence of balance training (BT) and plyometric training (PT) on postural control in CwHCP.
METHODS:
Forty-eight CwHCP (812 years) were randomized to a block or an alternating BT/PT training. The block BT/PT group (
RESULTS:
The block BT/PT group showed greater enhancements in postural control variables [RT (
CONCLUSION:
The block BT/PT sequence is more effective to enhance postural control than the alternating sequence in CwHCP.
Keywords
Introduction
Cerebral palsy (CP), a frequent developmental disability that is seen in 2–2.5 children of every 1000 live births. Insults or malformations of the immature brain, which mostly occurs before or shortly after birth are the main causes of CP. It is unprogressive but frequently results in a long-term physical disability that affects movement and posture [1]. Spastic CP is an increasingly widespread type affecting up to 80% of the cases, often sub-classified to several types with reference to the affected limbs. Hemiplegic CP (h-CP) delineates the type in which the motor function of one side is impaired and represents about 38% of all spastic CP diagnoses [2].
CwHCP display postural control problems, largely interfering with the performance of daily functional activities [3, 4, 5, 6, 7]. Although factors which contribute to postural control deficiency in those children are variable, they generally include hypertonia, lack of selective motor control, muscle weakness, muscle imbalance, abnormal muscle-activation strategies, deformities and contractures, and vestibular and visual deficits [4, 8, 9, 10]. Effective postural control occurs when a continuous integration exists between the nervous system (which convey the somatosensory, vestibular, and visual signals) and the musculoskeletal system. Impairments of these fundamental systems damage this integration, resulting in a negative impact on postural control in CwHCP [11, 12].
While postural control is the principal element in keeping up with daily functional activities [13], studies to define the best rehabilitative interventions to remediate postural control dysfunctions are warranted. The latest rehabilitation models have shown that balance and strength training ought to be incorporated into exercise regimens for CwHCP [8, 11, 14, 15, 16, 17, 18]. Antecedent investigations on the implications of balance training (BT) alone on postural control revealed meaningful improvements in the majority of measured variables [8, 11, 14, 15]. For instance, Shumway-Cook and colleagues [8] conducted a BT program (i.e., balance perturbation through a horizontal translation of a force plate forward and backward) in children with diplegic and hemiplegic CP. From pre- to post-training, the capacity to recover postural stability improved significantly in all children. In like manner, Woollacott et al. [11] explored the influence of an intensive BT program and reported improvements in directional specificity of postural muscle response and muscle-activation velocity, emergence of proximal-distal muscle sequencing, and reduction of abnormal co-activation, allowing faster recovery of postural stability.
In terms of plyometric training (PT), a series of studies by Elnaggar et al. [16, 17, 18, 19] investigated the effectiveness of a 2- and 3-month PT program encompassing a combination of horizontal and vertical hopping and jumping exercises in CwHCP. In comparison with the active controls, muscle strength, weight-bearing symmetry, gait performance, muscle-activation strategy, and response capacity to balance threats, all improved significantly after training. Also, Johnson et al. [20] studied in a single-subject trial the effectiveness of a PT program in CwHCP. Following 8–14 weeks of PT, improvements in gross motor abilities, lower limb muscle strength, and agility were observed. Further, Ramirez-Campillo et al. [21] analyzed the influence of PT in a group of healthy adolescents. The PT induced significant enhancements of muscle power and balance control.
There is evidence that the manifold physical demands of CwHCP (like strength/power, balance, and related functional aspects) require multi-modal training approaches [18]. In view of this, incorporation of balance and plyometric training appears to be an appropriate possibility, especially since the impact of their underlying neuromotor adaptations would most likely be intensified [22, 23]. As far as is known, a single study exists on the integrational effect of plyometric and balance training in CwHCP. The study revealed meaningful improvement in motor function when both training approaches were integrated within the same session [18]. However, no proof of their sequencing effect exists. A block sequence of balance followed by plyometric training (that is, BT for several consecutive weeks followed by PT for an equal number of weeks), on one hand, could be efficient considering that the BT-induced adaptations may have a preconditioning effect on the consequent PT-induced adaptations (for instance, enhanced ankle muscles activation, a muscle group that is heavily engaged in plyometric activities) [24, 25]. On the other hand, it is unclear whether, on using an alternating sequence (i.e., change of BT/PT on a one- or two-week basis), these positive effects would initiate earlier, thereby it could be more efficient compared to the block sequence. This study was, therefore, endeavored to evaluate the potential efficacy of a block versus an alternating sequence of BT and PT on certain aspects of postural control in CwHCP.
Methods
Experimental design
Forty-eight children were recruited from the four local hospitals, Al-Kharj, KSA. They were included on the basis of the following criteria: age of 8–12 years, affirmed diagnosis of hemiplegic CP [26], Gross Motor Function Classification System (GMFCS) level I or II, corresponding to independent walking [27], mild spasticity (that is, rated as level 1 or 1+ on the Modified Ashworth Scale) [28], impaired postural control as per a tilt board balance test (i.e., the average degree of tilt in all directions is 32.1
The sample size was estimated via a preliminary power analysis by means of PASS software (NCSS, LLC. Kaysville, UT, USA), version 15.0.5. Using a two-sided, independent-sample equal-variance
Children were assigned randomly into two groups: the block group (
Participants
This was a randomized, single-blind clinical investigation performed between January 2018 and March 2019 at the University Labs and Physical Rehabilitation Center. The Institutional Review Board approved the study (Protocol No. RHPT/0017/0054). The research methods adhered to the 1975 Declaration of Helsinki’s ethical guidelines. Children and their families were given a full explanation of the study’s goal and experimental methodology. Before enrollment, children and their legal guardians gave their written informed consent.
Elaboration of the block balance and plyometric training paradigm
Elaboration of the block balance and plyometric training paradigm
Specification of the alternating balance and plyometric training paradigm
Postural stability
The NeuroCom Balance System (NeuroCom
Reaction time (RT, sec); indicative of the time between the order to move (i.e., the appearance of the visual cue) and the first movement of the CoP in the direction of the target. Movement velocity (MV, degree/sec); suggestive of the velocity of CoP displacement. Maximum excursion of CoP (ME, % of the test target); denotative of the maximal distance that the CoP moved toward the planned direction. End-point CoP excursion (EE, % of the test target); characteristic of distance traveled by the CoP in the direction of the target during the first sustained excursion. Directional control (DC, %); pointing out to the extent to which the CoP was controlled (on-axis/off-axis) during the initial excursion.
The pediatric balance scale (PBS) was employed for functional balance assessment during steady-state and anticipatory balance activities, with or without visual input. The test has been shown to be reliable in children with mild-to-moderate motor impairments at the school-age [29, 30]. The scale consists of 14 criterion-referenced items that assess dynamic balance in tasks resembling the daily living activities. Item level scores range from 0 (unable to complete the activity without assistance) to 4 (able to complete the activity independently). The aggregate PBS score is calculated by summing all items’ scores, and ranges from 0–56, with 56 being the perfect score suggestive of best postural control. All children were evaluated by the same examiner as per the sequence suggested by the scale.
Characteristics of participating children
Characteristics of participating children
Abbreviations: BMI: body mass index, MAS: Modified Ashworth Scale, GMFCS: gross motor function classification system, RT: right, LT: left, Continuous data are shown as mean
Gait balance and fall risks were measured using the dynamic gait index (DGI). The DGI is a valid, feasible, and easy to administer measuring tool, evaluating the capability to adapt to different tasks during walking in children aged 8–15 years [31]. The DGI is made up of eight items, each of which is rated on a 4-point scale (severely impaired
Intervention
All children received a training program that lasted for 12 weeks, repeated twice/week, separated at least with 48 hours. The training included a lower limb-focused strength and agility exercises as well as balance exercises. The block BT/PT group performed balance exercises for six weeks succeeded by plyometric exercises in the next six weeks (as shown in Table 1). While, the alternating BT/PT group performed the same exercises, but in an alternating sequence, which was changed every two weeks between balance and plyometric training (as demonstrated in Table 2). Each training program lasted in total for 45 minutes consisting of 10-minute warm-up exercises such as static/dynamic stretching exercises and submaximal bicycle or treadmill raining based on children’s preference, 30-minute balance, or plyometric training, and 5-minute cool-down exercises in the form of flexibility and low-intensity jogging exercises.
The plyometric exercises were prescribed as per the National Strength and Conditioning Association Guidelines [32], and as delineated in a prior study that included individuals with CP [16]. The training was conducted at the same time for all children (between 9–11:30 am), and the progression of exercises was done by increasing the number of repetitions and duration of each exercise. A pre-training explanation of the proper execution of exercises was given to all children. The training programs were carried out under the supervision of two experienced pediatric physical therapists.
Changes in the postural stability variables in both intervention groups
Changes in the postural stability variables in both intervention groups
Data are expressed as mean
Postural control proxies pre- and post-treatment in the block and alternating balance/plyometric sequence groups.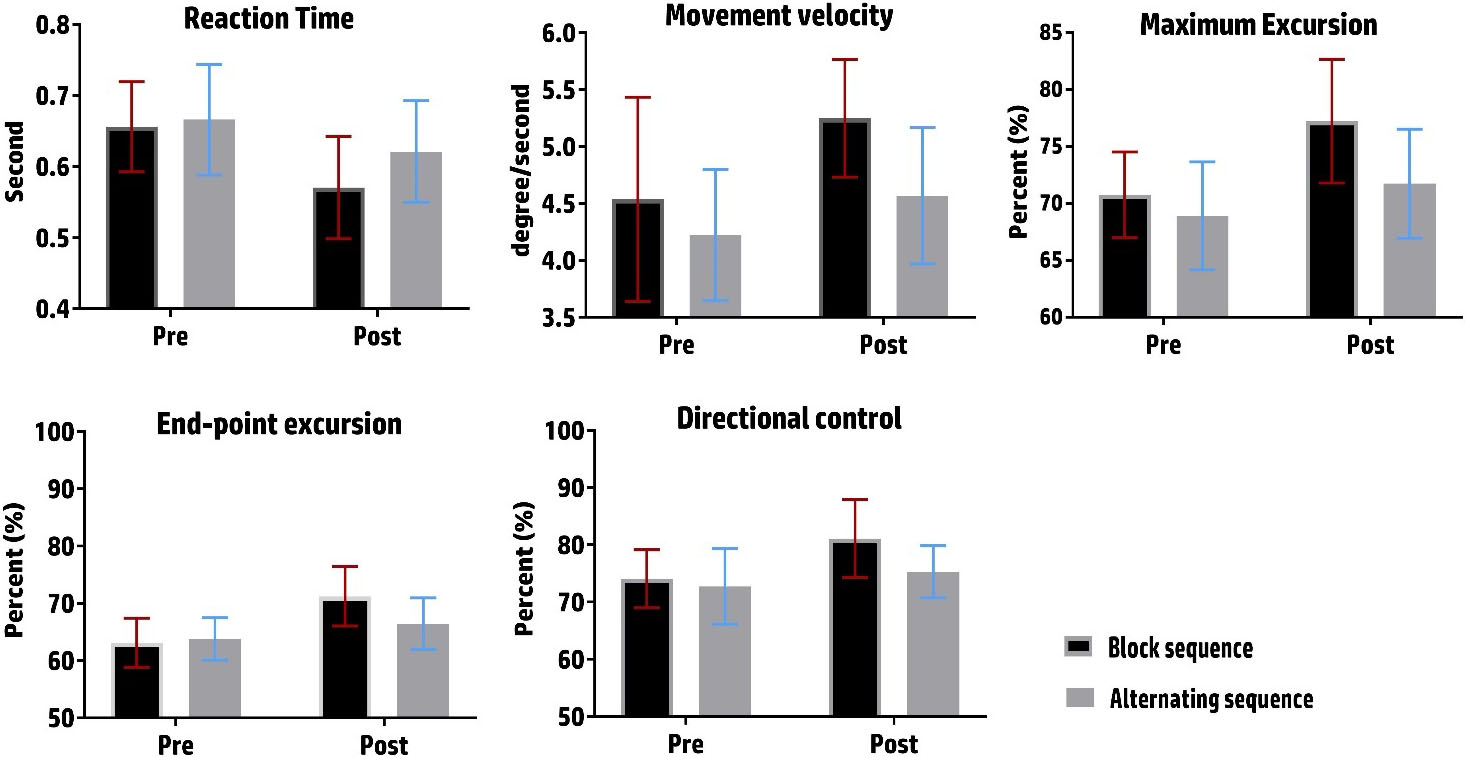
The balance training paradigm included static balance control and DLoS training. Static balance control exercises included heel-to-toe standing on a balance beam, one-leg stance on an Airex
Changes in the PBS and DGI values in the intervention groups
Data are expressed as mean
Pediatric balance scale (PBS) and dynamic gait index (DGI) scores pre- and post-treatment in the block and alternating balance/plyometric sequence groups.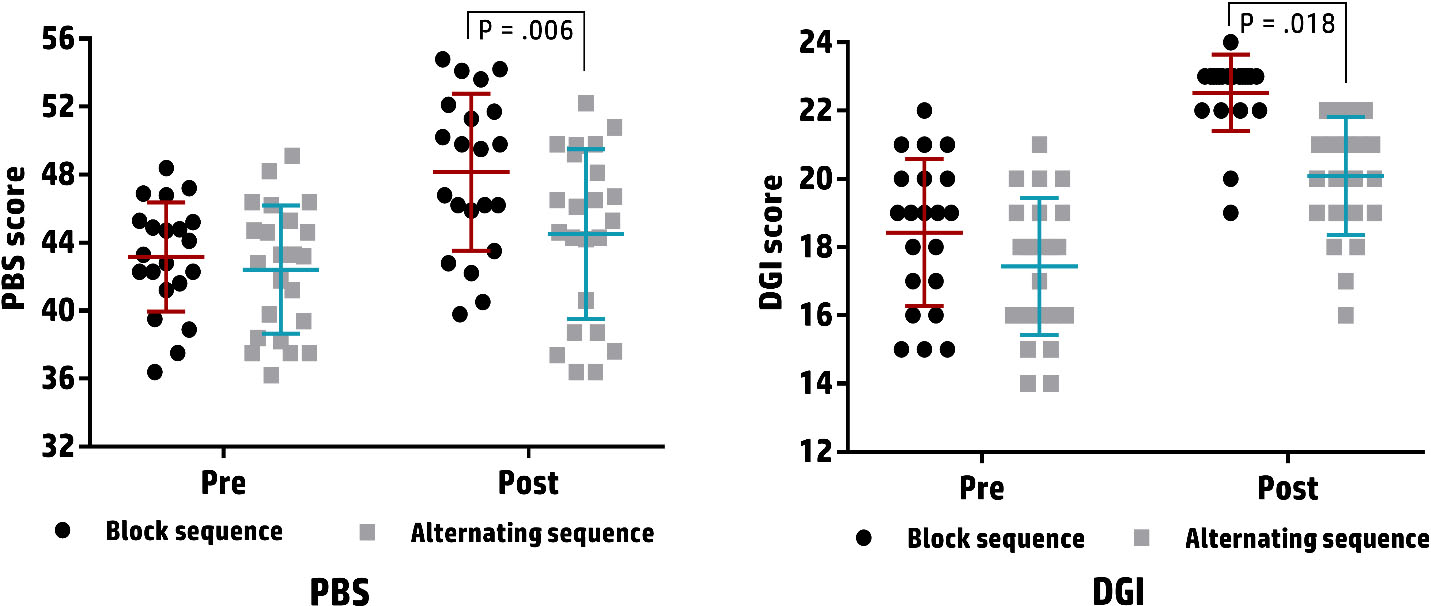
D’Agostino-Pearson omnibus test was used to compute the skewness and kurtosis of all data sets and to quantify how far data have deviated from normality. The two-way split-plot ANOVA was employed to estimate the difference between groups and to determine if an interaction exists between the treatment (block BT/PT, and alternating BT/PT) and the time (pre, post). When a significant interaction effect was confirmed, a group-specific post hoc test (dependent sample
Results
Of 76 children screened in the initial phase, 48 fulfilled the eligibility criteria and were assigned randomly to the intervention groups. However, four children (8.3%) were lost and 44 (91.7%) completed (21 in the block and 23 in the alternating BT/PT groups). The reasons for withdrawal were unknown for two children, transportation issues for one child, and moving outside the working area for one child. At the baseline, the two intervention groups were equivalent with respect to the age, anthropometry (weight, height, and BMI), or clinical features (level of motor function, grade of spasticity, and paretic side) (all
Table 4 displays changes in the measures of postural stability in both intervention groups. The analysis revealed a significant treatment-by-time interaction effect on RT [
Table 5 demonstrates the changes in the PBS and DGI values in both intervention groups. The mixed ANOVA test revealed a significant treatment-by-time interaction effect on PBS [
Discussion
This study aimed at investigating the effect of a block sequence of BT and PT versus an alternating sequence on postural control in CwHCP. In this regard, proxies of postural control (RE, MV, ME, EE, and DC), functional balance (i.e., PBS), and dynamic gait balance (i.e., DGI) have been assessed in CwHCP who either received 12 weeks of block BT/PT (6 weeks for BT followed by another 6 weeks for PT) or alternating BT/PT (a series of alternating BT and PT changed every 2 weeks). The main findings showed that both training sequences yielded enhancements in all postural control variables, functional balance, and dynamic gait balance post-intervention favoring the block BT/PT group. Improvements were large for the block BT/PT group and were small-to-large for the alternating BT/PT group.
In conformity with the initial hypothesis, the present report revealed that the combination of BT and PT in both training conditions enhanced the postural control variables and dynamic balance and reduced the risk of falls during walking in CwHCP. This observation matches well with the findings of previous research integrating balance and strength training in the physical care of children with CP or other developmental disorders. For instance, Auld and Johnston [33] noted that the multimodal intervention of both balance and strength training for eight weeks, in children with CP, had the potential to produce significant improvements across the balance and strength variables. Elnaggar et al. [16, 18] suggested that integrational approaches of strengthening exercises with advanced-balance and postural-correction exercises are effective in enhancing muscle strength, the symmetry of body-weight support on lower extremities, balance capabilities, and walking efficiency in CwHCP. Granacher et al. [34] proposed that combining balance and strength training is more successful in counteracting neuromuscular constraints and encouraging posture stability and strength in children with balance deficits. Gupta et al. [35] pointed out that six weeks of integrated strength and balance training produced favored outcomes regarding strength and balance in children with Down’s syndrome. Furthermore, the results herein fit with the findings of prior researches on the combinatory effects of BT and PT in normal children, where larger improvements in balance and muscle strength have been reported in comparison with the single-mode training conditions [36, 37].
The sequencing effect of BT and PT has not been previously assessed in children with CP. However, there is evidence indicating that the order of BT and PT has differential effects on muscle strength and neuromuscular activation [38]. More specifically, the block BT succeeded by block PT yielded better improvements compared to the reverse sequence, which corroborate the results from CwHCP in the present study. The plausible explanation is that, during the block BT/PT, the augmented neuromuscular activation triggered by BT for six consecutive weeks might have optimized the muscle power production during PT in the subsequent six weeks by what is called the “pre-conditioning effect” [18, 39]. That is, BT in the block sequence reached the highest intensity after six weeks, which may have allowed for intense afferent proprioceptive feedback, enhanced lower limb muscle activation, and consequently faster and more intensive activation of the neuromuscular system during the following PT [40], which probably resulted in better improvement of postural control. While, in the alternating schedule, BT was applied interchangeably with the PT in two-week sequences (i.e., reached the maximum intensity after 12 weeks), which was not sufficient to induce comparable effects, possibly because of the interference effect–that is, the change of BT with PT every couple of weeks is likely to interrupt adaptations specifically induced by the BT versus those related to the PT.
Hammami et al. [39] investigated healthy adolescents (12–13 years) who performed either a 4-week BT succeeded by a 4-week PT or conversely. They observed that PT preceded by BT produced considerably greater enhancements in reactive muscle strength, leg stiffness, and balance control when contrasted to the opposite order. Muehlhauser et al. [41] trained athlete adolescents in either a block or alternating BT/PT sequence for six weeks. The results proved favorable impacts of the block BT/PT sequence on some balance and muscle strength variables compared to the alternating sequence. Despite the methodological differences, findings from CwHCP may support the results of previous investigations indicating that block BT followed by block PT is a potentially more effective training paradigm than vice versa. In addition, this study provides experimental evidence corroborating the findings of previous studies that suggested that, because children’s balance and coordination are immature and balance is necessary for optimum execution of function, strength training should come after the BT [42, 43].
On the question of the influence of both training regimens on functional performance, this study found that the block BT/PT schedule brought on more conducive responses (i.e., higher PBS and DGI scores) in comparison with the alternating sequence. Considering the link between postural control and functional capacity in children with CP [44], it is possible that the higher levels of postural stability associated with the block BT/PT promoted the elaboration of more proficient functional skills. Supporting this claim, are the published reports which revealed that postural control is a crucial determinant in gross motor abilities and walking efficiency in children with CP [18, 19, 44, 45]. And more, it has been proved that with further development of postural control, children with CP become more capable of performing the necessary anticipatory adjustments for optimal execution of functional tasks [44].
The results of the present study have significant implications for the understanding of how the sequence in which the balance and plyometric exercises are administered has a differential bearing on motor function development in CwHCP. Despite the fact that both training regimens (balance and plyometric) result in neuromuscular changes [22, 23, 38], adaptation seems to be task- and/or training-specific. In other words, BT over several consecutive weeks leads to a reduction in the corticospinal excitability explosive strength training for several weeks results in enhancement of the corticospinal activation [46]. BT for six weeks followed by plyometric training for six weeks likely to be appropriate for reducing the interfering effects of neuromotor adaption patterns while promoting the therapeutic benefits. Accordingly, physical therapists are advised to employ a BT/PT sequence instead of the opposite or the alternating sequences if the goal is to help CwHCP improve their motor skills.
Certain limitations should be considered when interpreting the findings of this study. First, the findings are limited to a specific type of CP (h-CP) with a relatively good gross motor function and less restrictions when it comes to physical activity than other types of CP [47]. Second, the analysis was limited to the studied age group (i.e., 8–12 years). The author cannot, therefore, report on the responses of children with other forms of CP or even CwHCP whose age is more or less. Third, this study lacks a control (no-training) group as this was declined and has been classified as unethical by the reviewing committee.
Conclusion
Using either the block or the alternating BT/PT sequence is documented to enhance postural control, improve functional balance, and reduce the risk of falls during walking in CwHCP. Nonetheless, evidence from this study suggests that the block BT/PT sequence is a potentially more effective training paradigm. Further examinations to determine the training-related adaptations in other types of CP representing different age-categories remain necessary to substantiate the observations of this study.
Author contributions
CONCEPTION: Ragab K. Elnaggar.
PERFORMANCE OF WORK: Ragab K. Elnaggar, Mshari Alghadier and Alshimaa R. Azab.
INTERPRETATION OR ANALYSIS OF DATA: Ragab K. Elnaggar and Reham H. Diab.
PREPARATION OF THE MANUSCRIPT: Ragab K. Elnaggar, Mshari Alghadier, Reham H. Diab and Alshimaa R. Azab.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ragab K. Elnaggar and Mshari Alghadier.
SUPERVISION: Ragab K. Elnaggar and Alshimaa R. Azab.
Ethical considerations
The Institutional Review Board approved the study (Protocol No. RHPT/0017/0054). Before enrollment, children and their legal guardians gave their written informed consent. The research methods adhered to the 1975 Declaration of Helsinki’s ethical guidelines.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Footnotes
Acknowledgments
The authors are grateful to the children and their parents/legal-guardians for their enthusiastic participation in this study.
Conflict of interest
The authors declare that there is no conflict of interest.