
Abstract
BACKGROUND:
Stretching is commonly used for clinical and sports reason but the effects vary on time and the technique used.
PURPOSE:
To determine the acute effects of static and dynamic stretching of gastrocnemius muscle on muscle-tendon unit (MTU) and dorsiflexion range of motion (ROM) in the same individuals; to find out how long the stretching effects endure.
METHODS:
Twenty-eight males (mean age: 22.18
RESULTS:
Muscle thickness and pennation angle did not change over time with either techniques (
CONCLUSION:
We recommend using the dynamic stretching technique to achieve greater and longer lasting increases in tendon length and range of motion.
Abbreviations
Introduction
Muscle stretching is applied to enhance range of motion (ROM) and to reduce risk of injury in sports [1, 2, 3] or used as a therapeutic approach for many clinical conditions [4, 5, 6, 7, 8]. It can be performed in either a static or a dynamic manner. While the muscle is held in its lengthened position for some period in static stretching (SS), in movement-based dynamic stretching (DS) the muscle is relaxed and elongated via reciprocal inhibition of its antagonist’s contraction, without being held in the end position [9, 10].
Despite conflicting results regarding performance [9, 11, 12, 13, 14, 15, 16, 17] and injury prevention [3, 18, 19, 20], it is reported that flexibility and ROM can be improved by static stretching as a consequence of the decrement in muscle stiffness [21, 22, 23, 24]. Recent studies suggest the use of dynamic stretching if one avoids strength loss [25, 26, 27].
However, effects of stretching depend on the type, duration, position and timing of stretching and there is still debate over which prescription provides the best results in terms of flexibility, power, sports performance and injury protection [18, 28]. In addition, there is no consensus regarding which one is mostly affected, muscle or tendon, by stretching.
Various test methods (e.g. jump test, dynamometer, electRoMyography) are used to observe stretch-induced results [15, 16, 29]. Ultrasound seems to be a good option as it offers a objective and non-invasive way to observe the change in muscle and tendon due to stretching [30].
Limited number of studies exists in literature investigating the viscoelastic changes of the stretched muscle via ultrasound after different stretching techniques or the time-course of the stretching results.
This study was performed to determine the acute effects of static and dynamic stretching of gastrocnemius muscle on muscle-tendon unit (MTU) and dorsiflexion range of motion in the same individuals and to find out how long the stretching effects are sustained.
Methods
Subjects
This study complied with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee at Tokat Gaziosmanpasa University, Faculty of Medicine (Project No: 15-KAEK-025).
Twenty eight males [mean age: 22.18
Method
Outcome measures
Muscle-tendon unit properties of gastrocnemius muscle were assessed via ultrasound and recorded as the baseline values. Dorsiflexion range measurement was measured using a universal goniometer [31].
Ultrasound measurement
A radiologist (E.G.) assessed muscle-tendon junction (MTJ) displacement, muscle thickness and pennation angle via ultrasound which was taken in the scope of Scientific Research Project.
A real-time ultrasound (Toshiba Aplio 500, Otawara, Japan) was used to observe the position and the changes in the MTJ before and after stretching exercises. The device had a 9-MHz linear type probe (PLT 805 AT) with a 55-mm wide field of view. Each participant stood up on a hard ground with his feet placed parallel. Initially, ultrasound probe was placed at the achille tendon-medial gastrocnemius junction level and then caudal edge of the probe was marked with a permanent marker. This marked point was used for all ultrasonic measurements. MTJ displacement was calculated by measuring the distance between new MTJ position and the reference point [1]. The muscle thickness was defined as the distance between the deeper and upper aponeuroses and was measured at the MTJ [1]. The pennation angle of muscle was measured as the angle of insertion of the muscle fiber fascicles into deeper aponeurosis [32]. Muscle thickness and pennation angle measurements are shown in Fig. 1 and MTJ displacement, in Fig. 2.
Muscle thickness (A) and pennation angle (B).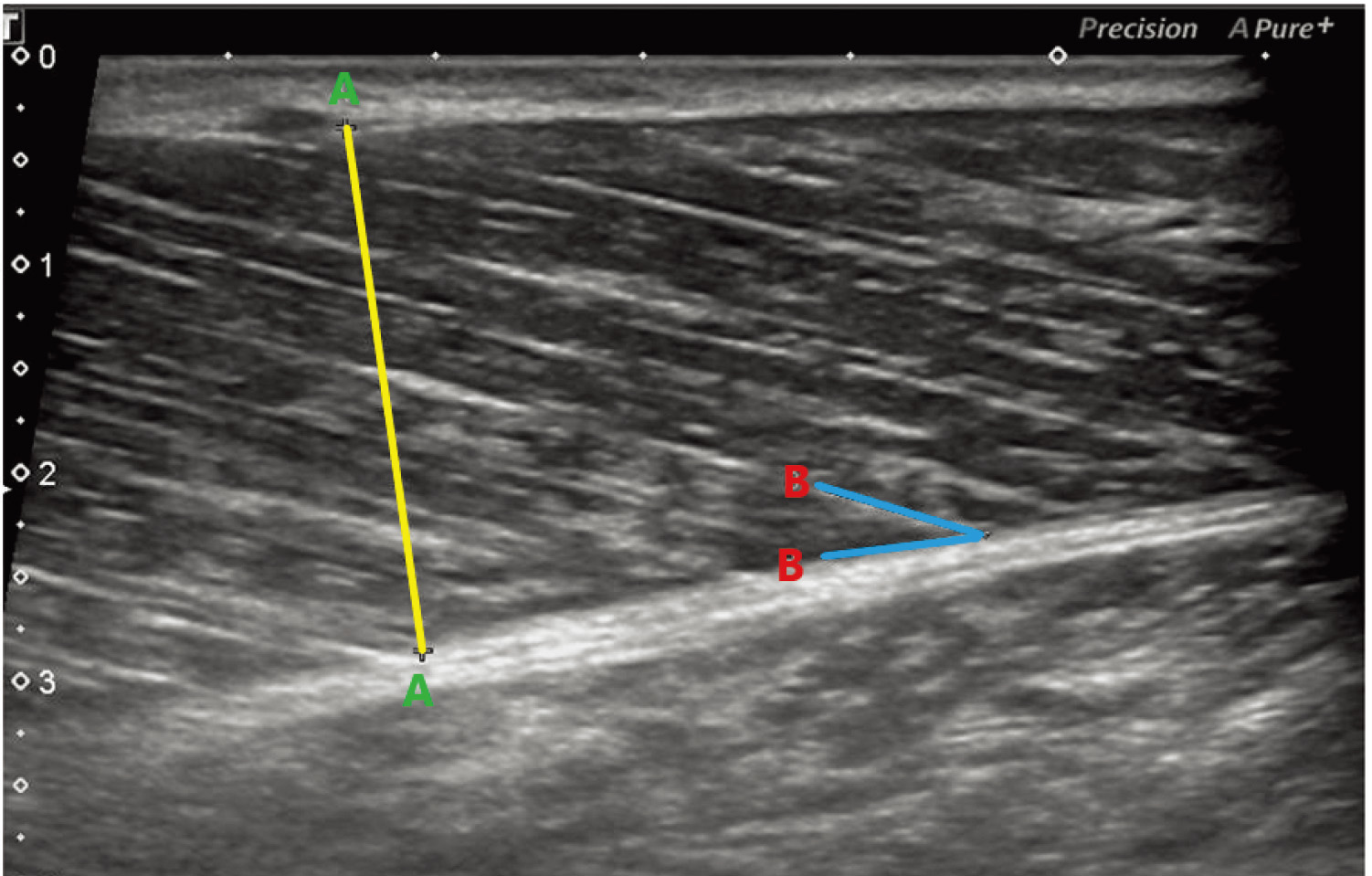
Ultrasonographic images of the MTJ of medial gastrocnemius. The “D” indicates the proximal displacement of the MTJ right after dynamic stretching.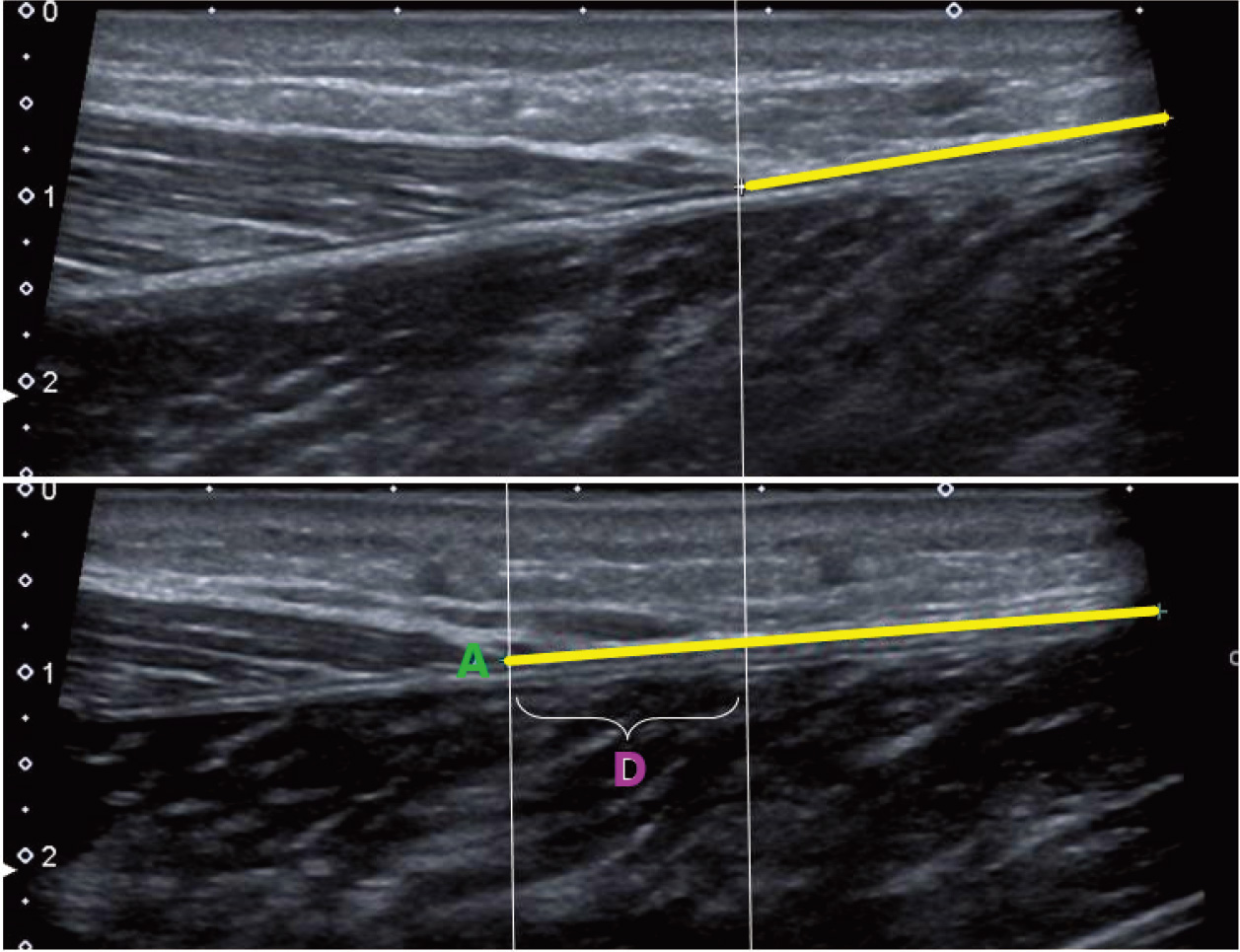
Goniometric measurement
Goniometric measurements were performed by the physiotherapist (F.D.). A universal goniometer was used to assess active and passive dorsiflexion range. The measurement was performed in non-weight bearing position. Participants lied in supine position. A roll shaped towel was placed under the knee to give slight flexion to the knee and relax the gastrocnemius muscle as it is a double-jointed muscle. Lateral malleolus was determined as the pivot point. The foot was brought to its neutral position of 90
Static stretching
After a 5-min warm-up period, static stretching was applied to participants’ gastrocnemius muscles on their right limbs. Participants lied in supine position and a physiotherapist (F.D.) took the ankle to dorsiflexion position until the end point. Each stretch was held for 45-s and repeated five times. There was a 15–20-s rest period between each stretch. The intensity of stretching was set to the threshold of mild discomfort, but not pain, as acknowledged by the participant. Ultrasonographic and goniometric measurements were repeated right after, 5-min, 15-min and 30-min after the stretching in order to see how long the stretching effect is sustained.
Dynamic stretching
After a few days, the same participants were assessed to see the effects of dynamic stretching. Participants performed dynamic stretching on their left sides this time in order to eliminate possible post-stretching effects or injuries on the right leg. Following a 5-min warm-up period, dynamic stretching exercises were performed based on the stretching protocol at Samukawa’s study [1]. Participants raised their left foot off the floor, extended their knees and performed active dorsiflexion and plantar flexion of their left ankle joints with a rhythm of 1 beat per second using a metronome. Dynamic stretching of 45-s was repeated 5 times. Between each set, participants rested their legs for 15–20-s. Ultrasonographic and goniometric measurements were repeated right after, 5-min, 15-min and 30-min after DS, as performed after the SS protocol.
Statistical analysis
Continuous data are expressed as mean
Results
The trial was completed within a week without any adverse effect or event. The physical characteristics of participants are presented in Table 1. Neither muscle thickness (Table 2) nor pennation angle (Table 3), varied over time (
Physical characteristics of volunteers
Physical characteristics of volunteers
Measurement results of muscle thickness
Group effect:
Measurement results of pennation angle
Group effect:
Measurement results of muscle-tendon junction (MTJ) displacement
Group effect:
However, MTJ displacement was significantly higher after dynamic stretching (
Goniometric measurement results of active dorsiflexion
Group effect:
Goniometric measurement results of passive dorsiflexion
Group effect:
Active dorsiflexion range increased over time with both techniques (
The results of our study indicate that muscle thickness and pennation angle values did not significantly changed but MTJ displacement occurred after the techniques; the highest change was achieved after DS. Although both techniques improved active range of motion values similarly, only dynamic stretching succeeded in increasing passive range of dorsiflexion motion significantly. The time course analysis indicated that active ROM, passive ROM and MTJ displacement values at 30
Pennation angle and fascicle length are generally used to determine change in muscle architecture [32, 34]. Our outcomes indicated that both stretching exercises affected “the tendon” essentially, not the muscle; as Samukawa et al. [1] previously reported, too. Similar to our findings, they found no change in pennation angle and fascicle length of plantar flexor muscle but a significant displacement of the MTJ and an increase in passive dorsiflexion angle, after dynamic stretching exercises of 30-s and 5 sets. The change in MTJ displacement was sustained until the second set but time course of the change in ROM was absent as it was not measured after each set [1].
Mizuno et al. [35] achieved an immediate increase in passive dorsiflexion ROM after static stretching of 1-min, performed 5 times. Muscle stiffness was reported to decrease and MTJ displacement increase (arguably due to increment of muscle length and decrement of tendon length) but these improvements returned within 10-min, although the gain in ROM sustained over 30-min. Similar results were showed in other studies of Mizuno et al., consisting of dynamic stretching exercises of various duration and set numbers [36, 37]. They stated that these results were due to the enhanced stretch tolerance, rather than viscoelastic changes of MTU.
Nakamuro et al. [38] reported an immediate and prolonged (10-min later) decrease in MTU stiffness of gastrocnemius muscle, with static stretching of 5-min. This decrease was attributed to the decrease in muscle stiffness, not to that in tendon. Fascicle length remained unchanged, but ROM was not evaluated in the study. Ryan [39] also studied the time course of stretching and found that ROM increased immediately after stretching, regardless of different stretching duration but the effects disappeared within 10-min. Nakao et al. investigated the acute effects of static stretching of active and passive knee extension on shear elastic modulus of hamstring muscle and maximum knee extension ROM. They indicated that the maximum ROM increased and shear elastic modulus decreased after both stretching without superiority between the techniques [40].
In the current study both techniques were applied to the same individuals in order to eliminate morphological differences [34, 41]. And unlike most of the studies involving stretching session of 30-s and stating that post-stretching achievements disappeared within 10-min [18, 39] we applied stretching for 45-s to find out whether the results would last longer if the stretch was prolonged.
As mentioned above, post-stretching changes, like increase in ROM, are mostly attributed to the viscoelastic properties of muscle-tendon unit [30, 42, 43] and to neural mechanisms [44, 45, 46]. Some of the studies analysing acute effects of stretching suggested that the increase in ROM was due to muscle compliance based on the change in pennation angle and fascicle length [34, 38], or a decrease in muscle stiffness [39]. Those who failed to find any change in pennation angle and fascicle length reported that elastic component of connective tissue elements within muscle was responsible from RoM increase [38, 47, 48] while some authors stated that stretching affected the tendon, primarily, not the muscle [1], supporting our findings.
In addition to the mechanism of action, exhibiting the technique difference in ROM and MTJ results constitute the main issue in this study. While stretching of a muscle in a static manner reveals autogenic inhibition [10] dynamic stretching generates reciprocal inhibition [49]. Thus, reciprocal inhibition is thought to be responsible for the significant difference in MTJ displacement, between the techniques.
According to Cyriax, passive movements test inert structures which include joint capsule, ligaments, fascia, and are generally used to get information about the integrity of contractile and inert structures [50]. It is apparent that various factors other than muscle or tendon also play role in a joint motion.
Chtourou et al. investigated the effect of dynamic and static stretching on diurnal variations of jump performance in soccer players. Hamstring, quadriceps and calf muscles were stretched for 20-s and 3 times. They recorded oral temperature before and after stretching in the morning and in the evening time as core temperature was a chronobiological marker and representing the circadian system. They indicated that the increase in oral temperature after dynamic stretching was significantly higher than that of static stretching. The improvement in muscular performance was attributed to the elevated muscle and body temperature [51].
In a systematic review, static stretching was mentioned as a passive technique which fails to warm a muscle [20].
Based on previous findings [51, 52, 53] we suggest that the compliance of soft tissues (like ligaments and other inert structures) around the ankle due to the rise in temperature obtained by DS, might be responsible for the rise in passive ROM.
The absence of a control group was one of the limitations of our study. Another limitation is that joint movements could not be measured with a dynamometer while inclusion of male only participants of similar ages was another.
Conclusion
Both static and dynamic stretching exercises elongated tendon and improved active ROM, but only dynamic stretching resulted in an increase in passive range of dorsiflexion and created a better lengthening in the tendon. Dynamic stretching seems to affect both contractile and inert structures. Given the results of this study, we recommend using the dynamic stretching technique to achieve greater and longer lasting increases in tendon length and range of motion.
Author contributions
CONCEPTION: Funda Demirturk.
PERFORMANCE OF WORK: Mustafa Kaya, Erkan Gokce and Funda Demirturk.
INTERPRETATION OR ANALYSIS OF DATA: Mustafa Kaya, Erkan Gokce and Funda Demirturk.
PREPARATION OF THE MANUSCRIPT: Mustafa Kaya, Erkan Gokce and Funda Demirturk.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Mustafa Kaya, Erkan Gokce and Funda Demirturk.
SUPERVISION: Funda Demirturk, Erkan Gokce and Mustafa Kaya.
Ethical considerations
This study complied with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee at Tokat Gaziosmanpasa University, Faculty of Medicine (Project No: 15-KAEK-025). Before participation, all procedures had been fully explained and written informed consent was obtained from all volunteers. Clinical Trial Number: NCT02428153.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.