
Abstract
BACKGROUND:
Various interventions have been recommended to increase ankle dorsiflexion range of motion (DFROM); however, few studies have investigated the long-term effects of applying gastrocnemius stretching with talus-stabilizing taping (GSTST).
OBJECTIVE:
To compare the effects of gastrocnemius stretching (GS) and GSTST on DFROM and balance in subjects with limited DFROM.
METHODS:
Twenty-six subjects with limited DFROM were randomly allocated to either the GS group (
RESULTS:
The GSTST group had greater maximum DFROM before heel-off, passive DFROM, and posterior talar glide than the GS group. Gastrocnemius flexibility and YBT-LQ scores increased significantly post-intervention in both groups; however, there was no significant difference between the groups.
CONCLUSIONS:
GSTST is recommend for improving ankle DFROM and balance in subjects with limited DFROM.
Introduction
To perform normal functional activities, an appropriate ankle dorsiflexion range of motion (DFROM) is required [1, 2] alongside a passive ankle DFROM of at least 10
Static stretching [11, 12, 13], mobilization with movement of the talocrural joint [14], and talus-stabilizing taping [15, 16] were used in clinical practice. Static stretching is the most commonly applied clinical method, and a study found that calf stretching with the knee straightened increased the displacement of the myotendinous junction of the calf muscle and increased passive ankle DFROM [11, 12, 13]. Mobilization with movement is used to increase the accessory movement of the talocrural joint; Vicenzino et al. [14] found that the posterior glide of the talus and ankle DFROM increased significantly after applying mobilization with movement of the talocrural joint in the anterior-to-posterior direction. In addition, application of talus-stabilizing taping as a mobilization with movement method has been shown to increase passive DFROM and maximum DFROM before heel-off during walking [15, 16]. Normal DFROM can be maintained by sufficient gastrocnemius flexibility and posterior talar glide; however, static stretching and mobilization with movement focus only on gastrocnemius flexibility and joint accessory movement, respectively.
Both gastrocnemius flexibility and posterior increased talar glide must be considered to improve limited DFROM. Interventions that simultaneously enhance gastrocnemius flexibility and talar posterior glide have also been proposed. Kang et al. [13] found that posterior talar glide and DFROM before heel-off were significantly increased following application of gastrocnemius stretching (GS) with sustained talocrural joint mobilization compared with GS alone; gastrocnemius flexibility and passive DFROM also increased significantly compared with pre-intervention levels. Another study reported that self-mobilization using a strap increased ankle DFROM more than static stretching [17].
Although clinicians have demonstrated that applying static stretching with sustained mobilization and movement of the talocrural joint is an effective method to increase ankle DFROM, the intervention durations in these studies have generally been short [13, 17]. Studies have reported that longer intervention periods of static stretching of the plantar flexors resulted in greater DFROM and gastrocnemius flexibility [18, 19, 20], with DFROM increasing after 6 weeks [18, 19]. In addition, therapists are required to apply talocrural joint mobilization with movement [13], whereas self-stretching using a strap is a mobilization with movement method for the talocrural joint with GS, but with more focus on posterior talar glide [17]. Talus-stabilizing taping is a mobilization with movement method for the talocrural joint that can increase posterior talar glide and ankle DFROM [15, 16] which can be applied with ease. However, no studies have demonstrated its long-term effects in combination with GS. Additionally, although DFROM has a positive correlation with forward dynamic balance, few studies have investigated the effect of static stretching with mobilization and movement on dynamic balance in subjects with limited DFROM.
Therefore, this study investigated the effect of GS with talus-stabilizing taping (GSTST) on improvement of ankle DFROM during walking, passive DFROM, and YBT-LQ scores compared with GS alone.
Methods
Subjects and design
Twenty-six subjects with limited ankle DFROM participated from August 2020 to November 2020 (a period of 4 months). The inclusion criteria were
CONSORT Flow chart of the study.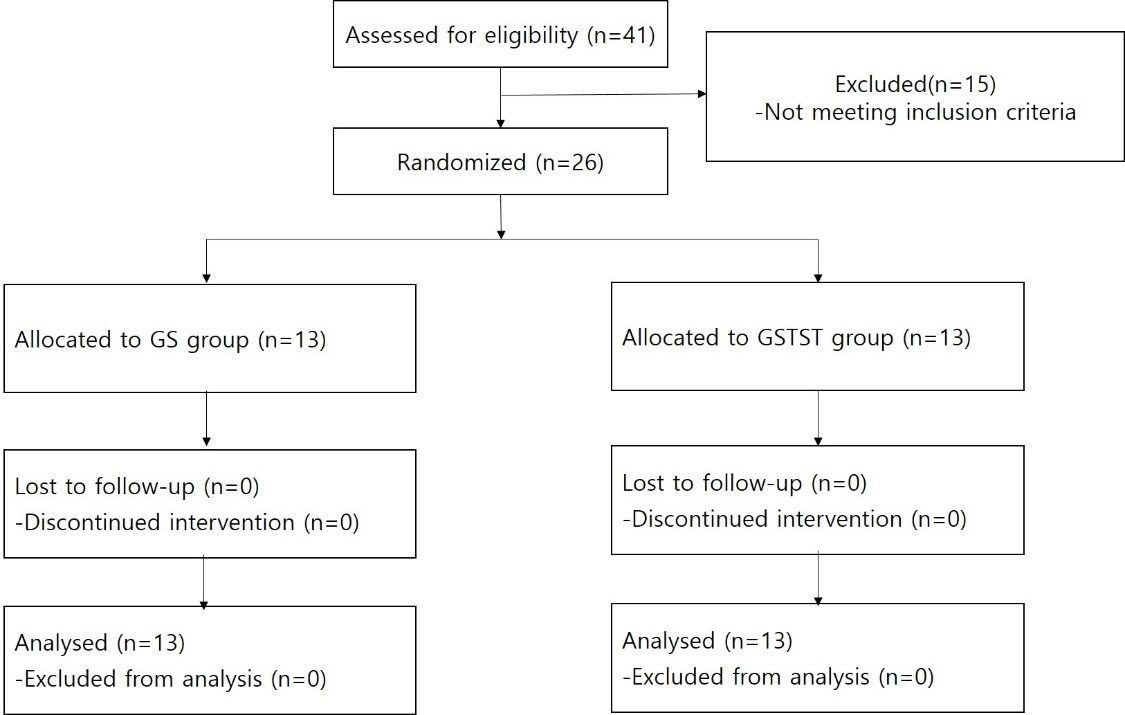
The present study was a researcher-blind, randomized, parallel-group study conducted at Pusan National University Yangsan Hospital. All subjects were randomized to GS group (
The sample size for the study was calculated using the statistical package G*Power 3 based on a previous study [13]. The results of the power analysis (mean difference: 4.69
In this study, primary outcome variables were ankle DFROM before heel-off, passive ankle DFROM, and posterior talar glide. Secondary outcome were gastrocnemius flexibility and dynamic balance. All outcome variables were measured by two investigators except the Y-balance test. Measurements were conducted 3 times with 1 min inter-trail rest interval. The mean value was used for data analysis.
Ankle DFROM before heel-off
A motion analysis system (Motion Analysis Corporation, Santa Rosa, CA, USA) and six infrared cameras were used to measure ankle DFROM before heel-off in mid-stance during walking. Nineteen 14-mm reflex markers were attached to the lower extremities on both sides according to the modified Helen Hayes set. Reflective markers were attached to the anterior superior iliac spine, between the bilateral posterior superior iliac spine, the center of the femur, the medial and lateral epicondyle of the femur, the center of the fibula, the posterior calcaneus, the lateral and medial malleolus, and the toe (between the second and third toes). Static measurements were used to create a static anatomical model. The ankle segment was created using the reflective markers on the lateral malleolus, toe, and posterior calcaneus, and the shank segment was created using markers on the lateral epicondyle of the femur, the fibula, and the malleolus. After attaching the reflective markers, subjects were asked to walk on a walkway at a comfortable pace with bare feet [13]. Subjects performed 5 continuous strides in each trial. During walking, the ankle DFROM was calculated as the movement of the ankle segment from the shank segment using the Cardan angle [22]. While walking on the ground, ankle kinematic data were measured using Cortex software (Motion Analysis Corporation), and the Orthotrak program (Motion Analysis Corporation) was used for data processing.
Passive ankle DFROM
Passive ankle DFROM was measured by two investigators using an electronic inclinometer. When the subjects were placed in a prone position with the knee extended, investigator 2 placed his hand on the plantar surface of the forefoot while keeping the subtalar joint in a neutral position and pushed it to the point where the ankle DFROM ended with a firm end feel. At this point, investigator 3 measured the DFROM by placing the digital inclinometer on the plantar surface of the foot.
Posterior talar glide
Posterior talar glide was measured by two investigators using an electronic inclinometer based on previous studies [13, 14]. Subjects were asked to sit on the corner of a firm table that provided maximum support for the thigh. Investigator 2 pressed on the subtalar joint in a neutral position parallel to the floor. In this position, investigator 2 placed both thumbs on the anterior surface of the talus and applied a posterior talar glide with a subtalar neutral position parallel to the floor until eliciting a firm end feel. Then, investigator 3 placed an electronic inclinometer at the distal part of the tibial tuberosity and measured the tibial inclination angle when tibia movement stopped. Once posterior talar glide was measured, the subjects stood in a comfortable position, then sat back onto the firm table for the next measurement (Fig. 2) [13, 14]. Intra-rater reliability for this method was reported to be excellent (0.97–0.99) in previous studies [13, 14].
Measurement of posterior talar glide.
The Silfverskiöld test was conducted by investigators 2 and 3 to assess gastrocnemius flexibility [23]. The subjects were asked to assume a lying position with the knee extended. Investigator 2 pushed the forefoot surface while maintaining the subtalar joint in a neutral position until the DFROM reached its limit and a firm end feel was elicited. Investigator 3 measured the DFROM by placing a digital inclinometer on the plantar surface of the foot (Fig. 3A). Then, investigator 2 performed the ankle DFROM procedure described above with the subject’s knee bent 90
Silfverskiöld test in supine position (A) and Silfverskiöld test in knee bent 90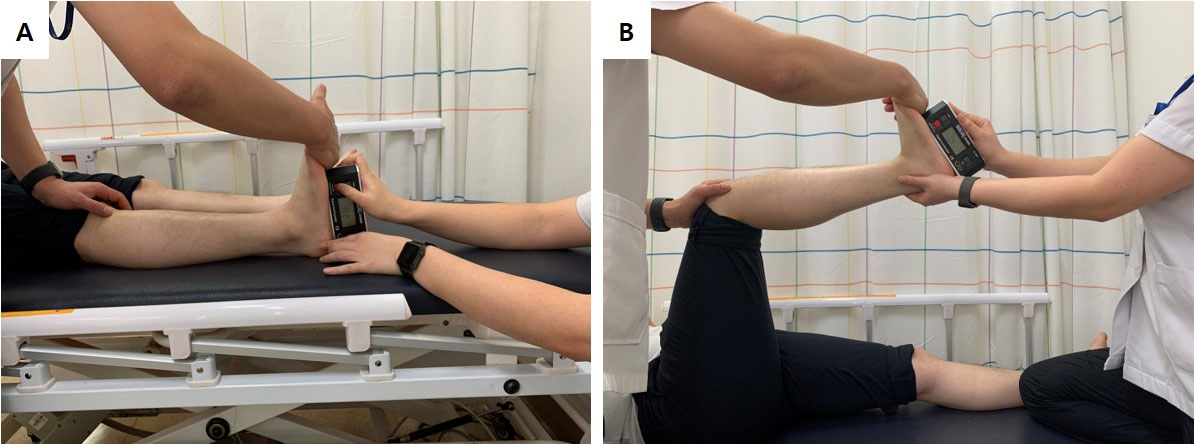
The YBT-LQ was performed using the YBT tool (Y Balance Test Kit; Functional Movement Systems, Inc., Chatham, VA, USA) to assess dynamic balance. Before administration of the YBT-LQ, investigator 2 measured the length of the test-side leg (from the anterior superior iliac spine to the medial malleolus) using a tape measure while the subjects lay comfortably on the bed. After investigator 3 demonstrated how the YBT-LQ is performed, subjects were asked to place the test-side leg on the scaffolding in the middle of the YBT tool while keeping a standing posture and move the non-test-side leg in three directions: anterior, posterolateral, and posteromedial. Investigator 2 measured the distance reached in three directions. Subjects practiced the movements twice before measurements began. Three measurements were taken in each direction, and the farthest-reaching measurement in each direction was used to calculate the scores by dividing it by the length of the lower extremity. If the support foot fell off the scaffold during the examination, the foot of the stretched leg touched the ground, or the leg was stretched and failed to return to the starting position, it was considered a failure and the measurement procedure was conducted again [24]. In previous studies, the reliability of YBT-LQ between and within testers was high [25].
Intervention
Both GS and GSTST were performed by one physical therapist (investigator 4) who had 5 years of experience and appropriate training in both techniques. In the GSTST group, talus-stabilizing taping was performed during GS on a scale to generalize the amount of force applied to the leg on the exercise side. The weight of the exercise-side leg was maintained at 60
Subjects stood on a scale with the exercise leg one step behind the non-exercise leg to perform the GS. To prevent excessive pronation of the subtalar joint on the exercise side, the exercise foot was placed on the tape on the scale to align the second toe and the middle part of the heel in a straight line. In this position, subjects leaned forward with the non-exercise-side knee flexed for maximum stretching in the gastrocnemius on the exercise side (Fig. 4A). During the calf stretch, the subject’s hands were placed on the wall as support to balance the body and prevent the heel from being lifted from the floor.
Gastrocnemius stretching (A) and gastrocnemius stretching with talus-stabilizing taping (B).
The GSTST was performed in same manner as GS except that talus-stabilizing taping was applied (Fig. 4A). The talus-stabilizing taping was applied following previous studies [15, 16]. Subjects put the exercise-side foot on a chair and then flexed the knee to advance the tibia over the foot. In this position, the investigator attached rigid tape (Battlewin tape; Nichiban Co., Ltd., Tokyo, Japan) from the talus of the exercise-side ankle to the plantar surface of the calcaneus (from anterosuperior to posteroinferior) through the lateral and medial sides of the talus. After attaching the talus-stabilizing taping, the subjects performed GS.
None of the subjects engaged in sports activities, performing only activities of daily life during the intervention period. Subjects who did not participate in stretching more than three times were dropped from the study to prevent data distortion. All GS was performed 10 times for 30-s (with 30-s of rest time between stretches) during the 6-week study period.
The statistical analysis was conducted using SPSS version 20.0 for Windows (IBM Corp., Armonk, NY, USA). The Kolmogorov-Smirnov test was used to identify normal distributions in variables. Two-way repeated-measures analysis of variance was used to determine main effects and interactions for ankle DFROM before heel-off, passive ankle DFROM, posterior talar glide, and YBT-LQ score. The within-group factors were time (pre-stretching and post-stretching) and group (GS and GSTST groups). If significant interactions or main effects were found, the
Results
There were no significant differences in the demographic characteristics of the subjects at baseline or in the outcome variables between the GS and GSTST groups (Tables 1 and 2), and all outcome variables were shown to have a normal distribution based on the Kolmogorov–Smirnov test (
Subject demographics
Subject demographics
Abbreviations: BMI: body mass index, GS: gastrocnemius stretching, GSTST: gastrocnemius stretching with talus-stabilizing taping
Baseline measures of all variables for both groups
Abbreviations: DFROM: dorsiflexion range of motion, GS: gastrocnemius stretching, GSTST: gastrocnemius stretching with talus-stabilizing taping, PDFROM: passive dorsiflexion range of motion, YBT-LQ: Y-balance test lower quarter.
Pre-intervention and post-intervention measurements in both groups
*:
Ankle DFROM before heel-off exhibited a significant time-by-group interaction effect (
A significant time-by-group interaction was found for passive ankle DFROM (F
There was a significant time-by-group interaction for posterior talar glide (
Although no significant time-by-group interaction was observed for gastrocnemius flexibility, a significant main effect for time was found (F
There was no significant time-by-group interaction for all YBT-LQ scores, but significant main effects for time were found for YBT-LQ scores (
In the present study, two types of stretching were performed in subjects with limited ankle DFROM over 6 weeks. The GSTST group had significantly greater increases in maximum DFROM before heel-off, passive ankle DFROM, and posterior talar glide than the GS group. Gastrocnemius flexibility and YBT-LQ scores increased significantly post-intervention versus pre-intervention in both groups; however, these did not differ significantly between groups.
For normal ankle DFROM to occur prior to heel-off, sufficient gastrocnemius flexibility and posterior talar glide must be generated [27]. Posterior talar glide increased significantly only in the GSTST group, which may have contributed to the significant increase in maximum DFROM before heel-off. In addition, talus-stabilizing taping would have provided stability to the talus during GS, which may also explain the increase in the maximum DFROM before heel-off. Since talocrural joint movement is caused by tibia movement relative to the talus or talus movement relative to the tibia, applying a stabilizing force to the talus can further increase tibial advancement for a fixed foot during GS. Our results are consistent with previous research. One study used GS with sustained talocrural joint mobilization to apply a constant anterior-to-posterior stabilizing force to the talus and found a significant increase in posterior talar glide and ankle DFROM before heel-off [13]. Another study found that ankle DFROM before heel-off increased significantly in patients who walked with talus-stabilizing taping, which provided a constant anterior-to-posterior stabilizing force to the talus [15]. Therefore, GSTST is useful for restoring ankle DFROM in the stance phase of gait in subjects with limited DFROM.
We found that gastrocnemius flexibility increased significantly after intervention in both groups, but posterior talar glide increased only in the GSTST group. This may be why the GSTST group had significantly greater passive ankle DFROM than the GS group. These results are consistent with previous studies. Jeon et al. [17] found that using self-stretching with a strap resulted in significantly greater ankle DFROM than performing static stretching in subjects with limited DFROM. Another study compared the immediate effects of gastrocnemius static stretching and GS with sustained talocrural join mobilization in subjects with limited passive ankle DFROM; both groups showed significant improvement in passive ankle DFROM after intervention, but there was no difference between groups [13]. Conversely, we found significant differences between the groups. This may be due to the longer intervention period used in the present study. For example, in another study, plantar flexor static stretching was performed for 6 weeks in subjects with limited ankle DFROM; ankle DFROM showed significant improvement at 4 weeks versus 2 weeks and at 6 weeks versus 4 weeks [19]. Therefore, GSTST is a useful intervention for increasing passive ankle DFROM in subjects with limited DFROM.
Posterior talar glide improved significantly more in the GSTST group than in the GS group, and increased significantly from pre- to post-intervention only in the GSTST group. Mobilization with movement treatment techniques, which are applied to the talus in a posteroinferior direction, can be used to minimize anterior talar displacement [27]. The talus-stabilizing taping used in this study was applied with non-elastic taping and, thus, could be considered a mobilization with movement treatment technique, which may explain the increase in posterior talar glide. Kang et al. [13] reported significantly increased posterior talar glide following GS with application of mobilization with movement to the talus in an anterosuperior-to-posteroinferior direction compared with GS alone. Another study indicated that posteroinferior talar glide mobilization increased posterior talar glide, and weight-bearing mobilization with movement treatment techniques for increasing ankle DFROM were more effective at increasing posterior talar glide than non-weight bearing mobilization with movement treatment techniques [14]. Posterior talar glide may have increased in our study because talus-stabilizing taping was applied in a weight-bearing position.
Post-intervention gastrocnemius flexibility was significantly higher than pre-intervention in both groups, which did not differ significantly. Our findings are consistent with those of previous studies [12, 13]. GSTST is an intervention focused on accessory motion of the ankle to increase ankle DFROM, so it does not seem to have an effect on gastrocnemius flexibility. Thus, GSTST and GS alone seem to have similar effects on muscle flexibility.
In both groups, YBT-LQ scores improved by more than 8% compared to pre-intervention. When performing the YBT-LQ, ankle DFROM on the test side must be generated to achieve maximum leg extension on the non-test side. Previous studies have found that ankle DFROM is the largest predictor of forward stretch during the YBT-LQ and affects reaching distance [8, 9, 10]. We found that ankle DFROM increased compared to pre-intervention in both groups, which appeared to have significantly increased YBT-LQ score. Although the GSTST group showed a significantly higher increase in ankle DFROM than the GS group, there was no significant difference in YBT-LQ score between the two groups. This may be because YBT-LQ performance is affected by factors other than ankle DFROM, such as lower-extremity strength, core stability, and mobility of the hip and knee joints [24]; however, these were not considered in this study.
Although some studies have focused on the immediate effects of various interventions for improving limited ankle DFROM, others have suggested that a long intervention period is required to restore ankle DFROM [18, 19, 20]. In this study, as both interventions were performed for 6 weeks and showed significant increases in all parameters related to ankle DFROM and balance compared with pre-intervention levels, long-term effects were demonstrated for both GSTST and GS. In addition, GSTST was more effective than GS for posterior talar glide, passive DFROM, and maximum DFROM before heel-off. Unlike sports taping used in previous studies [29, 30], the taping method applied in this study could be used during dynamic tasks with ankle movement, and as it is inexpensive and easy to apply, performing GS with talus stability taping has the advantage that it can be applied easily by anyone in clinical practice. Therefore, it is recommended that GSTST is applied for 6 weeks as an intervention to increase ankle DFROM, gastrocnemius flexibility, posterior talar glide, and balance in subjects with limited ankle DFROM.
There are several limitations to this study. After applying GS, only passive ankle DFROM was measured. Future studies should measure ankle DFROM in a weight-bearing position and active ankle DFROM after applying GSTST. In addition, when measuring passive ankle DFROM, the force applied to the plantar surface of the foot was not quantified. Furthermore, during GSTST, the amount of force created by the tape was not measured. Third, this study cannot be generalized to other subjects with ankle injury because subjects with limited ankle DFROM were involved. Future studies should include subjects with ankle or knee pathologies due to limited ankle DFROM. Finally, when measuring the ankle DFROM before heel-off pre- and post-intervention, we did not confirm whether the walking speed was the same.
Conclusions
We investigated changes in variables related to ankle DFROM and balance after applying GSTST and GS for 6 weeks. GSTST resulted in greater increases than GS in ankle DFROM before heel-off, passive ankle DFROM, and posterior talar glide. Therefore, to improve ankle DFROM and balance in clinical practice or sports medicine, we propose GSTST, which can achieve long-term improvements in both gastrocnemius flexibility and posterior talar glide.
Author contributions
CONCEPTION: Soo-Yong Kim, Jong-Chul Jung and Yong-Il Shin.
PERFORMANCE OF WORK: Da-In An, Won-Young Park, Jong-Chul Jung and Soo-Yong Kim.
INTERPRETATION OR ANALYSIS OF DATA: Soo-Yong Kim and Yong-Il Shin.
PREPARATION OF THE MANUSCRIPT: Soo-Yong Kim, Yong-Il Shin, Jong-Chul Jung, Da-In An and Won-Young Park.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Soo-Yong Kim and Jong-Chul Jung.
SUPERVISION: Soo-Yong Kim and Yong-Il Shin.
Ethical considerations
Ethical approval was given by the Institutional Review Board of Pusan National University Yangsan Hospital (05-2020-085; date of approval: May 14, 2020) and all participants signed an informed consent form.
Funding
This study was supported by Research institute for Convergence of biomedical science and technology (30-2020-010), Pusan National University Yangsan Hospital.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.