
Abstract
BACKGROUND:
The underlying morphology and behavior of abdominal muscles during breathing are still lacking in knowledge in healthy population.
OBJECTIVE:
To analyze the effects of three different types of breathing on the architectural characteristics of abdominal muscles.
METHODS:
Ninety-eight healthy subjects were measured to assess the effects of breathing on the abdominal muscles, subjects performed three different types of breathing and the muscular thickness was measured with ultrasound imaging, analyzing also the differences between sexes.
RESULTS:
During the three different types of breathing and in comparison with the resting state, an increase of the thickness has been reported in the transversus abdominis (
CONCLUSIONS:
All breathings activated the deepest abdominal muscles, but the most superficial were only activated with lips pursed. Moreover, men appeared to activate more the deepest abdominal muscles but also the rectus abdominis. Findings in this study support the use of different types of breathing depending on the muscle to be activated or the sex, helping health care professionals to address their interventions on the abdominal muscles with a more focused approach.
Introduction
In recent years, ultrasound imaging has become popular in physical therapy, since it is a portable, no-radiation method that provides high-resolution images of neuromuscular structures [1, 2]. Moreover, ultrasound imaging has been demonstrated to be a valid and reliable method to assess the muscle’s architectural characteristics [3], specifically in muscular thickness (MT). MT is one of the most studied variables, since it could be an indicator of a muscle’s functional capacity [4, 5, 6].
In this regard, previous research on MT has shown that it is a reliable measurement in order to know the size of a muscle [7, 8], but its relationship with the muscle contraction and activation still lacks evidence [9, 10, 11]. Some studies analyzed MT in different muscles in the lower limb [12], low back 8̧ and abdominal area [2, 8]. Particularly, the abdominal wall has been largely investigated, as it influences the pelvis and low back stability, and it is involved in breathing, especially during exhalation [16, 17]. Nevertheless, there is little evidence on changes in architectural parameters of the abdominal wall during breathing, since its unique morphology, with different types of fibers with different orientations, increases the difficulty in measuring contraction and activation [2, 4].
Prior systematic reviews have pointed out the need for further research in order to increase the knowledge about the underlying morphology and behavior of abdominal muscles [2], highlighting the relevance of ultrasound imaging in physical therapy during clinical practice, diagnosis and investigation [11, 18].
Taking into consideration that breathing influences abdominal muscles, specifically during exhalation [19], the purpose of this study was to analyze the effects of three different types of breathing on the architectural characteristics of abdominal muscles, which was assessed by ultrasound imaging.
Methods
Study design
A transversal observational study was conducted in accordance with the principles of the Declaration of Helsinki. This investigation was approved by the Ethics Committee of the University of Vigo (Spain) with the number 20072018/44 on July 17, 2018. Subjects were informed about all the procedures and provided with a written informed consent before the intervention. The rights of all subjects were protected.
Participants
In order to estimate the adequate number of participants for considering the results consistent, the sample size was calculated with the software G*Power (version 3.1) and based on the study run by Amerijckx et al. [16], where similar interventions and measurements were performed. The variables selected were ‘transversus abdominis thickness (average) at the end of relaxed expiration’ versus ‘transversus abdominis thickness (average) at the end of full expiration’, with a power of 0.95, and an
Finally, 98 healthy subjects (64% women, 36% men; age 22.43
Procedures
In this study, ultrasonography examination was performed with a 5–10 Mz lineal ultrasounds transducer (SonoSite M-Turbo
Participants were placed in supine position, having their knees and hips bent and their feet supported. Their skin was covered with a conductive gel and abdominal muscles were measured in the subjects’ dominant side. For RA, the probe was placed in the anterior abdominal area, just lateral to the navel, and for TrA, IO and OE, the probe was moved in the medial-lateral direction, between the rib cage and the iliac crest, until the muscle-fascia junction of the three muscles could be identified [20]. MT measurements were performed at rest and during the three different types of breathing by using the on-screen Calipper set between the fascial borders of the muscle [2, 7].
MT at rest and during different types of breathing in abdominal muscles (mean
SD)
MT at rest and during different types of breathing in abdominal muscles (mean
BME: breathing with maximal exhalation; BOG: breathing with open glottis: BPL: breathing with pursed lips; EO: external oblique; IO: internal oblique; RA: rectus abdominis; TrA: transversus abdominis; MT: muscular thickness; SD: standard deviation.
Subjects participating in this study were trained in three different types of breathing before the intervention: BME, BOG and BPL. All breathings started with a maximal nasal inspiration followed by a maximal mouth exhalation. In BME, subjects only performed the maximal exhalation; in BOG, the exhalation was performed having the glottis opened; and in BPL, lips were pursed [16, 17]. The intervention consisted in locating the abdominal muscles with ultrasound imaging and then performing the different breathings. MT was measured at the end of the exhalation, freezing the screen and using the on-screen Calipper. In order to preserve measurement reliability, the first rectus abdominis was measured during the three different types of breathing, and then the probe was placed laterally and obliques and transversus abdominis were found in the same image and measured under the three different conditions [20].
Statistical analysis
All statistical analyses were carried out by SPSS for Macintosh (version 25.0, Chicago, IL, USA). In order to compare MT at rest and during the different breathings, a repeated-measurement analysis of variance was performed, with the intra-subject factor type of breathing. Moreover, in order to analyse the differences between women and men, the intra-subject factor sex was included. Partial eta-squared (
Results
Ninety-eight healthy subjects were measured for this study, and their MT in abdominal muscles was evaluated by ultrasound imaging at rest and during different types of breathing. Results of the comparison between MT at rest and during the three different breathings are detailed in Table 1.
As shown in Table 1, a significant MT increase was found in TrA (
Flow chart outlining the intervention and measurement process.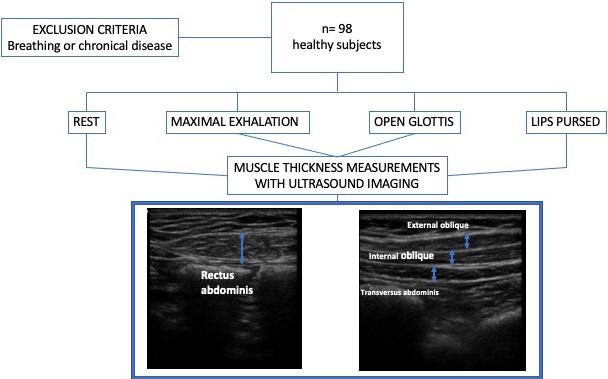
Rainclouds plot of muscular thickness (MT) in the TrA (transversus abdominis), IO (internal oblique), EO (external oblique) and RA (rectus abdominis) according to sex. BME: breathing with maximal exhalation; BOG: breathing with open glottis; BPL: breathing with lips pursed.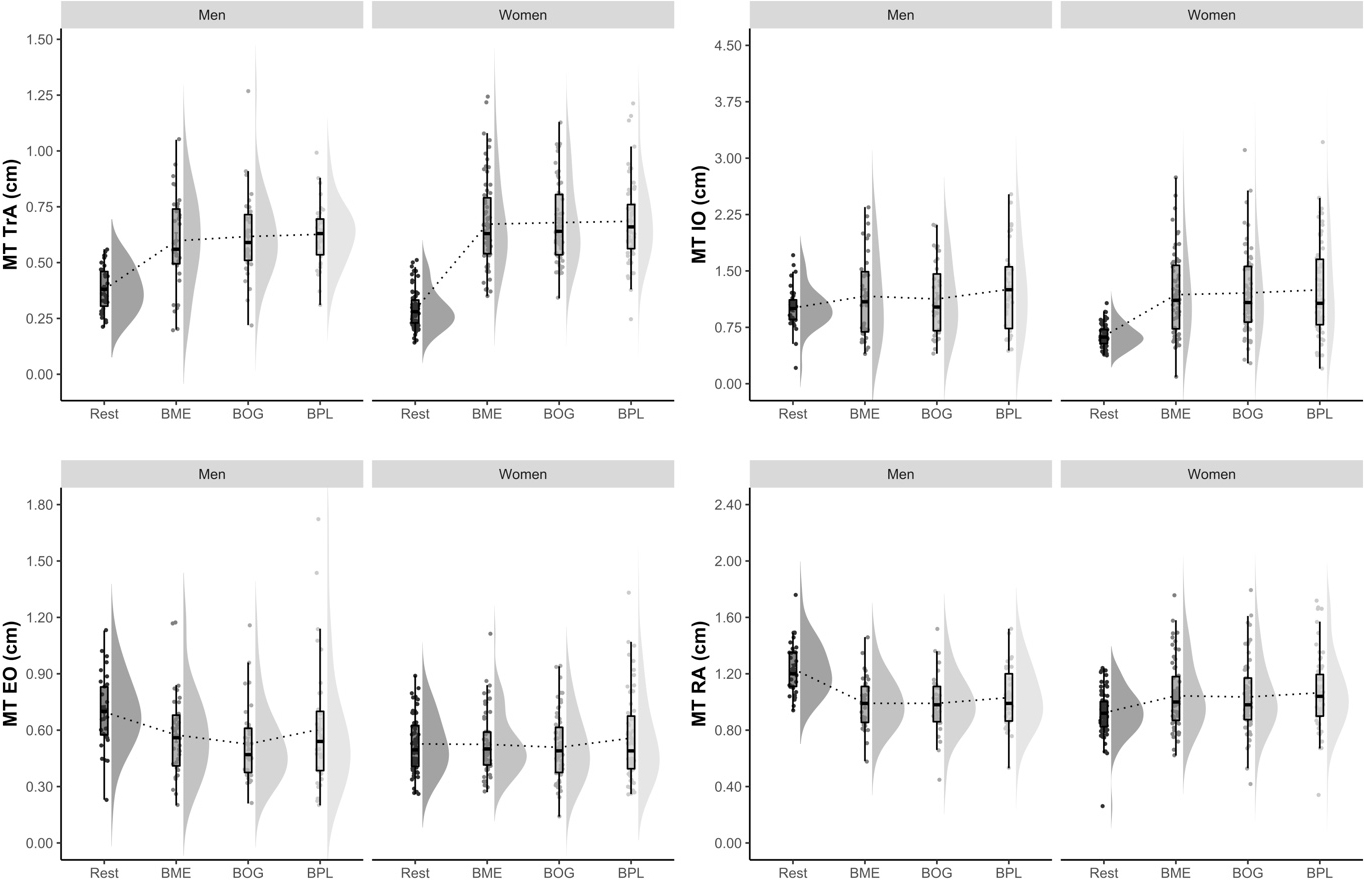
The analysis of the results according to sex is shown in Fig. 2. In TrA, both women and men had a significant increase in the thickness with the three types of breathing in comparison with rest, but men had a significantly higher increase than women in all breathings (
For this study, MT in abdominal muscles was evaluated in 98 healthy subjects at rest and during three different types of breathing (BME, BOG and BPL) using ultrasound imaging. The main results obtained were: (1) TrA and IO increase their MT during the three types of breathing in comparison with the resting phase: (2) IO increases its MT significantly during BPL in comparison with BME; (3) EO increases its MT significantly in BPL in comparison with BOG and decreases significantly in BOG in comparison with the resting phase; and (4) RA increases its MT significantly during BPL in comparison with BME and BOG. Moreover, sex differences were found in TrA, IO and RA.
Previous studies reported similar results, showing that the most internal muscles (TrA and IO) changed their MT significantly with maximal breathing in comparison with the resting phase, but RA and EO did not seem to change [9, 16]. Furthermore, TrA appeared to be the most active muscle during breathing [23] and also when performing different exercises [14, 24] and in different positions [25, 26], which is consistent with the findings included in this study, since TrA has larger ES than IO. Ultrasound imaging has proved to be a reliable method to assess MT on the abdominal wall [2]. However, most findings previously reported were measured by electromyography and should be read carefully, since little correlation has been found between electromyography and ultrasound imaging in the abdominal wall [9]. In this line, MT in this area does not only change due to the muscle itself, but also to the forces generated by the other abdominal muscles [4]. In addition, electromyography measures the surface of the abdominal wall, but does not report information on the deepest muscles that are involved in the breathing process [27].
On the other hand, differences during the three types of breathing have been reported depending on the muscle measured. Specifically, BPL changes the MT of IO, EO and RA in comparison with BME, BOG or both. Prior investigations showed that pursing the lips during exhalation meant a greater activation of the abdominal muscles, but especially the superficial ones, which change the recruitment pattern of the abdominal wall [28]. However, the use of this type of breathing is controversial, since it has been demonstrated to increase intraabdominal pressure, due to an increase of the air resistance [29]. The effects of a high abdominal pressure on the spine or on the pelvic floor have been studied, and currently, exercises that decrease intraabdominal pressure are preferred in order to improve spine and pelvic stability without damaging other structures [14, 30]. However, the activation of the deep abdominal muscles during this exercise is still being discussed.
During breathing, all abdominal muscles are involved in different ways, but EO is the only one that decreases its MT significantly during BOG in comparison with the resting phase. Regarding previous research on the anatomy and biomechanics of the abdominal wall, the complex fascial system of this area produces a coactivation of all the abdominal muscles during an abdominal contraction, but also a stretching of the structures that can cause a MT decrease [2, 4, 31]. Nevertheless, despite all the muscles are proved to be involved in the breathing process because of their fascial connections, there seems to be a clear implication of TrA and IO during maximal exhalations [10, 17]. In this sense, another factor that may influence these results and others in previous research is the subject’s position during breathing, since it has been shown that a standing position increases the pre-activation of the abdominal muscles, but the abdominal wall is relaxed in supine position [8, 15]. In this study, all the measurements were carried out in supine position in order to control the pre-activation of the abdominal muscles and only analyze the influence of the breathing process. However, the effects of breathing in standing position may be different.
Analyzing these results according to sex, it has been shown that in TrA and IO men had a higher increase than women in the muscle thickness during the three types of breathing in comparison with rest. This finding agree with Manshadi et al. [32] who also measured abdominal thickness in both sexes with ultrasound imaging, but during an abdominal exercise, and reported that men had significantly greater activations than women in all abdominal muscles. Conversely, the behavior of the RA is different from that of the other muscles of the abdominal wall, since during the breathing test women decrease the thickness of this muscle but men increase it. These differences could be explained due to the unequal anatomy between men and women, since the abdominal wall is similar but the viscera, the pelvic floor muscles and the fascial relationships are quite different and could produce differences in contraction and activation [33]. Nevertheless, little evidence has been found about the effects of breathing on the abdominal muscles and the differences between women and men, so further research should consider these results and analyze other possible explanations for this differences.
This study aims at contributing to the scientific debate about the behavior of abdominal muscles and especially during the breathing process, with implications in exercise, sports and the clinical respiratory practice of health professionals. However, several limitations must be discussed, since the sample conformed by healthy subjects does not allow to extrapolate results to other unhealthy populations, particularly those with spine or pelvic floor problems. In addition, all participants were measured in supine position, but the behavior of abdominal muscles may be different in other positions or during movements, so other situations like sport practice should be analyzed in future research in order to determine whether the MT of abdominal muscles depends on the position.
Conclusion
In conclusion, the deepest abdominal muscles, TrA and IO, increase their MT during the three different types of breathing in comparison with the resting phase, and EO and RA do not appear to be influenced by the type of breathing, finding activation only with the BPL.
Findings within this study support the use of different types of breathing depending on the muscle to be activated, thus helping healthcare professionals to address their interventions on the abdominal muscles with a more focused approach.
Author contributions
CONCEPTION: Iria Da Cuña-Carrera and Mercedes Soto-González.
PERFORMANCE OF WORK: Iria Da Cuña-Carrera, Mercedes Soto-González, Alejandra Alonso-Calvete and Yoana González-González.
INTERPRETATION OR ANALYSIS OF DATA: Alejandra Alonso-Calvete and Iria Da Cuña-Carrera.
PREPARATION OF THE MANUSCRIPT: Yoana González- González and Mercedes Soto-González.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Iria Da Cuña-Carrera, Mercedes Soto-González, Alejandra Alonso-Calvete and Yoana González-González.
SUPERVISION: Iria Da Cuña-Carrera, Mercedes Soto-González, Alejandra Alonso-Calvete and Yoana González-González.
Ethical considerations
Subjects were informed about the procedures and signed a written informed consent before the intervention. This study was approved by the Ethics Committee of the University of Vigo (Spain) with the number 20072018/44 on July 17, 2018 and followed the principles of the Declaration of Helsinki.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.