
Abstract
Background:
The extent to which differences in throwing kinematics between pitchers and nonpitchers influence ulnar collateral ligament (UCL) thickness has yet to be explored.
Purpose:
To examine bilateral UCL thickness in collegiate baseball players and potential contributions of throwing mechanics to the throwing arm’s UCL over the course of a preseason.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 22 Division I collegiate baseball players (pitchers: n = 11; nonpitchers: n = 11) from one university participated in this investigation. Ultrasound was used to measure UCL thickness in both the throwing and nonthrowing arms. Players wore a throwing sensor during all throwing activities that recorded elbow varus torque, arm speed, shoulder rotation, and arm slot. A 2-way analysis of variance (position [pitcher vs nonpitcher] × arm [throwing vs nonthrowing]) was conducted to investigate UCL thickness. Independent-samples t tests were used to compare throws between pitchers and nonpitchers. Pearson correlation coefficients were used to analyze relationships between UCL thickness and throwing variables.
Results:
UCL thickness was significantly greater in the throwing arm versus nonthrowing arm (0.618 ± 0.038 vs 0.581 ± 0.047 mm, respectively; P ≤ .001) and was significantly greater in pitchers than nonpitchers (0.618 ± 0.039 vs 0.581 ± 0.045 mm, respectively; P = .03). A significantly greater throw count (P = .02), high-effort throw count (P ≤ .001), torque (P ≤ .001), and high-effort torque (P ≤ .001) were observed in pitchers. UCL thickness was significantly related to high-effort throws (r = 0.43), torque (r = 0.42), high-effort torque (r = 0.48), and arm speed (r = 0.46).
Conclusion:
The findings emphasize the unique biomechanical demands on pitchers, highlighting the necessity for targeted injury monitoring strategies in baseball, particularly focusing on high-effort pitches.
Injuries to the medial ulnar collateral ligament (UCL) in the elbow are becoming more common at all levels of baseball and are considered among the most common pitching-related injuries, often requiring a surgical intervention.15,16 The incidence of UCL reconstruction, also known as Tommy John surgery, has been reported to be highest between the ages of 15 and 24 years, and this rate is expected to increase through 2025. 28 In a 3-year study on collegiate baseball players from 2016 to 2019, just under half of the Division I programs had at least 1 player requiring UCL reconstruction. 36 With over 38,000 collegiate baseball players in the United States annually, 31 prevention and the early identification of the underlying mechanisms for a UCL injury are important to reduce these injury rates.
It is believed that repetitive high loads exerted through the elbow during throwing, especially during pitching, cause microdamage to the UCL.17,43 The cumulative effects of high-intensity repetitive loading may lead to stretching of the ligament, which can then result in the development of joint instability, an increased risk of UCL injuries,26,33 and adaptations leading to failure of the UCL.7,37,41 A formal diagnosis of a UCL injury usually involves imaging techniques that include radiography, stress radiography, and magnetic resonance imaging. However, the use of ultrasonography has gained popularity because it is a quick and noninvasive tool that can show adaptive changes to the UCL. A 10-year prospective study on elite pitchers reported that the throwing arm’s UCL was thicker, more likely to have calcifications, and caused increased joint laxity. 9 Although investigators for that study were unable to relate these changes to injuries, a study conducted by Shanley et al 38 reported a positive relationship between stress ultrasound, UCL morphology, and an increased UCL injury risk in 70 professional baseball pitchers during spring training. Research has shown that ultrasound imaging may have the ability to detect changes in the UCL before the onset of symptoms in professional pitchers.2,9 Interestingly enough, investigations examining UCL thickness and injuries in nonpitchers are scarce, even though nonpitchers perform similar sport-specific tasks and are exposed to the same injury mechanisms as pitchers.
Wearable throwing sensors are often used to assess elbow varus torque, among other variables,3,6,24,48 as the sensors provide a reliable alternative to motion capture. The UCL injury risk has also been correlated with factors such as ball velocity,5,8,29,40,42 volume of throws,21,44 pitch type, 21 fatigue, 19 shoulder strength profiles,4,39 changes in shoulder range of motion,18,45,46 and poor throwing mechanics.1,10,17
While these risk factors have been extensively reported for baseball pitchers within the current literature, comparisons across positions are lacking. This is not unusual, as pitchers predominantly have the most UCL injuries, around 88% of reported UCL reconstruction cases. 12 At the collegiate level, 134 surgical procedures were reported during the 2017 National Collegiate Athletic Association baseball season, with 85.8% (n = 115) occurring in pitchers and 14.2% (n = 19) occurring in nonpitchers. 35 Injury data from 1988 to 2004 showed that the act of throwing accounted for 15% of all game injuries and that 71% of elbow injuries were from throwing at the collegiate level. 13 On account of the seemingly preferential injury risk, it bears investigating the kinetic and kinematic differences between these 2 groups.
Although recent research has reported evidence of a relationship between inefficient throwing biomechanics and an increased injury risk, a thorough investigation is needed to identify differences in throwing biomechanics and kinetics between players and how they might contribute to an increased UCL injury risk. Therefore, the purpose of this study was to compare bilateral differences in UCL thickness in the throwing and nonthrowing arms between pitchers and nonpitchers as well as correlate known factors associated with a UCL injury with throwing mechanics (ie, elbow varus torque, arm speed, shoulder rotation, and arm slot). Because of the increased number of throws demanded from pitchers compared with other positions, we hypothesized that UCL thickness and elbow varus torque would be greater in the pitcher group than the nonpitcher group.
Methods
A total of 22 collegiate baseball players underwent this investigation during preseason training. To meet inclusion criteria, players must have had no history of injuries in the throwing arm and must be without current symptoms in their throwing arm. Players were grouped based on their primary position: pitchers (n = 11) and nonpitchers (n = 11) (Table 1). Study approval and implementation were in accordance with recommendations of the university’s institutional review board for the protection of human participants (ED-18-178).
Participant Characteristics a

Data are presented as mean ± SD. Bolded P values indicate a statistically signficant difference between groups (P < .05). The nonthrowing arm was assessed to establish that throwing arm differences in groups were the result of throwing and not anthropometric discrepancies between groups. UCL, ulnar collateral ligament.
Before testing, participants provided informed consent and completed the Physical Activity Readiness Questionnaire for screening of any current or previous injuries, specifically, injuries of the UCL or those that may hinder testing and evaluation in the current investigation. No players had a history of injuries within the last 12 months that required >2 weeks of missed participation. Additionally, players who had undergone UCL reconstruction were excluded.
Ultrasonography
During their visit to the laboratory, players laid supine with their arm resting on a plinth, and a goniometer was used to ensure the shoulder was abducted at 90°, with elbow flexion of 30° and the forearm in a supinated position. B-mode ultrasonography (LOGIQ; GE Healthcare) was used to capture an image of the anterior band of the UCL. To maintain consistency, all images were taken by the same researcher (M.J.L.). To determine UCL thickness, the midpoint of the anterior band 2 was measured (in mm) 32 using ImageJ (National Institutes of Health) (Figure 1). The averages of 3 measurements from both arms (throwing and nonthrowing) were used for analyses. All measurements were performed by the same researcher to maintain consistency (Q.R.J.). Although stress ultrasonography is commonly used within UCL literature, for the purposes of this investigation, imaging in a resting state was conducted for anthropometric comparisons.
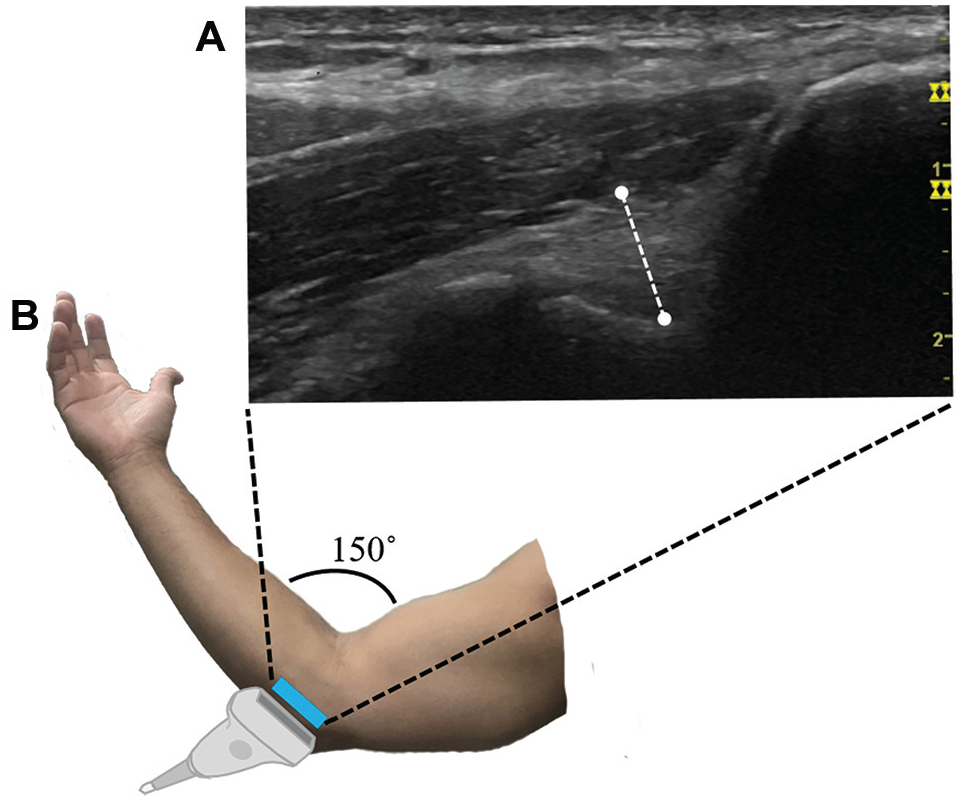
Examples of (A) ultrasound and (B) arm position. Dotted line denotes the midpoint measurement of ulnar collateral ligament (UCL) thickness.
Throwing Sensor
Before the first throwing session, each player was given a sensor and sleeve (Motus Global). Players were then instructed on how to properly wear the sensor: with the target printed on the sleeve aligned with the medial epicondyle of the humerus and the sensor 5 cm below, resting on the lateral aspect of the ulna. 6 The sensor was worn every day during all throwing events during the preseason (eg, practices, bullpens, warm-ups, exhibitions) for a total of 60 days. With each throw, the sensor recorded and stored the following variables of interest: arm speed (in rpm), arm slot (in deg), shoulder rotation (in deg), and elbow varus torque (in Nm). After throwing activities were concluded for the day, data from the sensors were transferred and stored on a secure server. Previous research has shown the system to be a valid and reliable measurement tool, deemed excellent by internal and third-party peer-reviewed studies.3,6
All recorded throws were included in the throw count with a subgroup of high-effort throws. High-effort throws were defined as any throw >70% of the player’s average of the 5 highest torque throws from the past 2 weeks. The high-effort throw threshold was a rolling average and changed daily as players built up their throwing loads throughout the preseason. Additionally, to meet inclusion criteria, players must have had at least 1000 throws recorded.
Statistical Analysis
A 2-way mixed-factorial analysis of variance (position [pitcher vs nonpitcher] × arm [throwing vs nonthrowing]) was performed to analyze UCL thickness. Independent-samples t tests were used to compare variables between pitchers and nonpitchers collected from the throwing sensor: arm speed, arm slot, shoulder rotation, and elbow varus torque. Data were reported as mean ± standard deviation for all throws between pitchers and nonpitchers. Pearson correlation coefficients were used to analyze relationships between UCL thickness and throwing variables. Pearson correlation coefficients were interpreted per the recommendation of Cohen 11 as weak (0.10), moderate (0.30), or strong (0.50). The a priori alpha level was set at .05, and all analyses were conducted using SPSS Statistics (Version 23; IBM).
Results
There was no difference in weight between the 2 groups (P = .111), but the pitchers were significantly taller than the nonpitchers (P = .046). Additionally, no anthropometric differences were found between the groups in the nonthrowing arm (Table 1).
For UCL thickness, no position × arm interaction (P = .74) was observed; however, there was a significant main effect for position (P = .03; partial η2 = 0.20) and throwing arm (P ≤ .001; partial η2 = 0.25) (Figure 2). When collapsed by position, UCL thickness was significantly greater in the throwing arm compared with the nonthrowing arm (0.618 ± 0.038 vs 0.581 ± 0.047 mm, respectively). Additionally, when collapsed by arm, pitchers had a significantly greater UCL thickness compared with nonpitchers (0.618 ± 0.039 vs 0.581 ± 0.045 mm, respectively).

Main effects on (A) arm and (B) position for ulnar collateral ligament (UCL) thickness.
Comparisons for throwing variables from the sensor between pitchers and nonpitchers are shown in Table 2. There were no significant differences observed between groups for arm slot (P = .09), high-effort arm slot (P = .78), or high-effort shoulder rotation (P = .10). However, pitchers displayed significantly greater values for throw count (P = .02), high-effort throw count (P ≤ .001), torque (P ≤ .001), and high-effort torque (P ≤ .001).
Measurements From Wearable Sensor a
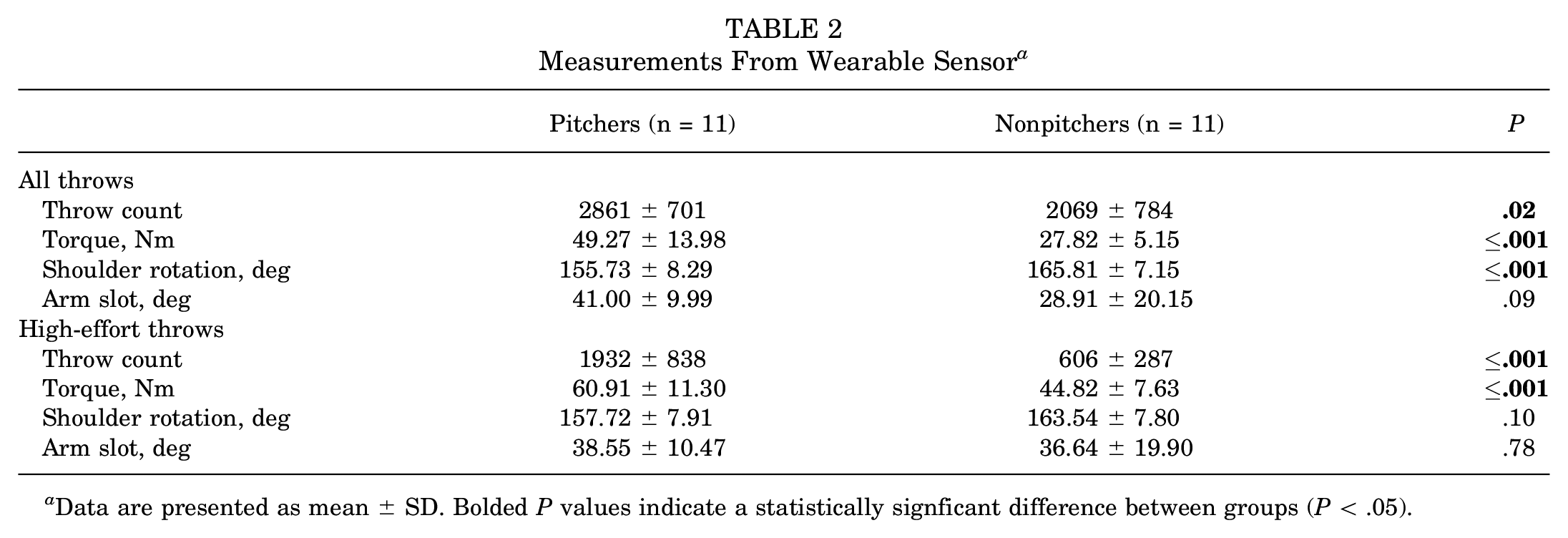
Data are presented as mean ± SD. Bolded P values indicate a statistically signficant difference between groups (P < .05).
Figure 3 displays the significant relationships between UCL thickness and throwing variables. Of note, UCL thickness was moderately related to high-effort throws (r = 0.43; P = .44), torque (r = 0.42; P = .05), high-effort torque (r = 0.48; P = .025), and arm speed (r = 0.46; P = .033). However, UCL thickness was not related to all throws (r = 0.28; P = .20), high-effort arm speed (r = 0.25; P = .20), shoulder rotation (r = −0.18; P = .43), high-effort shoulder rotation (r = −0.02; P = .93), arm slot (r = 0.01; P = .97), or high-effort arm slot (r = −0.25; P = .27).

Correlations between high-effort (HE) throw count, varus torque during all throws, HE varus torque, and arm speed during all throws and ulnar collateral ligament (UCL) thickness of the throwing arm (TA).
Discussion
The purpose of this investigation was to compare bilateral UCL thickness and known factors associated with a UCL injury between pitchers and nonpitchers. Our hypotheses were supported, as pitchers had a significantly larger UCL thickness than nonpitchers (P = .03), and UCL thickness of the throwing arm was significantly larger than that of the nonthrowing arm (P ≤ .001). Additionally, UCL thickness was associated with high-effort throws (r = 0.43; P = .44), varus torque (r = 0.42; P = .05), high-effort varus torque (r = 0.48; P = .025), and arm speed (r = 0.46; P = .033), with pitchers exhibiting significantly higher values for all of these variables except for arm speed.
We examined bilateral differences in UCL thickness and the relationship between UCL thickness and throwing variables in collegiate baseball players. Consistent with previous research,9,25,27,30,47 UCL thickness was greater in the throwing arm. The throwing arm experiences considerably more loading than the nonthrowing arm during a player’s career, resulting in a thicker UCL band compared with the nonthrowing arm. Additionally, UCL thickness was greater among pitchers than nonpitchers. In our investigation, pitchers had a significantly greater throw count, high-effort throw count, torque, and high-effort torque, which highlights the positional demands of pitchers; nonpitchers are often required to make shorter throws, lower intensity throws, and fewer high-effort throws compared with pitchers, which may result in a smaller UCL hypertrophic adaptation.
The thickness of the UCL demonstrated associations with high-effort throws, elbow varus torque, high-effort elbow varus torque, and arm speed. These relationships further underscore the observed disparities in positions, with pitchers exhibiting notably more high-effort throws, elbow varus torque, and high-effort elbow varus torque. Pitchers had significantly higher values for the majority of the variables correlated with UCL thickness, which may explain the significantly higher UCL reconstruction rates for pitchers. Since 2020, 503 professional players have required UCL reconstruction, with 94% of them being pitchers. 34 The significantly higher prevalence of UCL injuries among pitchers, along with their thicker UCLs, underscores the unique biomechanical demands placed on pitchers and highlights the need for targeted injury monitoring strategies in baseball.
There was no significant relationship between UCL thickness and total throw count. In regard to pitchers, this could imply that the total number of throws (ie, pitch count) may not accurately reflect UCL adaptations. Instead, it highlights the importance of high-effort pitches as the pivotal factor in determining pitch count guidelines. This is consistent with previous literature,29,40 which has linked increased pitch velocity with increased elbow varus torque. Our findings underscore the crucial role of high-effort pitches over total throw count in understanding UCL adaptations, aligning with previous research that emphasizes the link between increased pitch velocity and heightened injury susceptibility.
Our research revealed no correlation between either arm slot or high-effort arm slot and UCL thickness, contrary to previous findings. 22 Unlike Khalil et al, 22 who required participants to complete only 5 high-effort throws, players in the current investigation had to complete at least 1000 throws, for a total of 54,230 throws across participants (51% of these being high-effort), to be eligible for analysis. These differences in data collection methods may account for the variability in results. Additionally, no correlation with either shoulder rotation or high-effort shoulder rotation was found. While our study analyzed shoulder rotation before ball release, previous studies have linked UCL injuries to glenohumeral internal rotation deficits. Glenohumeral internal rotation deficits are believed to increase the UCL injury risk, as they are thought to disrupt the dispersion of loads through the kinetic chain14,23; however, this is not unanimous across the literature.18,20 While this falls outside of the scope of our study, it is worth mentioning, as deficits in total range of motion (internal + external) have been linked to UCL injuries. 18
Limitations
Careful consideration should be given to the limitations of this study. Muscle strength, range of motion, and full-body biomechanical factors were not extensively explored. Furthermore, the current investigation is limited in establishing causal relationships between the variables. Our study utilized a wearable device as opposed to a motion capture system; however, the system has been proven to be valid and reliable. While we found differences in collegiate baseball players, these findings might not translate to other levels of play.
Conclusion
This study sheds light on the bilateral differences in UCL thickness among collegiate baseball players and underscores the intricate relationship between UCL adaptations and throwing variables. These findings emphasize the unique biomechanical demands on pitchers, highlighting the necessity for targeted injury monitoring strategies in baseball, particularly focusing on high-effort pitches. While our research did not find correlations between arm slot or shoulder rotation and UCL thickness, it emphasized the need to consider broader biomechanical factors for a more comprehensive understanding of elbow injuries in baseball players. The relationship between positional demands, throwing variables, and UCL thickness is multifaceted. Further research is necessary to fully understand the mechanisms underlying their effect on overall UCL health.
Footnotes
Final revision submitted October 21, 2024; accepted November 14, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Oklahoma State University (ED-18-178).