Low-load resistance training with blood flow restriction (LL BFR) attenuated delayed onset muscle soreness (DOMS) under some conditions.
OBJECTIVE:
The purpose of this study examined the effects of reciprocal concentric-only elbow flexion-extension muscle actions at 30% of peak torque on indices of DOMS.
METHODS:
Thirty untrained women (mean SD; 22 2.4 years) were randomly assigned to 6 training days of LL BFR ( 10), low-load non-BFR (LL) ( 10), or control ( 10). Participants completed 4 sets (1 30, 3 15) of submaximal (30% of peak torque), unilateral, isokinetic (120s) muscle actions. Indices of DOMS including peak power, resting elbow joint angle (ROM), perceived muscle soreness (VAS), and pain pressure threshold (PPT) were assessed.
RESULTS:
There were no changes in peak power, ROM, or VAS. There was a significant interaction for PPT. Follow-up analyses indicated PPT increased for the LL BFR condition (Day 5 Day 2), but did not decrease below baseline. The results of the present study indicated LL BFR and LL did not induce DOMS for the elbow extensors in previously untrained women.
CONCLUSION:
These findings suggested LL BFR and LL concentric-only resistance training could be an effective training modality to elicit muscular adaptation without inducing DOMS.
Resistance training is a potent stimulator of muscle function that induces neuromuscular adaptations, muscular hypertrophy, and increases muscle strength [1]. Traditionally, resistance training is prescribed with moderate to heavy training loads (50–100% 1 repetition maximum [1RM]) to elicit muscular adaptations via mechanotransduction [2]. The use of heavy training loads (HL), however, is not always feasible and may have limited application during rehabilitation, among older adults, or among symptomatic populations. Alternately, resistance training with low training loads (20–40% 1RM), with and without blood flow restriction (BFR), has demonstrated comparable increases in muscle size as HL, but smaller or similar increases in muscle strength [3, 4, 5, 6]. The adaptations associated with low-load BFR (LL BFR) and low-load non-BFR resistance training (LL) may to be achieved through greater metabolic stress from accumulation of metabolites, reactive oxygen species, hyperemia, and/or hormonal changes [1].
Unaccustomed exercise can result in delayed onset muscle soreness (DOMS). Specifically, high-contractile forces, particularly during the eccentric phase of a muscle action, are associated with z-line streaming and connective tissue damage [7]. DOMS, however, was also observed following LL BFR and LL resistance training. For example, four sets of unilateral isotonic reciprocal (concentric-eccentric) elbow flexion muscle actions performed to failure at 40% 1RM with and without BFR increased perceived muscle soreness 24- and 48-h post-exercise [8]. Furthermore, four sets of unilateral isotonic reciprocal (concentric-eccentric) knee extension muscle actions performed to failure at 20% 1RM with BFR increased blood creatine kinase (CK) and myoglobin levels that remained elevated five days post-exercise [9].
These findings [8, 9] however, were not consistent with other investigations [10, 11, 12] that reported little or no DOMS after eccentric- or concentric-only resistance training. For example, after 75 unilateral isokinetic concentric-only or eccentric-only elbow flexion muscle actions (1 30, 3 15) at 30% 1RM with BFR, there were no changes in maximal voluntary isometric contraction (MVIC), perceived muscle soreness, resting joint angle (ROM), pain pressure threshold (PPT), or muscle edema [11]. In addition, after 75 unilateral isotonic concentric-only or eccentric-only elbow flexion muscle actions at 30% 1RM with BFR, there were no changes in MVIC, muscle thickness, circumference, or ROM [12]. However, for the eccentric-only condition perceived muscle soreness increased 24 and 48-h after the initial bout of exercise. Thus, contradictory evidence exists on the application of BFR and low-load training protocols that utilized various modes (isotonic vs isokinetic), muscle actions (concentric-eccentric, eccentric-only, concentric-only) muscle groups (knee extensors and elbow flexors), and sexes (men and women). Specifically, females are an understudied population in the resistance training literature, particularly among BFR investigations [13] and there is less available information on the effect BFR has on the upper body. Furthermore, no previous investigations examined BFR during reciprocal concentric-concentric muscle actions of the elbow flexors and extensors. There is a lack of available evidence on the effect of LL BFR versus LL of the upper body on indices of DOMS among previously untrained women that may limit the application of BFR in the athletic, inactive, and clinical populations. Therefore, the purpose of the present study was to examine the effects of reciprocal concentric elbow flexion-extension muscle actions at 30% of peak torque with and without BFR on indices of DOMS in previously untrained women. Based on previous investigations [11, 12] we hypothesized LL BFR and LL resistance training would not be associated with DOMS.
Methods
Participants
Thirty female participants volunteered for this study and were randomly assigned to LL BFR ( 10, mean age SD 22 2 years; body mass 60.1 5.3 kg; height 165.1 7.4 cm), LL ( 10, mean age SD 21 1 years; body mass 60.6 4.2 kg; height 163.8 5.5 cm), or control ( 10, mean age SD 23 3 years, body mass 70.1 17.6 kg; height 164.8 9.2 cm). Sample size calculation was performed with G*Power [14]. Sample size was computed from previous investigations that examined direct indices of DOMS [9, 15] with power set at 0.8 and an alpha of 0.05. The computed sample size ranged from 12 to 14 and was consistent with previous investigations [10, 11, 12] that examined LL BFR and LL on indirect indices of DOMS with sample sizes of 9 to 25. Data from these participants were examined in a previous investigation for purposes unrelated to the present study [11]. All participants were recreationally active but had not actively engaged in resistance training for the past six months. Participants had no known cardiovascular, pulmonary, metabolic, muscular, and/or coronary heart disease. Potential participants who took supplements or engaged in caloric restriction were excluded from the study. For the duration of the study, participants were asked to maintain their current diet, sleep, and exercise habits. The study was approved by the University of Nebraska Institutional Review Board for Human Subjects and all participants completed a health history questionnaire and signed written informed consent prior to training (20170517195EP, 05/12/2017).
Experimental design
A randomized, between-group, parallel, repeated measures for time design was used for this study. Thirty women were randomly assigned to LL BFR, LL, or control. BFR was applied using a KAATSU resistance band (KAATSU Master, Sato Sports Plaza, Tokyo, Japan). Participants visited the laboratory on eight occasions: one familiarization day, one baseline day, and six training days. All procedures occurred at the same time of day ( 2 h). BFR was applied at 40% of the lowest amount of pressure needed to completely occlude brachial artery blood flow as indicated by ultrasound. Participants completed reciprocal concentric elbow flexion-extension resistance training with their dominant arm at 30% of elbow flexion and elbow extension peak torque, respectively. Torque thresholds were displayed on a computer screen and monitored in real-time. Participants received both visual and verbal feedback for each repetition. Training was performed three times per week, with 48-h between each training day. Each training day consisted of 75 reciprocal elbow flexion-extension isokinetic muscle actions performed over four sets (1 30, 3 15) separated by 30 s. Muscle actions were performed at a constant angular velocity of 120s using an isokinetic dynamometer (Biodex System 3, Biodex Medical Systems, Inc. Shirley, USA). During each training day, peak power, resting elbow angle (ROM), pain pressure threshold (PPT), and visual analog scale of muscle soreness (VAS) were measured.
Procedures
The first laboratory visit consisted of a familiarization day to acquaint participants with the training procedures. During a familiarization, a Biodex was adjusted to the correct fit for each participant; the position was recorded and used during each training visit. Participants then completed submaximal and maximal reciprocal concentric isokinetic elbow flexion-extension muscle actions for the dominant arm at 120s on Biodex System 3 Pro isokinetic dynamometer. As they exercised participants were secured to the Biodex using chest, waist, leg, and ankle straps to limit extraneous movements. Participants practiced their performance of reciprocal concentric isokinetic elbow flexion-extension muscle actions at 30% peak torque. Torque was visually tracked using a real-time display on a computer screen and participants adjusted force output based on the visual feedback [11].
Training protocol
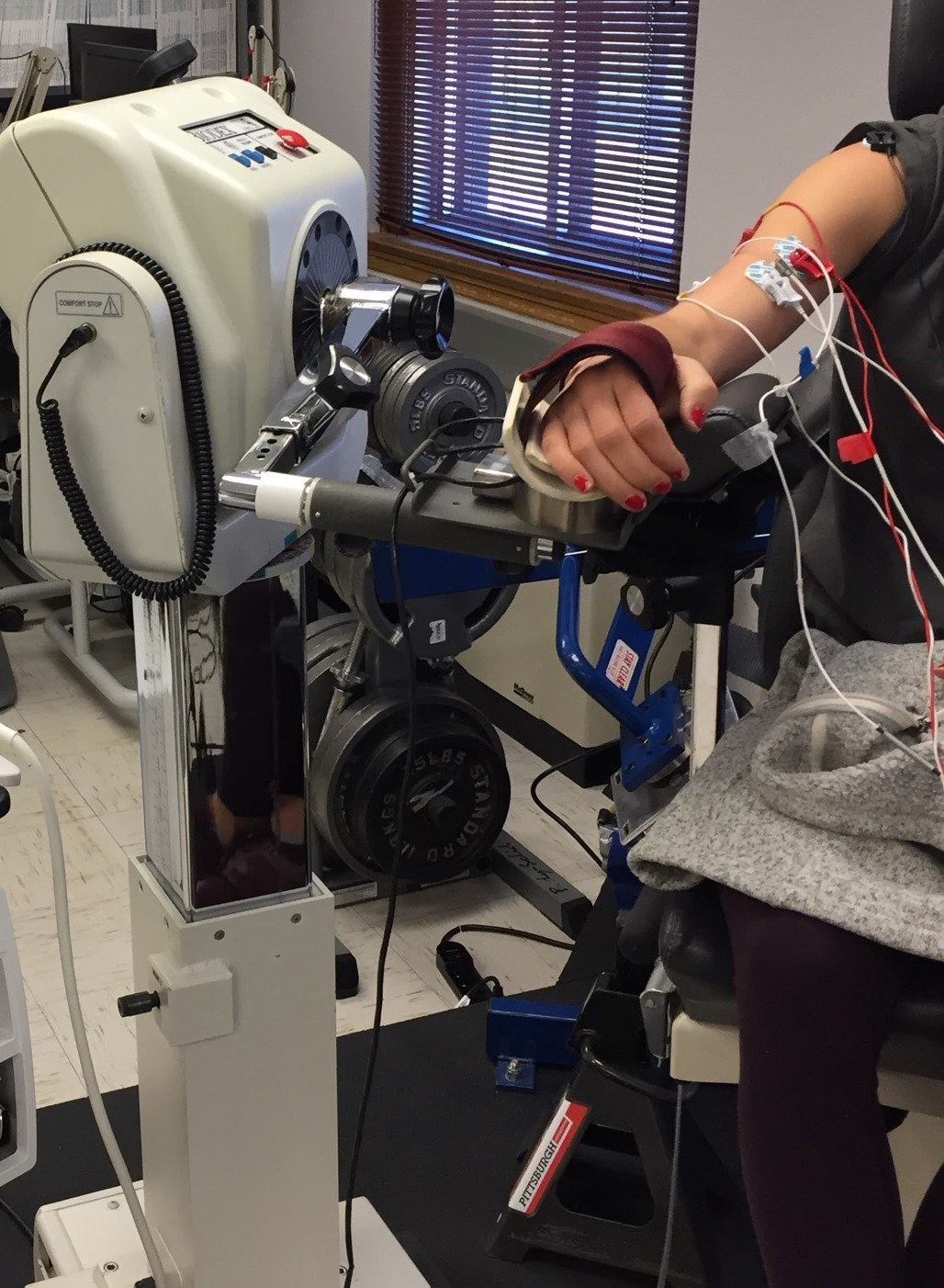
Participants completed two weeks of training at a frequency of three training days per week, separated by 48- to 72-h for a total of six training days. Each training day consisted of 75 submaximal (30% of peak torque) reciprocal concentric isokinetic elbow flexion-extension muscle actions completed over four sets (1 30, 3 15) separated by 30 s [11, 12]. All muscle actions were performed at 120s on a Biodex System 3 Pro isokinetic dynamometer and torque was visually tracked using a real-time display on a computer monitor (Fig. 1). The control group was assessed for all indices of DOMS on each training day but did not complete any training.
The KAATSU blood flow restriction cuff and EMG positioning on a Biodex System 3 Pro isokinetic dynamometer.
For the BFR group, a KAATSU resistance band was applied immediately prior to and was removed immediately after completing the 75 repetitions [11]. BFR was determined with a 30-mm wide resistance band (KAATSU Master, Sato Sports Plaza, Tokyo, Japan) placed on the proximal portion of the arm. The resistance band was inflated to 30 mmHg initially and progressively inflated and deflated over a 60-s period until the target pressure was reached. The target pressure was defined as 40% of the lowest pressure needed to completely occlude the brachial artery as indicated by doppler ultrasound [16, 17]. The total duration of BFR was approximately five minutes.
Time course of changes for indices of DOMS between LL BFR (), LL (), and control () across 6 training days. There were no significant interactions or main effects for Group or Time for A. peak power, B. ROM, and D. VAS. There was a significant interaction for C. PPT and follow-up analyses indicated that PPT was elevated at training day 5 relative to training day 2 for LL BFR only, but did not decrease from baseline. DOMS delayed onset muscle soreness; LL low-load resistance training without blood flow restriction; LL BFR low-load resistance training with blood flow restriction; PPT pain pressure threshold; ROM resting elbow angle; VAS visual analog scale. * Denotes significant effect ( 0.05) of Time (Day 5 Day 2).
Measurements
At the start of each training day, prior to the warm-up, exercise protocol, or application of BFR, ROM, PPT, and VAS were determined. ROM was determined as the resting angle between the forearm and upper arm using a goniometer (Smith & Nephew Rolyan, Inc., Menomonee Falls, USA) while the participant stood as their arm hung freely by their side [12]. A pressure algometer with a 1 cm flat rubber tip (Wagner FPX, Wagner Instruments, Greenwich, USA) was used to assess PPT. The unit was applied as pressure was constantly increased to the triceps brachii muscle at 66% of the distance from the olecranon and the cubital fossa on the lateral head of the triceps. Participants were asked to identify when the force (kg) applied was “slightly uncomfortable” [18] and the force (kg) at which this occurred was recorded. A scale from 0–10 was used to assess VAS where 0 corresponded to no soreness and 10 corresponded to severe soreness.
Following ROM, PPT, and VAS assessments, participants completed a standardized warm-up prior to performing two maximal concentric elbow extension muscle actions tested at 120s to determine peak power. Peak power was recorded and determined offline from a custom-fitted pancake load cell (Honeywell Inc, Model 41, NC). The highest peak power produced from two attempts was used for statistical analyses. The concentric muscle actions were performed over 120 of motion, where 0 corresponds to full extension at the elbow and 120 corresponds to full flexion at the elbow.
Statistical analysis
Peak power, ROM, PPT, and VAS were examined using separate three (Group [LL BFR, LL, and control]) x six (training days) mixed factorial ANOVAs. Significant interactions were decomposed with follow-up one-way repeated measures ANOVAs and one-way mixed factorial ANOVAs. All subsequent and independent or dependent samples t-tests were Bonferonni-corrected. Greenhouse-Geisser corrections were applied when sphericity was not met according to Maulchy’s test of sphericity. Partial eta-squared effect sizes () were calculated for each ANOVA and an alpha of 0.05 was considered statistically significant for all comparisons. All statistical analyses were performed using IBM SPSS v. 27 (IBM, Armonk, NY, USA).
Results
Peak power
There was no significant ( (2,27) 0.939, 0.500, 0.065) Group Time interaction or significant main effects for Time ( (2,27) 1.674, 0.145, 0.058) or Group ((2,27) = 0.213, = 0.809, = 0.016) for peak power (Fig. 2A).
Resting joint angle
There was no significant ( (2,27) 2.515, 0.098, 0.157) Group Time interaction or significant main effects for Time ( (2,27) 2.287, 0.141, 0.078) or Group ( (2,27) 3.209, 0.056, 0.192) for ROM (Fig. 2B).
Pain pressure threshold
There was a significant ( (2,27) 2.731, 0.020, 0.168) Group Time interaction for PPT and follow-up mixed factorial and repeated measure ANOVAs were performed. There was a significant ( (2,27) 4.342, 0.026, 0.240) simple main effect across Time for LL BFR (Day 5 Day 2) but no significant simple main effect across Time for LL or control. In addition, there were no significant ( (2,27) 0.458, = 0.637, 0.033) simple main effects for Group at any of the time points (Fig. 2C).
Muscle soreness
There was no significant ( (2,27) 1.152, 0.337, 0.079) Group Time interaction or significant main effects for Time ( (2,27) 0.645, 0.622, 0.023) or Group ( (2,27) 0.113, 0.667, 0.030) for VAS (Fig. 2D).
Discussion
The results of the present study indicate, in general, both LL BFR and LL are not associated with DOMS of the elbow extensors in previously untrained women. Specifically, there were no changes in peak power, VAS, or ROM across the six training days in any of the conditions. Furthermore, PPT increased at training day five relative to training day two for LL BFR only, but there were no reductions in PPT from baseline for any condition which would suggest muscle soreness. Therefore, these findings indicate both concentric low-load training interventions, regardless of BFR, did not induce DOMS as assessed by peak power, VAS, ROM, and PPT.
The results of this study were partially consistent with previous investigations [11, 12, 19, 20] that examined the effects of LL BFR and LL on indices of DOMS. For example, in previously untrained men, there were increases in perceived muscle soreness (VAS increased from 0 mm to 20 mm) following an initial bout of 75 unilateral eccentric-only elbow flexion muscle actions at 30% 1RM with BFR, but no changes in muscle soreness following concentric-only BFR muscle actions [12]. For both the eccentric-only group and concentric-only group, however, there were no changes in any other indices of DOMS including MVIC, muscle thickness, circumference, and ROM [12]. In recreationally active women, there were no changes in VAS, PPT, ROM, MVIC, or edema following six bouts of 75 unilateral isokinetic concentric-only or eccentric-only elbow flexion muscle actions at 30% 1RM with BFR [11]. Additionally, in trained males, there were no changes in VAS or peak power following an initial bout of 75 bilateral isotonic reciprocal (concentric-eccentric) leg press muscle actions at 20% 1RM with BFR [20]. Furthermore, after 12 repeated bouts, performed over a six day period, of 75 bilateral isotonic reciprocal (concentric-eccentric) knee extension muscle actions at 20% 1RM with BFR, there were no changes in plasma CK, myoglobin, or Interleukin 6 (IL-6), but increases in muscle cross-sectional area (75.1 9.1 cm to 77.6 8.3 cm), muscle volume (1,812 247 cm3 to 1863 236 cm), and strength (60 9 kg 1RM to 64 9 kg 1RM) [19]. Acute changes in muscle size were caused by venous pooling but they dissipated in approximately three hours which suggests changes in muscle size were due to increased muscle protein synthesis or decreased proteolysis [19].
However, the present findings were not consistent with those of Brandner and Warmington [21] and Alvarez et al. [22]. For example, in previously untrained men, as a result of 75 unilateral isotonic reciprocal (concentric-eccentric) elbow flexion muscle actions at 20% 1RM with BFR, VAS was significantly elevated for 48-h following continuous BFR (0 mm to 15 mm) and 72-h following intermittent BFR condition (0 mm to 20 mm) [21]. During the continuous BFR condition, the cuff was inflated immediately before exercise and remained inflated during the exercise bout, in the intermittent BFR condition the cuff was inflated before each set of exercise and deflated during the 30 second rest periods [21]. For untrained women, following a bout of approximately 75 (1 30–35, 3 15–18) unilateral isotonic reciprocal (concentric-eccentric) knee extension muscle actions at 20% 1RM with BFR, there was a significant (9.1%) decrease in MVIC 24-h post-exercise and 48-h post-exercise (9.3%) [22]. Additionally, there was a significant (12.2%) decrease in maximal voluntary concentric contraction (MVCC) 24-h post-exercise, and a significant increase in VAS 24-h (0 mm to 18 mm) and 48-h (0 mm to 16 mm) post-exercise. However, there were no changes in ROM from 24- to 96-h post-exercise [22]. Furthermore, there were also significant increases in muscle edema (as assessed by echo intensity) for the vastus laterals (increased from 22.3 AU to 29.4 AU) which remained elevated 24-, 48-, and 72-h post-exercise, and for the rectus femoris (increased from 24.48 AU to 34.68 AU) which remained elevated 24-, 48-, 72-, and 96-h post-exercise [22]. Together, these findings suggest DOMS was present for at least 48-hours post-exercise. In the investigation of Brandner and Warmington [21] however, the primary indicator of DOMS was VAS which exhibits poor reliability ( –0.346) when used individually compared to other indirect assessments or clusters of assessments of DOMS including MVIC and ROM [23, 24]. Furthermore, there were contrasting responses across the indirect assessments of DOMS reported by Alvarez et al. [22].
The present findings, in conjunction with previous investigations [11, 12, 19, 20], were also not consistent with low-load training protocols performed to volitional failure with or without BFR. For example, in untrained males, 5 sets of unilateral isotonic reciprocal (concentric-eccentric) knee extension muscle actions performed to volitional failure at 30% 1RM with BFR resulted in a 36-fold increase serum CK (137 26 IU/L to 4,954 2,773 IU/L) that peaked four days post-exercise and increased VAS from 0 cm to 5 cm and remained elevated six days after the initial bouts of exercise [15]. Additionally, myoglobin was elevated two (52 0 /L to 948 575 /L) and four days (601 395 g/L) post-exercise [15]. Similarly, in untrained males and females, four sets of unilateral isotonic reciprocal (concentric-eccentric) knee extension muscle actions performed to volitional failure (84 15 repetitions per bout) at 20% 1RM with BFR resulted in a seven-fold increase in serum CK (177 118 U/L to 1,224 968 U/L), increased VAS (39 mm 21 mm), and myoglobin (42 24 g/L to 253 238 g/L) followingseven repeated bouts performed over five days [9]. In untrained males and females, following four sets of unilateral isotonic reciprocal (concentric-eccentric) elbow flexion muscle actions performed to volitional failure at 40% 1RM with and without BFR, VAS increased in both LL BFR ( 15 mm at 0-h, 50 mm at 48-h) and LL ( 10 mm at 0-h, 30 mm at 48-h) immediately after exercise and remained elevated 24-h post-exercise [8].
Unlike repetitions to failure, it is possible LL BFR and LL interventions that utilize a 75-repetition scheme do not cause sufficient exercise stress to induce DOMS. For example, in the present study and those of previous investigations [11, 12, 19, 20] participants completed 75 repetitions (1 30, 3 15), in contrast to Sieljacks et al. [15] which entailed five sets to volitional failure or Bjørnsen et al. [9] which involved four sets to volitional failure. These differences in repetitions and sets may distinctly induce different physiological stresses. They include increased exercise volume, time under tension, and/or metabolic accumulation that together or separately may affect indices of DOMS uniquely. Collectively, our findings, in conjunction with previous investigations [11, 12, 19, 20] indicate LL BFR and LL resulted in little or no DOMS when performed over 75 repetitions (1 30, 3 15).
The results of the present study indicate LL BFR and LL resistance training was not associated with DOMS. These findings, in conjunction with previous investigations [25, 26, 27] that examined the ability of LL BFR and LL to elicit increases in muscle strength and size, suggest that LL BFR and LL training may be particularly useful among various populations including older adults, those undergoing rehabilitation, and athletes. Specifically, LL BFR and LL may allow for early post-surgical exercise conditioning [28, 29, 30], increased exercise program adherence [31, 32], and allow athletes to achieve positive muscular adaptations without experiencing the adverse effects of DOMS on sports performance [33].
One limitation of the current study is that a concen-tric-concentric training protocol was utilized. Although this is a common training protocol during isokinetic training, concentric-only contractions may limit the development of DOMS due to the absence of the eccentric phase. The eccentric phase of a muscle action has been associated with greater levels of z-line streaming and increased markers of DOMS, but muscle soreness has been observed following other training interventions [33]. For example, increased muscle soreness has been observed following concentric only contractions [34, 35, 36, 37], isometric only contractions [38, 39, 40, 41, 42, 43], electric stimulation contractions in the absences of voluntary muscle activation [44, 45], and endurance exercise [46, 47]. While it is possible that a concentric-only training protocol may limit the development of DOMS in the present study untrained individuals were recruited which would increase the probability of the development of DOMS due to the novel stimulus.
Conclusion
The results of the present study indicate LL BFR and LL did not induce DOMS for the elbow extensors in previously untrained women as assessed by peak power, VAS, ROM, or PPT. These findings were consistent with previous investigations that utilized LL BFR and LL interventions performed over 75 repetitions with various training loads (20–30% of maximum strength), muscle groups (elbow flexor, elbow extensor, and knee extensor), and muscle actions (reciprocal concentric-eccentric, reciprocal concentric-concentric, eccentric-only, and concentric-only). The present findings were not consistent with LL BFR and LL protocols that implemented repetitions to failure which may induce different physiological stresses that include increased exercise volume, time under tension, and/or metabolic accumulation that may affect the magnitude of DOMS uniquely.
Author contributions
CONCEPTION: Christopher E. Proppe, Paola M. Rivera, Ethan C. Hill and Terry J. Housh.
PERFORMANCE OF WORK: Christopher E. Proppe.
INTERPRETATION OR ANALYSIS OF DATA: Christopher E. Proppe, Paola M. Rivera, Ethan C. Hill Terry J. Housh, Joshua L. Keller, Cory M. Smith, John Paul V. Anders, Richard J. Schmidt, Glen O. Johnson and Joel T. Cramer.
PREPARATION OF THE MANUSCRIPT: Christopher E. Proppe.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: All authors.
Ethical considerations
The study was approved by the University of Nebraska Institutional Review Board for Human Subjects and all participants completed a health history questionnaire and signed written informed consent prior to training (20170517195EP).
Funding
This research was supported by the NASA Nebraska Space Grant (Grant No. 44-0307-1019-457).
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors have no conflicts of interest to report.
References
1.
SchoenfeldBJ. The mechanisms of muscle hypertrophy and their application to resistance training. J Strength Cond Res.2010; 24: 2857-72. doi: 10.1519/JSC.0b013e3181e840f3.
2.
RobertsMDHaunCTMobleyCBMumfordPWRomeroMARobersonPA, et al. Physiological differences between low versus high skeletal muscle hypertrophic responders to resistance exercise training: Current perspectives and future research directions. Front Physiol.2018; 9: 834. doi: 10.3389/.
3.
KubotaASakurabaKSawakiKSumideTTamuraY. Prevention of disuse muscular weakness by restriction of blood flow. Med Sci Sports Exerc.2008; 40: 529-34. doi: 10.1249/MSS.0b013e31815ddac6.
4.
PearsonSJHussainSR. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med.2015; 45: 187-200. doi: 10.1007/s40279-014-0264-9.
5.
SchoenfeldBJGrgicJOgbornDKriegerJW. Strength and hypertrophy adaptations between low-vs. high-load resistance training: A systematic review and meta-analysis. J Strength Cond Res.2017; 31: 3508-23. doi: 10.1519/JSC.0000000000002200.
6.
TakaradaYNakamuraYArugaSOndaTMiyazakiSIshiiN. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J Appl Physiol.2000; 88: 61-5. doi: 10.1152/jappl.2000.88.1.61.
7.
ClarksonPMSayersSP. Etiology of exercise-induced muscle damage. Can J Appl Physiol.1999; 24: 234-48. doi: 10.1139/h99-020.
8.
FarupJde PaoliFBjergKRiisSRinggardSVissingK. Blood flow restricted and traditional resistance training performed to fatigue produce equal muscle hypertrophy. Scand J Med Sci Sports.2015; 25: 754-63. doi: 10.1111/sms.12396.
9.
BjørnsenTWernbomMLøvstadAPaulsenGD’SouzaRFCameron-SmithD, et al. Delayed myonuclear addition, myofiber hypertrophy, and increases in strength with high-frequency low-load blood flow restricted training to volitional failure. J Appl Physiol.2019; 126: 578-92. doi: 10.1152/japplphysiol.00397.2018.
10.
CurtyVMMeloABCaldasLCGuimarães-FerreiraLde SousaNFVassalloPF, et al. Blood flow restriction attenuates eccentric exercise-induced muscle damage without perceptual and cardiovascular overload. Clin Physiol Funct Imaging.2018; 38: 468-76. doi: 10.1111/cpf.12439.
11.
HillECHoushTJSmithCMKellerJLSchmidtRJJohnsonGO. Eccentric and concentric blood flow restriction resistance training on indices of delayed onset muscle soreness in untrained women. Eur J Appl Physiol.2019; 119: 2363-73. doi: 10.1007/s00421-019-04220-8.
12.
ThiebaudRSYasudaTLoennekeJPAbeT. Effects of Low-Intensity Concentric and eccentric exercise combined with blood flow restriction on indices of exercise-induced muscle damage. Interv Med Appl Sci.2013; 5: 53-9. doi: 10.1556/IMAS.5.2013.2.1.
13.
CountsBRRossowLMMattocksKTMouserJGJesseeMBBucknerSL, et al. Let’s talk about sex: where are the young females in blood flow restriction research? Clin Physiol Funct Imaging.2018; 38: 1-3. doi: 10.1111/cpf.12394.
14.
FaulFErdfelderEBuchnerALangA-G. Statistical power analyses using G*Power 31: Tests for correlation and regression analyses. Behav Res Methods.2009; 41: 1149-60. doi: 10.3758/BRM.41.4.1149.
15.
SieljacksPMatzonAWernbomMRinggaardSVissingKOvergaardK. Muscle damage and repeated bout effect following blood flow restricted exercise. Eur J Appl Physiol.2016; 116: 513-25. doi: 10.1007/s00421-015-3304-8.
16.
CountsBRDankelSJBarnettBEKimDMouserJGAllenKM, et al. Influence of relative blood flow restriction pressure on muscle activationand muscle adaptation. Muscle Nerve.2016; 53: 438-45. doi: 10.1002/mus.24756.
17.
LoennekeJPKimDFahsCAThiebaudRSAbeTLarsonRD, et al. Effects of exercise with and without different degrees of blood flow restriction on torque and muscle activation. Muscle Nerve.2015; 51: 713-21. doi: 10.1002/mus.24448.
FujitaTBrechueWFKuritaKSatoYAbeT. Increased muscle volume and strength following six days of low-intensity resistance training with restricted muscle blood flow. Int J KAATSU Train Res.2008; 4: 1-8. doi: 10.3806/ijktr.4.1.
20.
WilsonJMLoweryRPJoyJMLoennekeJPNaimoMA. Practical blood flow restriction training increases acute determinants of hypertrophywithout increasing indices of muscle damage. J Strength Cond Res.2013; 27: 3068-75. doi: 10.1519/JSC.0b013e31828a1ffa.
AlvarezIFDamasFde BiazonTMPMiqueliniMDomaKLibardiCA. Muscle damage responses to resistance exercise performed with high-load versus low-load associated with partial blood flow restriction in young women. Eur J Sport Sci.2020; 20: 125-34. doi: 10.1080/17461391.2019.1614680.
23.
DamasFNosakaKLibardiCChenTUgrinowitschC. Susceptibility to exercise-induced muscle damage: A cluster analysis with a large sample. Int J Sports Med.2016; 37: 633-40. doi: 10.1055/s-0042-100281.
24.
WarrenGLLoweDAArmstrongRB. Measurement tools used in the study of eccentric contraction-induced injury. Sports Med.1999; 27: 43-59. doi: 10.2165/00007256-199927010-00004.
25.
LaurentinoGCUgrinowitschCRoschelHAokiMSSoaresAGNevesM, et al. Strength training with blood flow restriction diminishes myostatin gene expression. Med Sci Sports Exerc.2012; 44: 406-12. doi: 10.1249/MSS.0b013e318233b4bc.
26.
SchoenfeldBJPetersonMDOgbornDContrerasBSonmezGT. Effects of low- vs. high-load resistance training on muscle strength and hypertrophy in well-trained men. J Strength Cond Res.2015; 29: 2954-63. doi: 10.1519/JSC.0000000000000958.
27.
VechinFCLibardiCAConceiçãoMSDamasFCavaglieriCRChacon-MikahilMPT, et al. Low-intensity resistance training with partial blood flow restriction and high-intensity resistance training induce similar changes in skeletal muscle transcriptome in elderly humans. Appl Physiol Nutr Metab.2019; 44: 216-20. doi: 10.1139/apnm-2018-0146.
28.
HughesLRosenblattBHaddadFGissaneCMcCarthyDClarkeT, et al. Comparing the effectiveness of blood flow restriction and traditional heavy load resistance training in the post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: A UK national health service randomised controlled trial. Sports Med.2019; 49: 1787-805. doi: 10.1007/s40279-019-01137-2.
29.
OhtaHKurosawaHIkedaHIwaseYSatouNNakamuraS. Low-load resistance muscular training with moderate restriction of blood flow after anterior cruciate ligament reconstruction. Acta Orthop Scand.2003; 74: 62-8. doi: 10.1080/00016470310013680.
30.
TakaradaYTakazawaHIshiiN. Applications of Vascular Occlusion diminish disuse atrophy of knee extensor muscles. Med Sci Sports Exerc.2000; 32: 2035-9. doi: 10.1097/00005768-200012000-00011.
31.
GeneenLJMooreRAClarkeCMartinDColvinLASmithBH. Physical activity and exercise for chronic pain in adults: An overview of cochrane reviews. In: The Cochrane Collaboration, editor. Cochrane Database Syst. Rev., Chichester, UK: John Wiley & Sons, Ltd; 2017, p. CD011279.pub2. doi: 10.1002/14651858.CD011279.pub2.
32.
TrostZFranceCRThomasJS. Pain-related fear and avoidance of physical exertion following delayed-onset muscle soreness. Pain.2011; 152: 1540-7. doi: 10.1016/j.pain.2011.02.038.
ByrnesWCClarksonPMKatchFI. Muscle soreness following resistance exercise with and without eccentric contractions. Res Q Exerc Sport.1985; 56: 283-5. doi: 10.1080/02701367.1985.10605375.
35.
KangM-SKimJLeeJ. Effect of different muscle contraction interventions using an isokinetic dynamometer on muscle recovery following muscle injury. J Exerc Rehabil.2018; 14: 1080-4. doi: 10.12965/jer.1836440.220.
36.
TalagTS. Residual muscular soreness as influenced by concentric, eccentric, and static contractions. Res Q Am Assoc Health Phys Educ Recreat.1973; 44: 458-69. doi: 10.1080/10671188.1973.10615226.
37.
WilloughbyDSVanenkCTaylorL. Effects of concentric and eccentric contractions on exercise induced muscle injury, inflammation, and serum IL-6. J Exerc Physiol.2003; 6: 8-15.
38.
AldayelAJubeauMMcGuiganMRNosakaK. Less indication of muscle damage in the second than initial electrical muscle stimulation bout consisting of isometric contractions of the knee extensors. Eur J Appl Physiol.2010; 108: 709-17. doi: 10.1007/s00421-009-1278-0.
39.
AllenTJJonesTTsayAMorganDLProskeU. Muscle damage produced by isometric contractions in human elbow flexors. J Appl Physiol.2018; 124: 388-99. doi: 10.1152/japplphysiol.00535.2017.
40.
ClarksonPByrnesWMcCormickKTurcotteLWhiteJ. Muscle soreness and serum creatine kinase activity following isometric, eccentric, and concentric exercise. Int J Sports Med.1986; 7: 152-5. doi: 10.1055/s-2008-1025753.
41.
JubeauMMuthalibMMilletGYMaffiulettiNANosakaK. Comparison in muscle damage between maximal voluntary and electrically evoked isometric contractions of the elbow flexors. Eur J Appl Physiol.2012; 112: 429-38. doi: 10.1007/s00421-011-1991-3.
42.
PhilippouAMaridakiMBogdanisGC. Angle-specific impairment of elbow flexors strength after isometric exercise at long muscle length. J Sports Sci.2003; 21: 859-65. doi: 10.1080/0264041031000140356.
43.
TrifflettiPLitchfieldPEClarksonPMByrnesWC. Creatine kinase and muscle soreness after repeated isometric exercise. Med Sci Sports Exerc.1988; 20: 242-8. doi: 10.1249/00005768-198806000-00005.
44.
FouréANosakaKWegrzykJDuhamelGLe TroterABoudinetH, et al. Time course of central and peripheral alterations after isometric neuromuscular electrical stimulation-induced muscle damage. PLoS ONE.2014; 9: e107298. doi: 10.1371/journal.pone.0107298.
45.
MackeyALBojsen-MollerJQvortrupKLangbergHSuettaCKalliokoskiKK, et al. Evidence of skeletal muscle damage following electrically stimulated isometric muscle contractions in humans. J Appl Physiol.2008; 105: 1620-7. doi: 10.1152/japplphysiol.90952.2008.
46.
NosakaKNewtonMSaccoP. Muscle damage and soreness after endurance exercise of the elbow flexors. Med Sci Sports Exerc.2002; 34: 920-7. doi: 10.1097/00005768-200206000-00003.
47.
VickersAJ. Time course of muscle soreness following different types of exercise. BMC Musculoskelet Disord.2001; 2: 5. doi: 10.1186/1471-2474-2-5.