
Abstract
BACKGROUND:
Individuals may suffer from repeated sprints-induced muscle damage, which could lead to a prolonged recovery period, thereby influencing subsequent closely-scheduled training or competitions.
OBJECTIVE:
To examine whether an initial muscle-damaging sprint exercise could confer a protective effect against muscle damage induced by the subsequent identical exercise performed four days later.
METHODS:
Fourteen physically-active men completed two sprinting bouts (15 sets of 30-m maximal sprints) with 4 days apart. Before, 24, 48, and 72 hours after both bouts, muscle damage markers were measured. In addition, time trial, along with the peak heart rate (HR) and rating of perceived exertion (RPE) during each sprint set were also recorded.
RESULTS:
Comparing to the initial bout, less muscle soreness and faster recoveries of the knee flexion eccentric peak torque and angle of peak torque were found following the second bout. In addition, the time trial and HR for each sprint set were not different between the two bouts, but the average RPE was less during the second bout (
CONCLUSIONS:
The protective effect from the exposure to the initial sprint was evident. Thus, repeated exposures to the sport-specific sprints can positively influence the symptoms of muscle damage without influencing the sprinting performance.
Introduction
Exercise-induced muscle damage (EIMD) is usually associated with the exercises and sporting activities that partly or entirely consist of unaccustomed eccentric muscle actions [1]. Different from muscle fatigue, what makes EIMD peculiar are the prolonged muscle damage symptoms such as the muscle soreness, the inflammation, and the decrements in muscular functions, which can reduce subsequent performance [2]. Thus, recovery enhancement from EIMD is especially important for individuals who have densely scheduled (2–3 times per week) competitions (e.g., athletic population) or training sessions (e.g., both athletic and recreationally-active population). Despite the prolonged muscle damage symptoms from the EIMD, skeletal muscles have the ability to adapt to this type of the exercise rapidly. Specifically, when compared to the first exercise bout-induced muscle damage, it has been well-documented that the symptoms of EIMD can be attenuated after a second bout of identical muscle-damaging exercise [1]. This specific adaptation is termed as the repeated bout effect (RBE), and it has been reported to occur as early as 1–2 days following the initial bout of exercise [3], and it can last more than 6 months [4]. Therefore, strength and conditioning specialists may be able to take advantage of the RBE to design specific strategies or training programs to enhance recovery following intense competitions or exercise training sessions.
Several studies [5, 6, 7] have examined the potential RBE induced by the exposure to the initial muscle-damaging exercise bout in different populations. Conflicting results have been reported, with the elite level athletes (e.g., National League or English University Premier Division soccer players) showing limited RBE [7], whereas a positive RBE has been shown in collegiate soccer players and female dancers [5, 6]. Two worth-mentioning areas from these studies should be pointed out: 1. The sport-specific muscle-damaging exercise (repeated maximal sprints, and the Loughborough Intermittent Shuttle Test) bouts were used in these studies, making the findings more interpretable regarding the related practical situations. Indeed, these high-intensity intermittent sprints are usually performed repetitively in field sports such as soccer, basketball, rugby, and football. 2. These studies have used a 2-week [5, 7] and 4-week [6] rest period between the two repeated bouts, for the purpose of examining the RBE from the initial sport-specific exercise bout. While a 2-to 4-week period is a suitable experimental design specifically for examining the RBE, this time frame may not be feasible in practical situations where consecutive competitions or training sessions are usually separated by days. Considering the rapid adaptations (as mentioned above, as early as 1–2 day) could occur following the initial muscle-damaging exercise bout, it would be interesting to examine the potential prophylactic effect a few days after an initial sport-specific muscle-damaging exercise bout.
In the past, a report has demonstrated that a sport-specific sprinting exercise bout (12 sets of 30-meter maximal intermittent sprints) can induce muscle damage, even in the athletic populations [8]. Based on these findings, along with the ones from others [6, 9], where similar sprinting exercise protocols were performed, some muscle damage indices did not return to baseline even three days after the initial sprints. Thus, if the second identical sprinting bout were performed around this point, it is difficult to predict whether there would be an attenuated or exacerbated response for the muscle damage markers. In addition, it has not been studied whether the performance of the second bout would differ from that of the initial bout, considering the damaged muscle group may not be fully recovered. Therefore, the primary purpose of this study was to examine whether the initial sport-specific muscle-damaging sprint exercise could confer a protective effect against muscle damage induced by a subsequent bout of identical exercise performed only four days later in physically active men. In addition, the secondary purpose of this study was to examine the sprinting-related performance during the second bout of muscle-damaging exercise would be different from the initial one. As far as we know, this is the first study to examine the potential RBE in a sport-specific muscle-damaging protocol setup within a short time period (4 days apart). It was hypothesized that, the EIMD observed after the second bout of the sprints would be lower than the first bout. In addition, we expected to see the sprinting performance (e.g., time trial for each sprint) during the second bout would not differ from that during the initial bout.
The flow chart of the experimental design.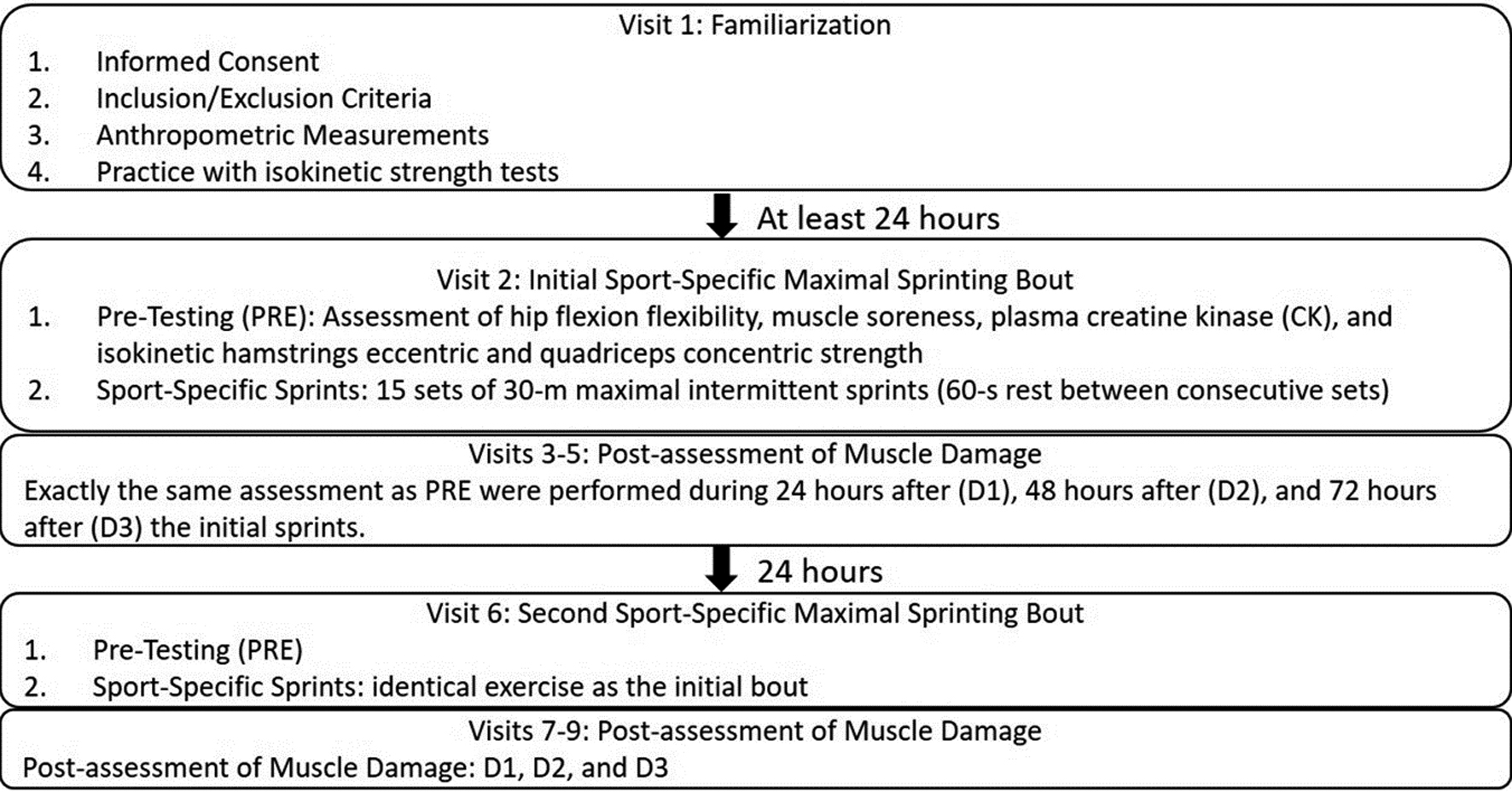
Subjects
Fourteen healthy college-aged men (mean
Design
To examine the effects of the second bout of maximal sprinting exercise on muscle damage markers four days after the identical initial bout, nine separate visits to the laboratory were required to complete this study (Fig. 1). After the first visit as the familiarization, the following eight visits were conducted on eight consecutive days, during which the two identical muscle-damaging maximal sprinting exercise bouts were performed with 96 hours apart (Visit 2 and Visit 6). All dependent variables (muscle damage markers) were measured before (PRE), 24 (D1), 48 (D2), and 72 (D3) hours after both bouts of sprints on the dominant side of the subjects’ thigh muscles based on their kicking preferences. In addition, the sprint-related variables were also measured during both sprinting bouts.
Procedures
During the familiarization visit (Visit 1), all subjects visited the laboratory to receive instructions and to participate in a familiarization trial specifically to practice isokinetic strength tests. At least 24 hours after the familiarization, the subjects returned to the laboratory for the purpose of getting the PRE-measurements, followed by performing the first bout of sport-specific sprints. Upon arrival, the subjects were asked to perform 5 minutes of jogging at a self-selected speed. Following the warm-up exercise, dependent variable measurements were taken by the investigators with the order of hip flexion flexibility, muscle soreness, plasma creatine kinase (CK), and isokinetic knee flexion eccentric strength. Following the completion of the PRE-measurements, the subjects were asked to perform a 5-minute dynamic sprint drills which consisted of several running bouts at 60%–100% of perceived maximum speed, high knees, heel-flicks, and walking lunges. In addition, the subjects also performed self-administered static stretching exercises specifically targeting the gluteus, psoas, adductors, hamstrings and quadriceps muscles. The maximal sprinting protocol began 5 minutes following the final set of sprint drill or static stretches. Specifically, 15 sets of 30-m maximal intermittent sprints were performed by the subjects on the concrete floor, with a 10-m acceleration and a 15-m deceleration for each sprint set. The rest interval between consecutive sprint sets were 60 seconds. Each subject was verbally encouraged to give a maximal effort during every sprint set. For the sprint-related variables, the time to complete each sprint (time trial) was measured through a FitLight device (FitLight Corp., ON, Canada). The peak heart rate (HR) was recorded through a heart rate monitor (Polar RS 800, Polar Electro Inc., Kempele, Finland) during each sprint set. In addition, the rating of perceived exertion (RPE) was recorded using the Borg Rating of Perceived Exertion Scale [10] at the end of each spring set. Twenty-four (D1), 48 (D2), and 72 (D3) hours after the sprints, dependent variables were measured again with the same order and manner as they were measured at the PRE. Separated by four days from the first bout, the second bout of the sprinting exercise with its associated measurements (PRE, D1, D2, and D3) were performed with the exact same manner as they were performed for the initial bout.
Dependent variables
Hip flexion passive range-of-motion (ROM)
The passive straight-leg raises (PSLR) test was used to measure the hip flexion passive ROM. The subjects were required to lie supine on a padded plinth, with both waist and the nondominant leg fixed by a strap. One investigator held the subject’s dominant ankle with the knee fully extended, and the inclinometer (Digital Inclinometer, Model # A800; JIN-BOMB Inc, Kaohsiung, Taiwan) was placed over the distal tibia. The dominant leg was then raised up slowly to the point that the subject first felt tension or slight stretch from the hamstring muscle. The value from the inclinometer was then recorded as the hip flexion passive ROM. This test was repeated at least 3 times with 15-second rest between trials. If the values from any two trials differed more than 2 degrees, extra trials were conducted. The average of the three closest trials was calculated and recorded as the hip flexion passive ROM.
Muscle soreness
The level of muscle soreness was quantified using a visual analog scale that had a 100-mm continuous line with “not sore at all” on one side (0 mm) and “very, very sore” on the other side (100 mm). The investigator asked the participant to rate his perceived soreness on the visual analog scale when the knee joint was passively extended through the ROM that used for the maximal isokinetic strength measures.
Plasma creatine kinase (CK)
Approximately 10 ml of venous blood was drawn using a standard venipuncture technique from the cubital fossa region of the arm and centrifuged for 10 min to extract plasma. Plasma samples were stored at
Isokinetic knee flexion eccentric strength
Isokinetic strength testing was performed to assess the muscle function of the hamstrings using a Biodex System Pro 4 isokinetic dynamometer (Biodex Medical Systems, Inc., Shirley, NY, USA). The subject sat in a comfortable, upright position on the dynamometer. The mechanical axis of the dynamometer was aligned with the lateral epicondyle of the knee, and the trunk, waist, thigh, and chest were stabilized with belts to minimize extraneous body movements. The range of motion of the dominant knee was set before the strength testing. The subject performed a standardized warm-up composed of 3 submaximal (50% of perceived maximal effort) knee flexion eccentric contractions at 30
Statistical analyses
To compare the sprint-related performance variables between all 15 sets from the first and the second sprinting bouts, separate two-way repeated-measures (bout [initial vs. second]
Sprint-related variables at each sprint set during two sport-specific maximal intermittent sprint bouts. Sub-figure A, B, and C are demonstrating Mean 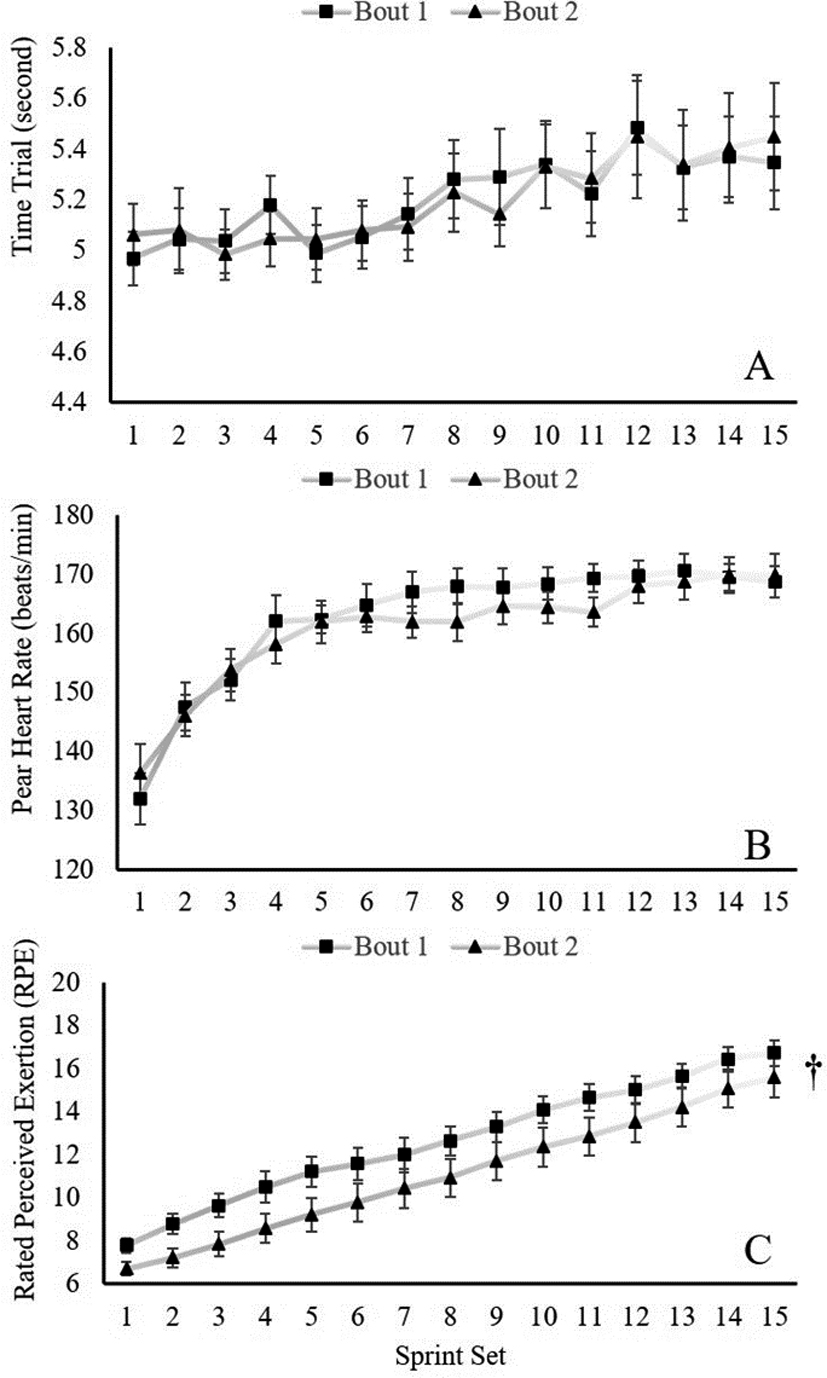
The responses of Mean 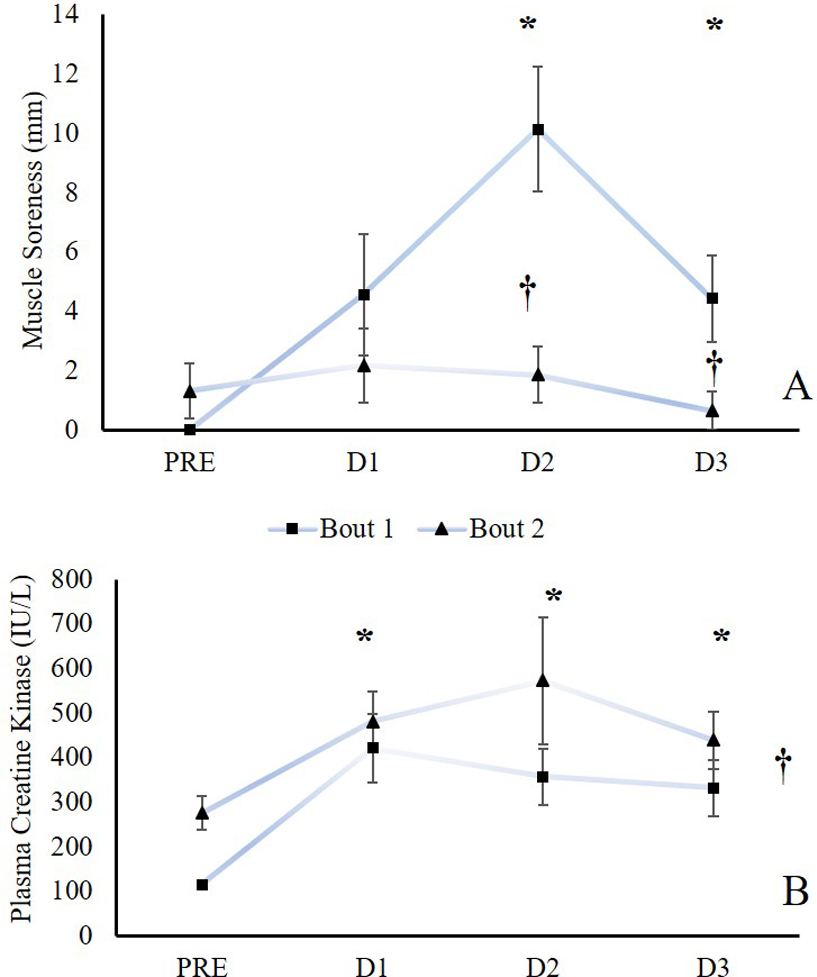
The responses of Mean 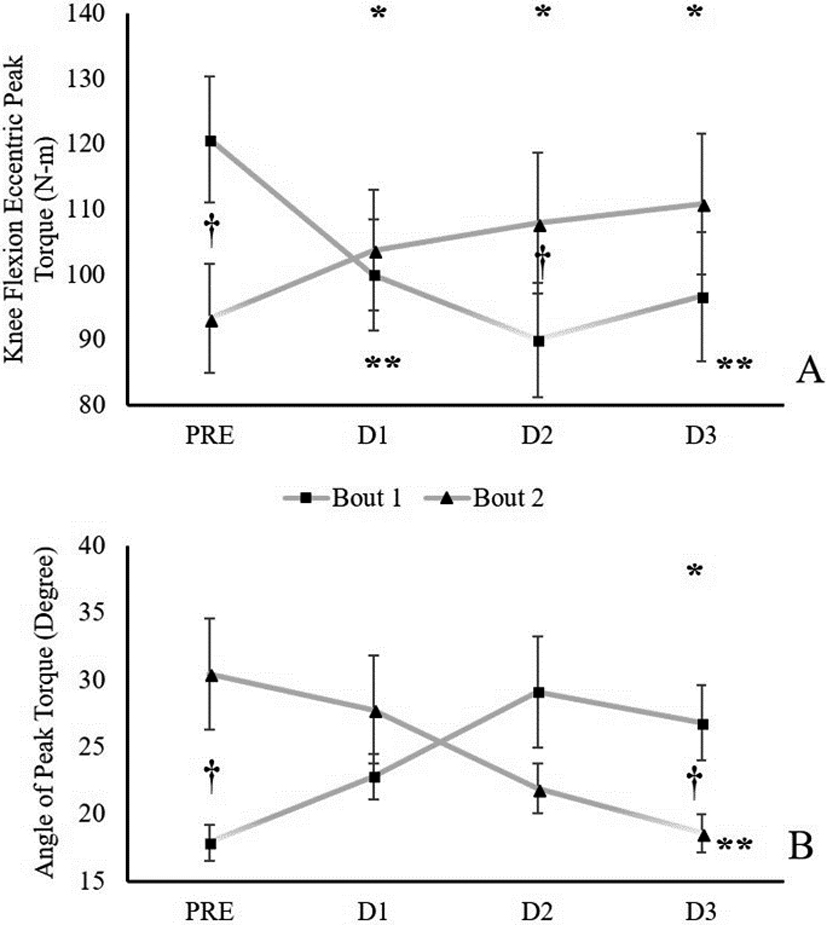
Sprint-related variables between the initial and second sprinting bouts
For all the sprint-related performance variables (time trial, HR, and RPE for each sprint set), the results from the 2-way repeated-measures ANOVAs indicated that there were no bout
The comparisons of muscle damage markers’ responses after initial and second sprint bouts
To determine whether there was a potential prophylactic effect from the exposure to the initial muscle-damaging sport-specific sprinting bout, comparisons of muscle damage indices were made between the two bouts across time (PRE, D1, D2, and D3):
Hip flexion passive ROM
The results from the 2-way repeated measures ANO VA indicated no significant interaction (
Muscle soreness
The 2-way repeated measures ANOVA detected a significant bout
Mean
Standard Deviation (SD) before (PRE), 24 hours (D1), 48 hours (D2), and 72 hours after (D3) the initial and second sport-specific sprinting bouts for hip flexion passive ROM, muscle soreness, plasma creatine kinase, knee flexion isokinetic eccentric peak torque and angle of peak torque
Mean
The results from the 2-way repeated measures ANO VA indicated that there was no significant interaction. However, there were main effects for both bout (
Knee flexion isokinetic eccentric strength
For the knee flexion isokinetic eccentric strength parameters (PT and APT), the results from the separate 2-way repeated measures ANOVAs indicated that there were significant 2-way interactions for both variables (PT:
The pairwise comparisons showed that the PT values decreased from PRE to D1 (
For the knee flexion eccentric APT, the pairwise comparisons showed that the APT values increased from PRE to D3 (
Discussion
The purposes of this study were: 1) to examine whether the initial sport-specific muscle-damaging sprint exercise could confer a protective effect against a subsequent bout of identical exercise performed four days after, and 2) to compare the sprint-related performance variables between two closely-scheduled maximal sprinting bouts. The presumption to answer these research questions is the presence of EIMD following the initial sport-specific sprint exercise bout. Based on our results, several muscle damage indices showed positive responses following the initial 15 by 30-meter sprints. Specifically, the prolonged elevations of muscle soreness score (peaked at D2) and plasma CK concentration (peaked at D1) [12] have confirmed our expectation. In addition to the prolonged depression of knee flexion eccentric strength, the angle of peak torque of the eccentric knee flexion also increased and peaked at D3. This potentially suggested a shifted length-tension relation in the direction of longer muscle lengths [13]. Thus, the initial sport-specific sprint exercise induced muscle damage.
Performance comparisons between the initial and the second sprint bouts
With the presence of EIMD and its prolonged symptoms, which could be detrimental to the subsequent performance, it was also important to compare the sprint-related variables between the two exercise bouts separated by 96 hours. Based on our findings, all the variables (time trial, HR, and RPE for each sprint set) gradually increased throughout the 15-set intermittent maximal sprinting protocol. This indicates that the intermittent maximal sprints imposed greater physiologic stress, resulting in continued decrements in performance (longer time to complete each sprint set) throughout the sprint bout [14]. When comparing the performance and physiologic parameters between two bouts, no difference was found for the time trial or the HR, but interestingly, the RPE was generally lower by a 2-point scale during the second bout than the initial bout of the sprints. These findings are in agreement with the ones from Leeder et al. [7], where 5 sets of intensity-varying 15-minute Loughborough Intermittent Shuttle Test were performed by well-trained national or college athletes. It is worth mentioning that the training statuses (physically active men vs. well-trained national or college athletes), the running protocols (15 sets of 30-m intermittent maximal sprints vs. 5 sets of intensity-varying 15-minute Loughborough Intermittent Shuttle Test), as well as the rest periods between two bouts (4 days vs. 14 days) are different between these experiments. Even with all these differences, however, it is likely that the initial sprinting bout-induced muscle damage did not affect the second bout’s sprint time performance, given the 4-day rest period. Moreover, since the subjects were not accustomed to the intermittent maximal sprint exercise, the reduced RPE during the second bout was likely due to the habituation to the level of exertion [7], given that the second bout of sprints induced similar physiologic stress (heart rate responses) as the initial one did.
The protective effect from the initial bout?
Based on the results, lower levels of muscle soreness were found at both D1 and D2 after the second bout, when compared to the initial one. In fact, the muscle soreness scores were not elevated after the second sprinting bout, primarily due to the fact that 9 of the subjects reported “not sore at all” (muscle soreness
It is important to mention that the responses of different muscle damage markers do not necessarily correlate with each other in terms of magnitude and time-course after a muscle-damaging exercise bout [12]. Generally speaking, the blood CK activity increases dramatically 1–2 days and may reach the peak within 4–5 days after muscle-damaging exercises [16]. As shown from our data, the CK level was still elevated 3 days after the sport-specific sprints, it was possible therefore, the CK response after the second sprinting bout might still have partly represented EMID from the initial muscle-damaging bout. In addition, just like previous literature suggested [12], our CK data also showed large inter-subject variation especially after the second sprint bout, which challenges its use as a meaningful marker of EIMD. In contrast, muscle soreness develops at 1 day and peaks 2–3 days after muscle-damaging exercises [16]. Indeed, it is possible that the dampened muscle soreness response after the second bout could be attributed to familiarization to the sensation of pain [17]. However, previous review has suggested that muscle soreness can be a result of the increase of the inflammatory-induced tissue osmotic pressure, which triggers nociceptors to induce the pain sensation [18]. Regardless, our finding regarding the muscle soreness response was accompanied by the faster recoveries of both knee flexion peak torque and angle of peak torque after the second sprint bout, indicating the recovery of the muscle fiber membrane damage. Therefore, the protective effect from the exposure to the initial sport-specific sprint was positive, even when the second bout was performed only 4 days after.
Limitations
With some novel findings which can potentially provide practical information for sports performance and training purposes, this study however, does have some worth-mentioning limitations. Primarily, without a control group (only performing the initial sprints but getting muscle damage markers measured for the next 7 days) for the study, it was impossible to monitor how long the sport-specific sprints-induced muscle damage truly would have lasted, because some damage markers (plasma CK, knee flexion peak torque, and angle for peak torque) did not return to the baseline at the onset of the second sprint bout. That being said, this could have influenced the second sprint bout’s performance and physiologic variables as well as the subsequent muscle damage markers’ responses. Regardless, the second sprinting bout’s performance was not affected, and more importantly, there were evidences showing the protective effect from the previous muscle-damaging sprints. Second, when interpreting the results of the current study, it is important to be aware that these findings were based on healthy and physically-active individuals, meaning the related protective effect may or may not be observed in different populations (e.g., high-trained athletes who normally sprint during competitions or training). Thus, future studies are still needed to shed light onto this topic in a variety of populations.
In conclusion, for healthy physically-active young men who are not accustomed to maximal intermittent sport-specific sprints, performing a sport-specific sprinting exercise induced muscle damage. Even though some muscle damage markers (e.g., knee flexor strength) were not recovered to the baseline 4 days after the initial bout, the subjects’ performance and heart rate responses during the exact same second sprints were not affected. In addition, less muscle soreness and greater strength performance recovery following the second bout of sprints suggested a protective effect from the exposure to the initial muscle-damaging sprints. The current study suggests that repeated exposure of sport-specific maximal intermittent sprints even within a relatively short time period (e.g., 4 days) can positively influence symptoms of muscle damage, recovery, and adaptation, without sacrificing the sports performance. Therefore, training strategies can be specifically developed for specific individuals for the purposes of attenuating muscle damage and enhancing recovery between closely scheduled training sessions.
Footnotes
Acknowledgments
The authors would like to thank all the participants who took time out of their schedules to help with this project.
Conflict of interest
The authors declare no conflict of interest.