
Abstract
BACKGROUND:
Combining strength training (ST) with unstable surfaces (US) is a promising complementary approach to traditional ST to optimize muscle strength and balance in different populations.
OBJECTIVE:
To evaluate the effects of traditional ST and ST+US on grip strength, flexibility and quality of life in older women.
METHODS:
Fifty-eight older women were randomly assigned into ST (
RESULTS:
At completion of 24-weeks, compared with control group, traditional ST promote flexibility gains [SRT
CONCLUSION:
Traditional strength exercises were effective to improve flexibility and health-related quality of life among healthy older women. Combining unstable devices with traditional exercise did not provide additional gains in order to promote flexibility and quality of life.
Introduction
The physical decline which occurs with aging alters physical fitness components such as strength, flexibility and balance, leading to frailty and increased chances of falls in older adults [1, 2, 3]. Strength training (ST) has been widely recommended as a strategy to improve health parameters and functional independence in older adults. In this sense, there is a growing number of studies that advance and support the inclusion of ST for strength, flexibility [4, 5] and balance [6, 7, 8] gains in older adults, and consequent functional improvement.
In fact, older adults experience impaired functional ability and self-efficacy over the years [9]. Thus, in addition to the physical benefits, the Center for Disease Control and Prevention (CDC) reinforces the importance of mechanisms which not only improve functionality but also the quality of life in older adults [10]. However, although quality of life is a multifaceted phenomenon, the self-efficacy and overall well-being of older adults are significantly influenced by physical activity. Improvement in cardiovascular and functional parameters promoted by the exercise gives older adults autonomy and well-being [9].
Mobility is one of the domains of quality of life, and has been significantly associated with physical exercise practice [11]. Older adults with less mobility and functional independence are less involved in exercises [11], suggesting that engaging in regular physical exercises like strength, balance and flexibility training is important for achieving higher quality of life (QoL) in older people. In this view, other studies involving ST have also shown significant effects to improve the well-being in this population [9, 12].
Traditional resistance training programs focus on developing strength gain and muscle mass to control the deleterious effects of sarcopenia in older adults. The insertion of unstable surfaces at strength training (ST
Studies examining the effects of ST
Considering the importance of strength training for maintenance and/or improvement of physical fitness components and QoL, the aim of this study was to evaluate the effect of a 24-week strength training protocol with and without unstable surfaces on the strength, flexibility and QoL in older adults.
Methods
Participants
Fifty-eight community-dwelling older women voluntarily participated in the study. Participants were eligible if they met the following criteria: 1) no severe functional limitation (e.g., several osteoarthritis); 2) no previous experience with strength exercises in the last six months; 3) no previous cardiovascular (e.g., ischemic heart disease), neurological (e.g., dementia), and other clinical conditions or signal/symptoms of unstable disease (e.g., angina pectoris) which contraindicate participation in an exercise program. The participants were recruited through local advertising, social media, and personal contact at community centers that offer services for older people. The study conforms with The Code of Ethics of the World Medical Association and it was approved by the local ethics committee of University of Pernambuco (C.A.A.E 35220014.1.0000.5207 – August 21, 2014) and prospectively registered at Brazilian Clinical Trials Platform (protocol number: RBR-7wcmd6) that relates to large, multi-factorial studies. All participants signed an informed consent form prior to baseline assessments.
Flowchart of study timeline.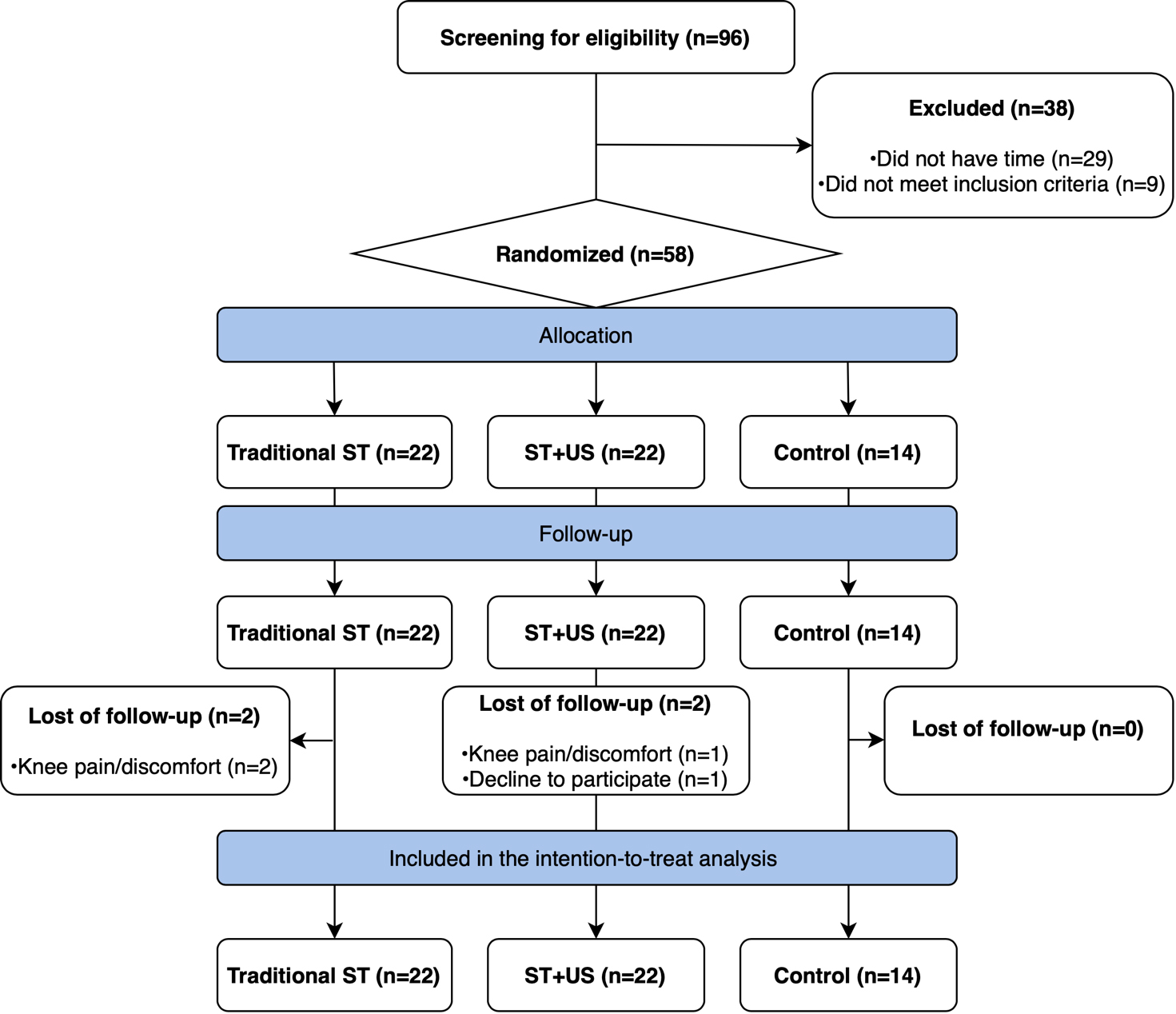
Since no previous studies had identical experimental design the parameters of the two most similar studies for sample size calculation [11, 12] were used along with the GPower 3.1 software. Effect sizes greater than 0.39 were reported for balance and functional outcomes in both studies. Thus, we considered the following parameters: repeated measures with within-between interaction:
Experimental design
This is a secondary analysis from a previous randomized controlled trial designed to examine the effects of strength training with unstable devices in older adults [17]. The study was carried out between May 2016 and March 2017 in Caruaru city, PE, Brazil, and had two enrollment periods for volunteers. First, 36 volunteers were randomly allocated into three groups (ST, ST
Interventions
Participants who were assigned to traditional ST intervention performed moderate-intensity strength exercise, thrice weekly during 24-weeks. Exercise prescription and progression (external resistance adjustments) followed the American College of Sports Medicine (ACSM) recommendations [18] and consisted of whole-body exercises (leg press 45
Description of the strength training program and the instability levels progression.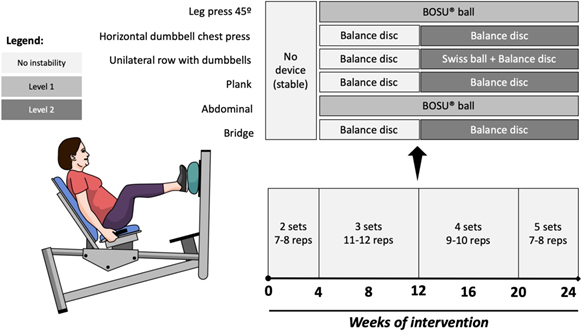
Control group participants did not undergo any type of intervention, but they were encouraged to maintain their daily routine and lifestyle habits. At completion of intervention, a short-version of exercise training program was offered.
We monitored the external resistance progression after 4-, 12- and 24-weeks of intervention in the following exercises: horizontal dumbbell chest press and unilateral row with dumbbell (trunk and upper limbs), and leg press 45
Outcome measures
We used the handgrip test (in both hands), the sit-and-reach test (SRT) and the World Health Organization Quality-of-Life Scale (WHOQOL-BREF) to measure grip strength, flexibility and health-related quality of life, respectively.
The handgrip test was performed using an adjustable and calibrated dynamometer with a digital display (CAMRY, United States) with a scale from 0 to 100 kgf. Participants were evaluated sitting with the shoulder slightly adducted, the elbow flexed at 90
General characteristics of participants
General characteristics of participants
Note: BMI – Body mass index; Values are displayed as mean and standard deviation.
Mean and standard error of the external resistance (in kilograms) after 4-, 12- and 24-weeks of intervention. Note: * Statistically different from baseline assessment (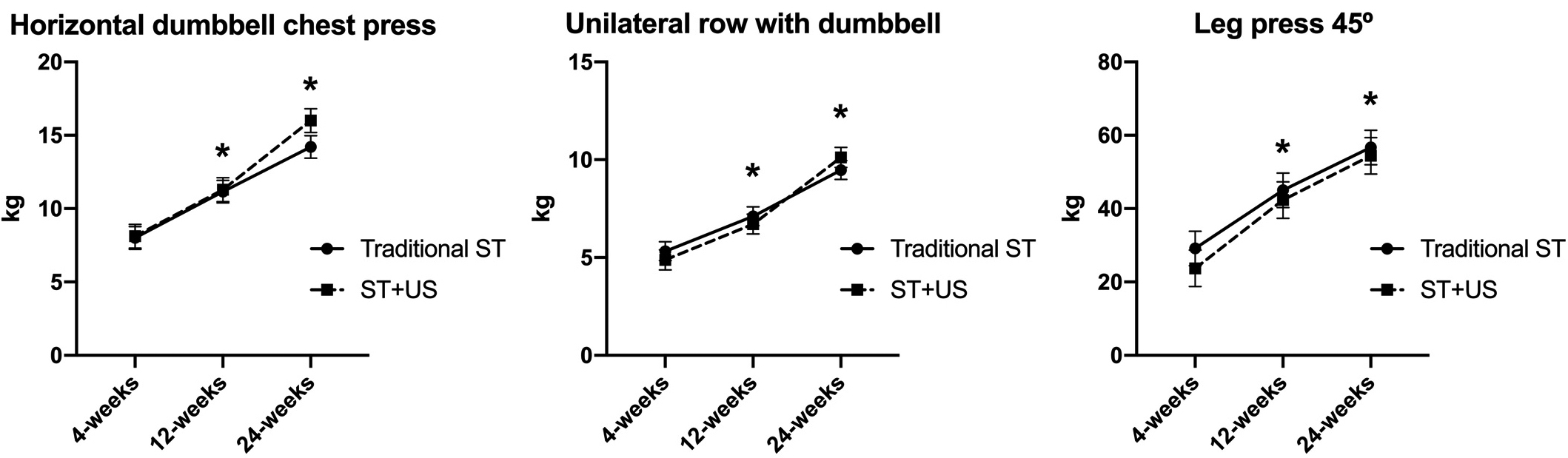
The SRT assesses lumbar and lower limb flexibility [20]. A wooden bench 48 cm long with a tape measure fixed (ruler) on it was used to perform the test. Each subject was positioned sitting on the floor with their legs stretched out straight ahead and feet placed flat against the box, bent forward with their palms facing downwards and sliding over the ruler. Participants performed three attempts and the highest value between them was recorded.
The brief version WHOQOL-BREF questionn-aire [21] was applied in a face-to-face interview. Briefly, WHOQOL-BREF have 26-items encompassing different domains including (overall quality of life – 2 items; physical health – 7 items; psychological health – 6 items; social relationship – 3-items; environmental health – 8 items). Each item of the WHOQOL-BREF is scored from 1 to 5 on a response scale and the total score were computed (higher scores denote higher quality of life).
All statistical procedures were followed the principles of intention-to-treat, such that all randomized participants were included to estimate intervention effects, irrespective of potential deviations from treatment protocol which they were originally assigned (e.g., loss of follow-up, non-compliance).
Firstly, we performed a descriptive analysis and visual inspections (e.g., Q-Q plot, histograms) to check data normality (or lack thereof). Within- and between-group differences and their respective 95% confidence intervals were calculated using linear mixed models by using group, time and group-versus-time interaction terms, as well as the Dunn-Sidak post hoc for multiple comparisons adjustments. The differences were considered statistically significant at
Results
The descriptive characteristics of participants between experimental groups at baseline are shown in Table 1. There were no differences between groups at baseline with respect to demographic and anthropometric characteristics, and dependent variable measures (
A similar improvement was observed regarding the external resistance of trunk and upper limbs, and lower limbs in both exercise groups during all intervention (
Significant within-group changes (24-weeks – baseline) in grip strength were observed for all groups (Right hand: ST:
The ST
Regarding WHOQOL-BREF scores, both exercise groups experienced significant improvements through of 24-weeks, and these gains were superior to the control group at the end of intervention [ ST
Descriptive results (mean
standard deviation) of the effects of 24-weeks of traditional ST and ST+US on grip strength, flexibility and quality of life in older women
Descriptive results (mean
Note: SRT – Sit-and-reach test; WHOQOL – World Health Organization Quality of Life; Values showed as mean and standard deviation. * – represents a statistical difference compared to the baseline; # – Represents difference compared to the control group (
The mean differences within- and between-groups with 95% confidence intervals of the Linear Mixed Models
Our main findings showed that 1) traditional ST and ST
The health-related quality of life might be perceived from subjective and multidimensional aspects (physical well-being, functional capacity, emotional well-being, social well-being) [22]. From this perspective, lifestyle-based therapies such as physical activity and exercise have beneficial effects in several domains of quality of life across the lifespan, including aging [6]. Herein, we demonstrated improvements on overall WHOQOL-BREF score after 24-weeks of traditional ST and ST
Flexibility gains in our study were only demonstrated after ST intervention. A previous systematic review led by Correia et al. [4] showed that older adults undergoing traditional ST programs improved flexibility levels. This finding has implications considering the morphological and functional impact of aging process on muscular, bone and joint components which may lead clinically reductions of range of motion. On the other hand, we did not observe between-group differences on flexibility among individuals allocated to ST
As expected, we found overall muscle strength gains (measured by external resistance) after moderate-intensity ST intervention, which agree with previous studies that investigated the effects of strength training regimes in older adults [13, 27]. We observed that combined strength exercise with unstable devices was also effective to induce similar gains in this outcome. Last but not least, our findings showed grip strength gains in all interventions. This result it is not surprising because although the strength exercise interventions are powerful to improve muscular components in older adults, our exercise-based prescription was not proposed to improve a specific manifestation of strength. We designed an exercise protocol focused on main muscular clusters according to ACSM recommendations.
Although we used a 24-week randomized controlled trial to assess the effects of strength training with and without instability in the elderly, our study has weaknesses and limitations that deserve to be highlighted. Of note, our study sample consisted exclusively of older women living independently in the community who were without significant physical and cognitive impairments or any overt disease. Thus, the current results may not generalize to older men or individuals with significant physical and/or cognitive impairments.
Conclusion
Our findings suggest that traditional strength exercises were effective for improving flexibility and health-related quality of life among healthy older women. Combining unstable devices with traditional exercise did not provided additional gains in order to promote these traits.
Author contributions
CONCEPTION: Rodrigo Cappato de Araújo.
PERFORMANCE OF WORK: André Luiz Torres Pirauá, Valéria Mayaly Alves de Oliveira and Natália Barros Beltrão.
INTERPRETATION OR ANALYSIS OF DATA: André Luiz Torres Pirauá, Valéria Mayaly Alves de Oliveira and Bruno Remígio Cavalcanti.
PREPARATION OF THE MANUSCRIPT: André Luiz Torres Pirauá and Bruno Remígio Cavalcanti.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ana Carolina Rodarti Pitangui and Rodrigo Cappato de Araújo.
SUPERVISION: Rodrigo Cappato de Araújo.
Ethical considerations
The study conforms with The Code of Ethics of the World Medical Association and it was approved by the local ethics committee of University of Pernambuco (C.A.A.E 35220014.1.0000.5207 – August 21, 2014) and prospectively registered at Brazilian Clinical Trials Platform (protocol number: RBR-7wcmd6) that relates to large, multi-factorial studies. All participants signed an informed consent form prior to baseline assessments.
Funding
This study was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq (457585/2014-5) and Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco – FACEPE (APQ-0580-4.08/14).
Footnotes
Acknowledgments
We thank the participants for their contribution to the study. We thank the CNPq and FACEPE for the financial support to carry out this study.
Conflict of interest
The authors declare no conflicts of interest.