
Abstract
We report a longitudinal survey of a 53-year-old man suffering from right knee osteoarthritis who has undergone total knee replacement (TKR). We aimed at evaluating the effect of a short preoperative isokinetic strengthening program on the functional status, pain, and quadriceps and hamstrings strength before and after TKR. The patient performed a 4-week (6 sessions) preoperative isokinetic strengthening program of the quadriceps and hamstrings. The findings for the concentric strength at 60
Introduction
Knee osteoarthritis (OA) is a common degenerative musculoskeletal disease, associated with pain, stiffness, and loss of mobility. It affects 2% to 10% of men and 1.6% to 15% of women over 40 years old depending on the geographical area and definition of pathology [1]. According to a US study, 45% of adults over age 45 will show knee OA before the age of 85 [2].
Currently, there is no effective pharmacological treatment, but non-pharmacological treatments have been found effective [3]. The need for joint replacement surgery is frequent, and 86,000 knee replacements were performed in France in 2011 [4]. The frequency of joint replacement increased more than 33% between 2008 and 2013 [4], which is consistent with data from other knee arthroplasty registries in several Nordic and Anglo-Saxon countries.
In end-stage knee OA, total knee replacement (TKR) is an effective intervention to reduce pain and improve function for many patients. However, after TKR, some patients still experience pain, loss of function, deficient muscle strength or reduced walking speed.
Despite growing development of preoperative exercise programs, most studies show no difference between preoperative intervention and usual care in postoperative pain, function, and muscle strength [5, 6]. A recent (2018) meta-analysis concluded that preoperative training did not benefit functional recovery over the control treatment but that better studies with more patients seemed necessary before a definitive conclusion [7]. Indeed, only 9 randomized controlled trials were included in this meta-analysis, and the sample size of each study was small. Conversely, other studies, some of good quality (level of evidence I) support the interest in a program of preoperative exercises (especially designed to increase lower limb muscle strength) for patients with terminal OA to improve early post-operative results. These programs result in reduced length of hospital stay and faster physical and functional recovery (improved strength, range of motion and functional measures as well as reduced pain) in the early postoperative periods compared with control [8]. None of these studies used exercise programs tailored to patients’ phenotypes.
The great diversity of preoperative exercise protocols, both in terms of the type of exercises (aerobic/specific reinforcement, low/high intensity) and type of muscular reinforcement (isometric/isokinetic), as well as the period of intervention, may explain this great diversity in effect. For example, a meta-analysis suggested that an 8-week exercise period (including muscular strengthening exercise) seemed necessary to improve function and physical activity before TKR [9]. Moreover, it seems important to dissociate the content of these interventions: exercise (aerobic and specific reinforcement), self-management strategies, and associated interventions (occupational therapist, social worker).
We report a longitudinal study of a 53-year-old man with right knee OA who had to undergo TKR after failure of well-conducted medical and conventional physical therapies. His occupation involved significant physical activity but otherwise kept a sedentary lifestyle with few physical activities. This patient had grade 1 obesity (body mass index 30.8 kg/m
Evaluation and strength conditioning
We aimed to evaluate the effect of a short preoperative isokinetic strengthening program on functional status, pain, and muscle strength assessed before and after TKR in this patient. Repeated measures followed the International Classification of Functioning, Disability and Health core assessment set, isokinetic quadriceps concentric strength (60
The patient performed a preoperative isokinetic strengthening program of the quadriceps-hamstrings couple on a Cybex HumacNorm
The TKR involved also tibial tuberosity realignment. The intervention was performed without any complications (Fig. 2B) and allowed for walking without weight-bearing restriction. In view of the tibial tuberosity realignment, postoperative rehabilitation was initially limited because of use of a functional knee brace with knee range of motion restriction from 0
Results
At baseline, active and passive RoM were 0–90
Static lower-limb alignment evaluation with the EOS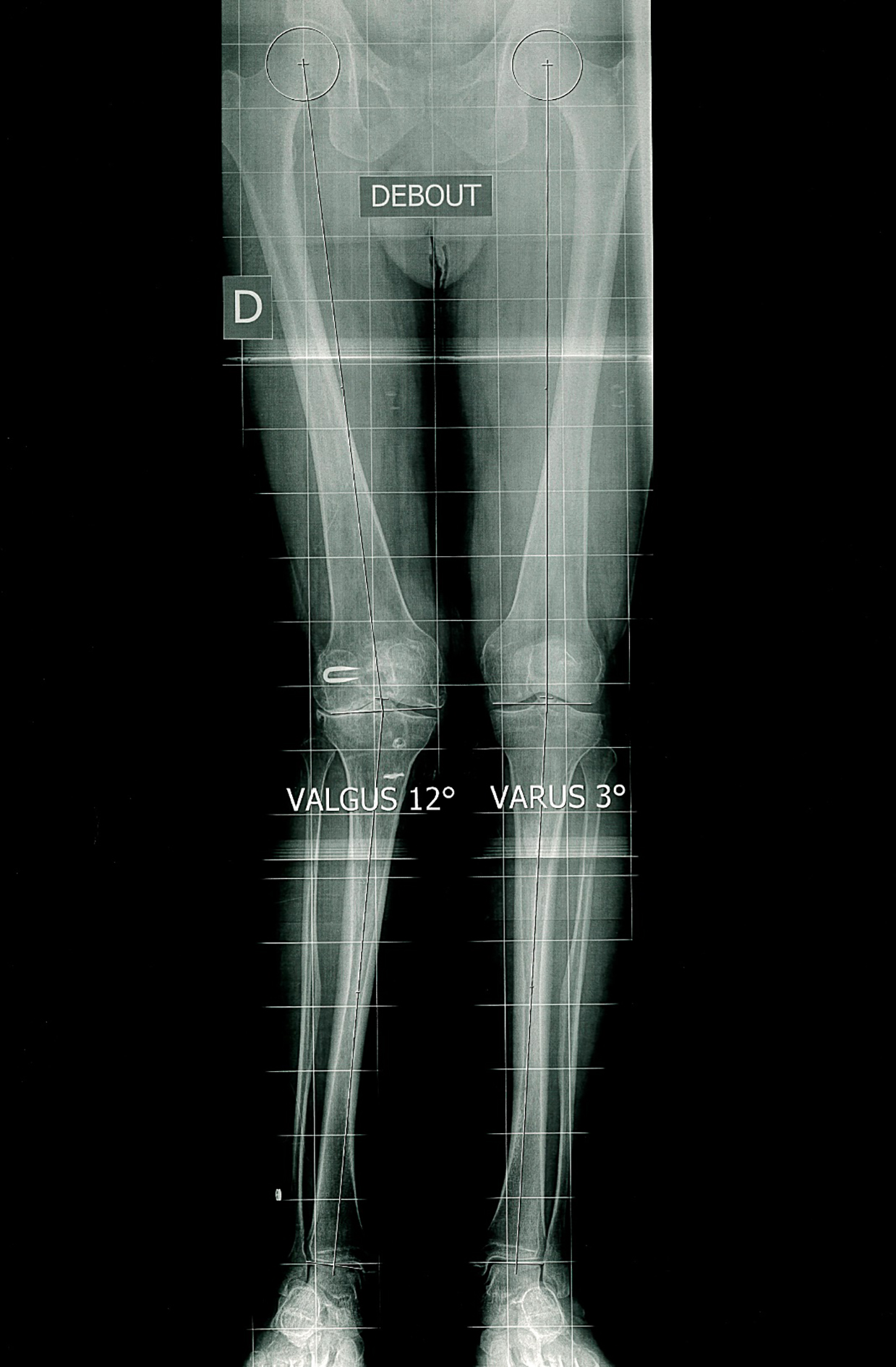
After the strengthening program (but before the intervention) quadriceps strength of the compromised limb (assessed under identically as at baseline) almost doubled (to 121 Nm;
Radiography after total knee replacement (TKR). A. Static lower-limb alignment evaluation with the EOS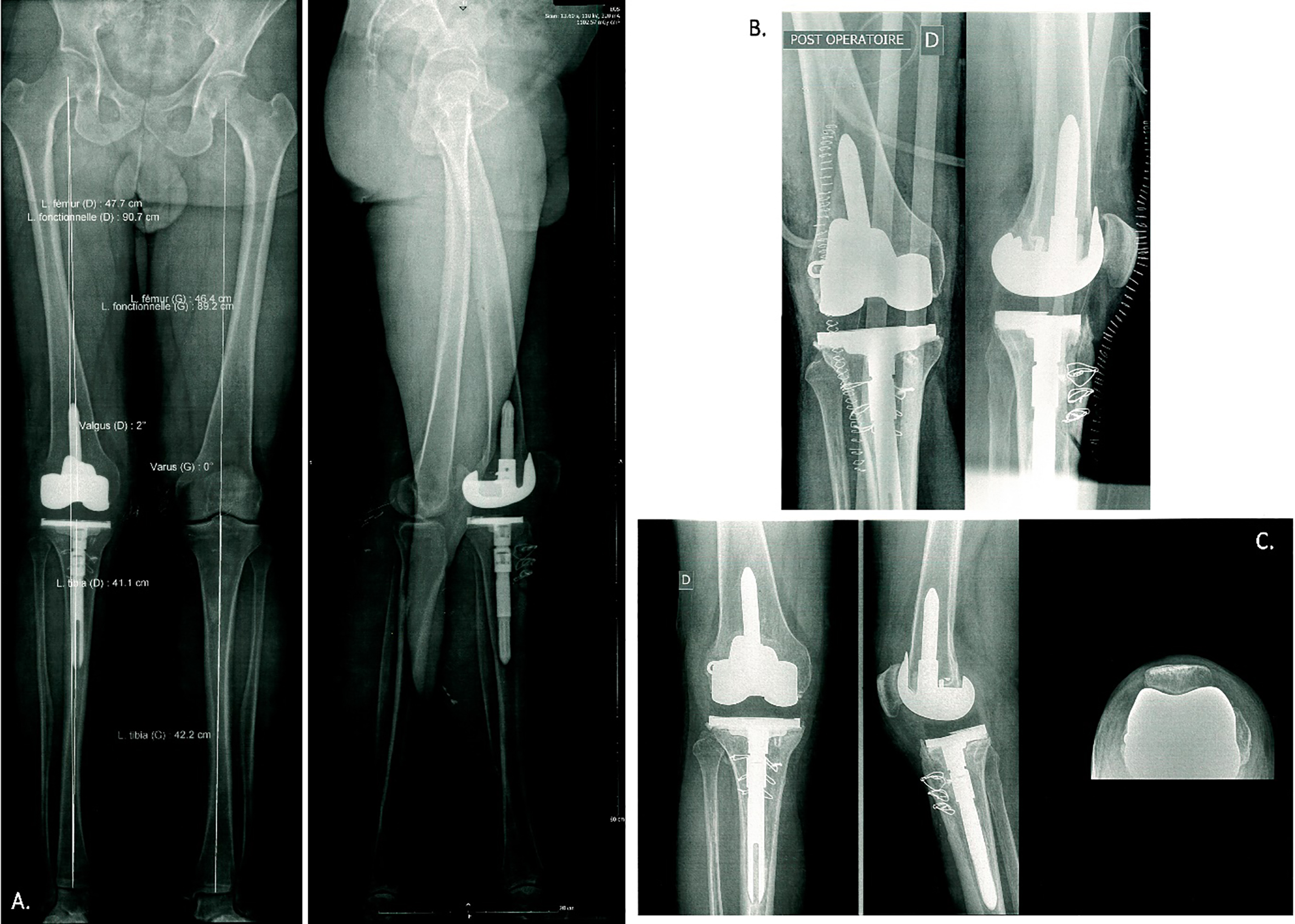
Tested postoperatively at 3, 9 and 17 months, quadriceps strength amounted to 50, 65, and 104 Nm, respectively (versus 178, 171 and 165 Nm for the non-operative limb). On average therefore, knee extension strength deficiency was a significant 57% throughout the follow-up time but significantly stood at 37% at 17 m. Hamstring bilateral values were, at 3, 9 and 17 months, 52, 58 and 62 Nm (operated side) versus 65, 53 and 79 Nm (non-operative limb), Thus, knee flexion deficiency stood on average at 11% and although at 17 m it amounted to 22%, on the whole there was marginal deficiency at worst [11, 12]. The 6MWT was 295, 540, 565 and 575 m at 1, 3, 9 and 17 months, respectively. The KOOS score was 81% (80.6% pain and 91.2% function) at 3 months, 83.9% (83.3% pain, 91.2% function) at 9 months and 85% (83.4% pain, 91.3% function) at 17 months.
Radiography performed 2 months after the TKR revealed a tricompartmental prosthesis in place, no evidence of loosening and satisfactory ossification of the tibial tuberosity (Fig. 2C). Static lower-limb alignment evaluation performed with the EOS
Despite substantial persistent amyotrophy of approximately 4 cm (with thigh perimeter at 49, 50 and 52 cm on the right limb against 51, 57 and 58 cm on the left at 5, 10 and 15 cm above-patellar respectively), the patient was very satisfied with the care that allowed for walking “without any restriction” and a “faster walking speed”, measured with the GAITRite
Quadriceps isokinetic strength was improved after a short preoperative isokinetic strengthening program, but postoperative quadriceps strength deficit remained despite pain and functional improvements. Preoperatively, this patient underwent quite an intensive strength enhancement program using isokinetic dynamometer and so it is not surprising to find a strength improvement in the same measurement modality. However, function and pain were not related to this improvement according to the KOOS score. A possible explanation could be that the main postoperative objective was on function rather than on quadriceps strengthening. Thus, the extent to which quadriceps strength enhancement is transferrable to functional or pain improvements is still open, a point raised by Husby et al. in their study [13]. On the other hand, hamstrings isokinetic strength was practically normalized concordant with literature showing predominant quadriceps deficit in OA and post TKR patient [14]. In this particular case, tibial tuberosity realignment could explain the more pronounced deficiency in quadriceps.
The fact that the functional status and the isokinetic strength are not related is not obvious, especially as both are frequently considered to be closely complementary constructs. Further, several randomized control trials or clinical control trials used isokinetic muscle strength as a primary criterion for assessing the efficacy of rehabilitation outcomes in TKR [12, 15]. Our case deviates from this schema possibly due to of the lack of post-operative quadriceps strengthening. This observation is consistent with Cavanellas et al. study who have indicated that traditional rehabilitation programs were not sufficient in terms of quadriceps strength restoration [14].
This case report suggests the potential interest of focusing on functional evaluation rather than maximal strength to assess the effectiveness of TKR. However, it should be emphasized that without an adequate level of strength, good functioning may not be possible. Moreover, in situations where the integrity of the knee is threatened (e.g. perturbations) quadriceps strength and the speed with which it may be recruited, could be crucial.
Thus, further studies are needed to determine the significance of attaining maximal strength (which in fact relates to the strength level of the sound side) and to the impact of such deficit. The usefulness of a pre- and post-operative isokinetic strengthening program remains undetermined but could be of interest in preparing younger individuals with knee OA with high expectations regarding functional improvement after TKR.
Author contributions
CONCEPTION: Vivien Reynaud, Lech Dobija and Emmanuel Coudeyre.
PERFORMANCE OF WORK: Vivien Reynaud, Lech Dobija, Pierre-Louis Fournier and Charlotte Lanhers.
INTERPRETATION OR ANALYSIS OF DATA: Vivien Reynaud, Lech Dobija and Charlotte Lanhers.
PREPARATION OF THE MANUSCRIPT: Vivien Reynaud and Lech Dobija.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Vivien Reynaud, Lech Dobija and Charlotte Lanhers.
SUPERVISION: Emmanuel Coudeyre.
Ethical considerations
Because patients’ data were retrospectively retrieved for the purpose of the present study, a formal approval by an institutional review board is not required according to the Jardé Law of March 5, 2012 and its application decree (No. 2016-1537) relating to research involving the human person in France. We still proceeded to a reinforced information with explanatory mail and form to the patient and retrieved his signature of an information and non-opposition form.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors sincerely thank the patient who gave written consent for this case report.
Conflict of interest
None declared.