
Abstract
Purpose
To evaluate clinical outcomes between hybrid closed wedge high tibial osteotomy (HCWHTO) and total knee arthroplasty (TKA) for advanced medial compartmental osteoarthritis of the knee (advanced knee OA).
Methods
In more than grade 3 OA based on the Kellgren-Lawrence classification, when patients’ age was less than 60 years or activity level was more than level 5 based on the UCLA activity score, 22 knees (18 patients) underwent HCWHTO. The other 22 knees (18 patients) that underwent TKA were evaluated retrospectively. Muscle strength was evaluated preoperatively and at 1 year postoperatively. The visual analogue scale (VAS) and Japanese version of the Knee injury and Osteoarthritis Outcome Score (J-KOOS) were used to evaluate clinical outcomes preoperatively and at a mean 66-months follow-up.
Results
All postoperative muscle strength measures improved to preoperative equivalent levels in the HCWHTO group; they were significantly higher in the HCWHTO group than in the TKA group (p < .05). The VAS score and total J-KOOS significantly improved in both groups (HCWHTO, p = .001; TKA, p = .040); there were no significant differences in the scores between the groups at the final follow-up. Hybrid closed wedge HTO significantly improved the activities of daily living and sport/recreation scores, whereas TKA did not at the final follow-up.
Conclusions
In advanced knee OA, HCWHTO led to improved muscle strength, and its midterm clinical outcomes were equivalent to those of TKA. To postpone or even to avoid TKA, HCWHTO is considered an appropriate treatment for young and high-activity patients with advanced knee OA.
Level of Evidence
Therapeutic Level III
Introduction
High tibial osteotomy (HTO) is an effective treatment for medial compartmental osteoarthritis (OA) of the knee with good clinical results in young and middle-aged patients.1,2,3 However, there has been no consensus as to which level of OA severity can be treated with HTO.4,5 Regarding the types of HTO suitable for advanced OA of the knee, hybrid closed wedge high tibial osteotomy (HCWHTO) is a more effective treatment than open wedge HTO because HCWHTO can improve not only medial compartmental OA but also patellofemoral joint congruity through closed wedge osteotomy.1,6,7,8 Therefore, HCWHTO may be indicated in patients who have advanced OA.
Total knee arthroplasty (TKA), a surgical procedure for advanced OA, is also considered a good option for low-demand patients older than 60 years of age, with reportedly good long-term outcomes.9,10 In a comparative study between HTO and TKA in patients above 60 years of age, there was no significant difference in clinical scores at the 1-year follow-up 11 . However, TKA has several limitations in young patients, such as polyethylene wear, aseptic loosening, and a lower survival rate.12,13 Therefore, HCWHTO may be indicated in young patients who have advanced OA and a high activity level to avoid these aforementioned limitations caused by TKA. However, there are currently no reports in the literature comparing the clinical results of HCWHTO and TKA, although it is important to select patients who meet optimal surgical indications to achieve satisfactory results.
The present study aimed to evaluate the clinical outcomes between HCWHTO and TKA for advanced OA of the knee at a mid-term follow-up. We hypothesized that the outcomes for the two techniques are different because HCWHTO improves postoperative clinical results despite advanced OA of the knee.
Materials and methods
Patients
This retrospective study evaluated patients who underwent HCWHTO and TKA in our hospital between May 2011 and July 2013. The inclusion criteria were more than grade 3 medial compartment OA of the knee based on the Kellgren-Lawrence classification, varus alignment, no inflammatory arthritis, and follow-up of at least 5 years. During the study period, HCWHTO and TKA were performed for 58 knees in 51 consecutive patients with medial compartment OA of the knee and varus knee deformities. The exclusion criteria included follow-up of fewer than 5 years, history of surgical procedure of the ipsilateral knee, or absent outcome scores including the visual analog scale (VAS) and the Japanese version of the Knee injury and Osteoarthritis Outcome Score (J-KOOS). 14 Nine knees with less than 5 years of follow-up, two knees with previous ipsilateral open wedge HTO or internal fixation of the femur, and three knees with incomplete outcome scores were excluded. Therefore, 44 knees in 40 patients comprised the final study population. Based on the UCLA activity score, 15 HCWHTO was selected when the patients’ activity level was more than level 5, or when they were less than 60 years of age; TKA was indicated when the patients’ activity level was less than level 4, they were aged greater than 60 years. There was no ligament instability in patients who underwent HCWHTO.
Regarding the preoperative range of motion (ROM), the mean extension ROM was −3.6° ± 4.1° (range: −15.0 to 0) in the HCWHTO group and −7.5° ± 7.2° (range: −25.0 to 0.0) in the TKA group. The mean flexion ROM was 135.9° ± 10.4° (range: 110.0–145.0) in the HCWHTO group and 117.0° ± 17.3° (range: 90.0–140.0) in the TKA group.
This study was approved by our institutional review board (30–3), and all patients provided informed consent for participation in the study.
Surgical techniques and postoperative rehabilitation
Hybrid closed wedge high tibial osteotomy was performed according to the method described by Takeuchi et al.
8
Before tibial osteotomy, fibular osteotomy at the mid-portion and segmental resection were performed. Biplanar osteotomy of the tibia was performed. Then the hinge point that divided the proximal tibial osteotomy line by about 2 to 1 was determined. After removing the lateral closed wedge bone block, the medial side was opened, and the lateral side was closed. A proximal-lateral tibial plate (five distal screw holes; Synthes, Solothurn, Switzerland) was inserted into a subcutaneous tunnel formed on the lateral side of the tibia after bending the plate so the proximal screws would be parallel to the tibial plateau and fixed in place with eight locking screws with minimal invasiveness (Figure 1(a) to (d)).
8
Medial compartment osteoarthritis of the right knee (a, b, c, d). (a) Anteroposterior radiograph before hybrid closed wedge high tibial osteotomy (HCWHTO). (b) Anteroposterior radiograph after HCWHTO. (c) Lateral view before HCWHTO. (d) Lateral view after HCWHTO. Medial compartment osteoarthritis of the left knee (e, f, g, h). (e) Anteroposterior radiograph before total knee arthroplasty (TKA). (f) Anteroposterior radiograph after TKA. (g) Lateral view before TKA. (h) Lateral view after TKA.
On the day after HCWHTO, active and passive ROM exercises and isotonic muscle-strengthening were started. Standing exercises were initiated as soon as possible. At 1 week after surgery, patients were permitted to begin partial weight-bearing walking depending on their pain with walker equipment, and at 2 weeks postoperatively, full weight-bearing walking was started.
In TKA, the Vanguard knee system (Zimmer-Biomet, Warsaw, IN) was used. A midline knee incision was followed by the midvastus approach. Preparation of the femur was accomplished first, followed by tibial preparation. The measured resection technique was performed intraoperatively and confirmed to obtain proper balance. The femoral and tibial components were fixed using a cruciate-retaining type in all knees; bone cement was used in 15 of 22 patients (68.2%), and the patellae were resurfaced in 14 patients (63.6%) (Figure 1(e) to (h)).
On the day after TKA, active and passive ROM exercises and isotonic muscle-strengthening were started similar to those after HCWHTO. Standing exercises were initiated as soon as possible. At 3 days after surgery, patients were permitted to begin full weight-bearing walking depending on their pain with walker equipment.
Radiological and clinical evaluation
The degree of OA was evaluated using the Kellgren-Lawrence classification. The following data were measured using digital software (Plissimo; Konica, Tokyo, Japan). Using an anteroposterior weight-bearing whole-leg radiograph with the knee joint in extension, the hip-knee-ankle angle (HKA; defined as the angle between the femoral mechanical axis and the tibial mechanical axis) and weight-bearing line ratio (WBL ratio; calculated as the horizontal distance from the WBL to the medial edge of the tibial plateau (d), divided by the width of the tibial plateau (W); d/W × 100%) were calculated (Figure 2(a) and (b)). Radiographic assessments. (a) Hip-knee-ankle angle. (b) Weight-bearing line ratio.
The VAS and J-KOOS were used to evaluate the clinical outcomes preoperatively and at a mean 66-months follow-up. The maximum J-KOOS is 168 points. 14
Lower-extremity muscle strength measures, including knee extension, knee flexion, plantarflexion, and dorsiflexion, were calculated preoperatively and at 1 year after the procedure using a handheld dynamometer (HHD; μTas F-1; Anima Inc., Tokyo, Japan) with a fixed belt (Figure 3(a) to (d)).
16
During the measurements, maximum isometric strength was then evaluated, and the sensor pad was supported lightly to prevent the HHD from shifting. The lower-extremity muscle strength after HCWHTO and TKA were measured by a dedicated physical therapist. Measurement of lower-extremity muscle strength using a handheld dynamometer (HHD: arrow) with a fixed belt. The participant is positioned in the sitting position on the stretcher (a and b). (a) Knee extension (the HHD is placed on the front of the ankle of the evaluated limb). (b) Knee flexion (the HHD is positioned behind the heel of the evaluated limb). The participant is positioned in the supine position on the stretcher (c and d). (c) Plantarflexion (the HHD is positioned between the forefoot and the board installed vertically on the stretcher). (d) Dorsiflexion (the HHD is positioned on the dorsum pedis).
Statistical analysis
The radiographic parameters for HCWHTO and TKA were measured by two authors who were blinded to the clinical results. The same observers reviewed the radiographs three times for each subject on different days, and the mean values were calculated. Intraobserver and interobserver reliabilities were assessed by calculating the intraclass correlation coefficients (ICCs) using a two-way mixed model for each parameter. Data for patients with HCWHTO and TKA were evaluated separately. Lower-extremity muscle strength measures were measured three times for each muscle, and the mean values were calculated. The preoperative and final follow-up values of the radiographic parameters, ROM, muscle strength, J-KOOS, and VAS were compared by a paired t-test. Differences among the demographic parameters were analysed by the Mann–Whitney U test, and those among categorical variables were analysed by the chi-square test. The differences in radiographic parameters and muscle strength between patients with HCWHTO and TKA were analyzed for normal distribution using the Student’s t-test. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). Statistical significance was assumed for p-values less than .05.
A power analysis was performed for the primary comparison of interest (postoperative lower-extremity muscle strength including knee extension, knee flexion, plantarflexion, and dorsiflexion between HCWHTO and TKA). The power analysis revealed that a total sample size of n = 44 for the study was sufficient to detect a minimum effect size (d) of 0.87 at a power of 0.80 and an α-error of 5%, based on G power software (version 3.1.9.4).
Results
Demographic parameters of hybrid closed wedge high tibial osteotomy and total knee arthroplasty.
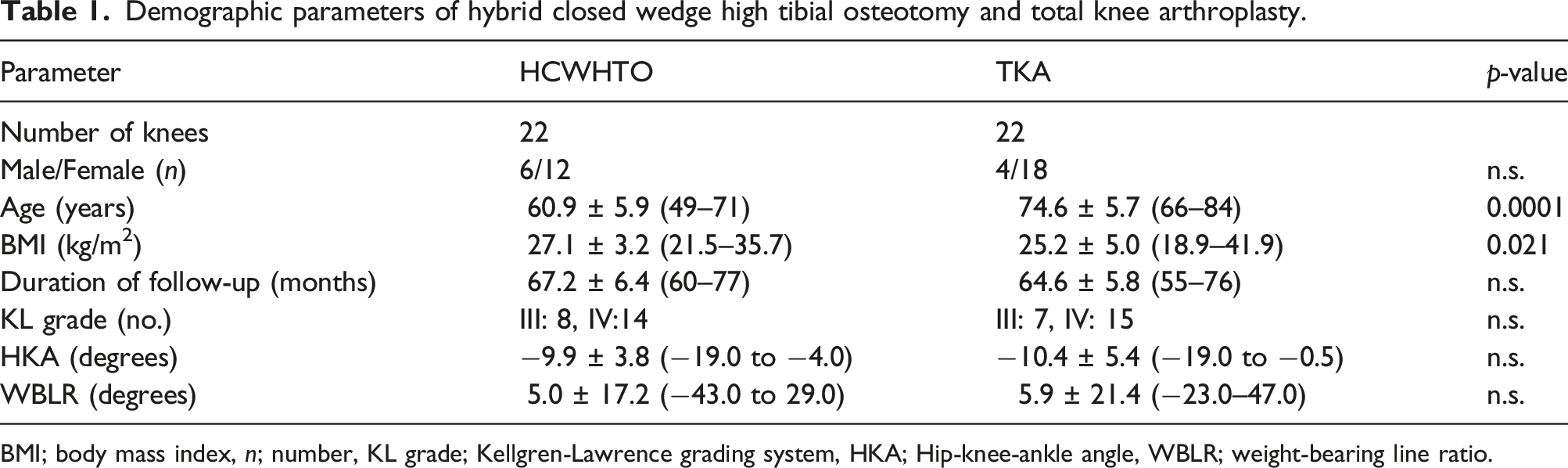
BMI; body mass index, n; number, KL grade; Kellgren-Lawrence grading system, HKA; Hip-knee-ankle angle, WBLR; weight-bearing line ratio.
Pre- and Postoperative range of mortion and muscles strength of hybrid closed wedge high tibial osteotomy and total knee arthroplasty.

ROM; range of motion.
aSignificant difference between HCWHTO and TKA.
For repeated measurements of the HKA and WBL ratio, the intraobserver ICCs were 0.968 and 0.921, and the interobserver ICCs were 0.927 and 0.866, respectively. These ICCs indicated high intraobserver and interobserver reliabilities.
Regarding lower-extremity muscle strength, TKA significantly improved knee extension, knee flexion, and plantarflexion (p = .003, p = .034, and p = .003, respectively). In contrast, HCWHTO did not change these parameters significantly after the procedure (p = n.s., n.s., and n.s., respectively). All the muscle strength measures were significantly higher in the HCWHTO group than in the TKA group before and after the procedure (knee extension: p = .0001, p = .0001; knee flexion: p = .0001, p = .0001; plantarflexion: p = .001, p = .0001; and dorsiflexion: p = .0001, p = .008, respectively) (Table 2).
Change in clinical parameters with hybrid closed wedge high tibial osteotomy and total knee arthroplasty.

There are no significant differences between HCWHTO and TKA.
VAS; Visual analog scale, J-KOOS; Japanese version of the Knee injury and Osteoarthritis Outcome Score, QOL; Quality of life.
Discussion
The main findings of the present study is that the clinical outcomes such as the VAS score and J-KOOS between HCWHTO and TKA were equivalent at the minimum 5-years follow-up.
In 2002, Machner et al. concluded that quadriceps muscle strength was significantly lower than the preoperative values at 1-year follow-up after CWHTO. 17 However, the rehabilitation plan of this study was relatively slow because a locking plate was not used. Although the recovery of lower-extremity muscle strength after CWHTO is an essential data point for patients considering CWHTO, the postoperative lower-extremity muscle strength after HCWHTO, based on an early rehabilitation plan with a locking plate, remains unknown. In our study, all lower-extremity muscle strength measures in HCWHTO improved to the preoperative equivalent levels using this early rehabilitation plan and a locking plate. Therefore, even in advanced OA of the knee, young patients with a high activity level who will undergo HCWHTO may have preoperative equivalent activity by recovered lower-extremity muscle strength based on an early rehabilitation plan and use of a locking plate.
Concerning the clinical evaluation, there are many reports on the good clinical outcomes after TKA.18,19 At the mid-term follow-up, Fokin et al. reported that the knee society score and function score were significantly increased at 3 months after surgery and were significantly greater than the preoperative values at 5 years after TKA. 18 In our study, the VAS score and the J-KOOS significantly improved after TKA at a minimum 5-years follow-up compared with preoperative values, similar to findings of a previous study. There are several reports on the good clinical outcomes after CWHTO at mid- and long-term follow-ups.1,3,20 In the present study, the clinical outcomes of HCWHTO were equivalent to those of TKA at the minimum 5-years follow-up, although patients had grade 3 or 4 OA based on the Kellgren–Lawrence classification. Therefore, if patients less than 60 years of age with a high activity level have advanced OA of the knee, HCWHTO may indicate the need to postpone TKA in these patients.
In the present study, only the HCWHTO group showed significantly improved ADL and sport/recreation scores of the J-KOOS postoperatively. Concerning postoperative return to sports, Ekhtiari et al. reported that 90.8% of patients who underwent HTO resumed their sports participation, and 78.6% of them could return to the same or a higher level. 12 In contrast, in a review of TKA, Witjes et al. found that 36–89% of patients could return to sports after TKA, and 87% of these patients were engaged in low-impact sports. 21 Furthermore, high-impact sports were performed more often after HTO than after TKA. 22 Therefore, HTO seems to be more effective than TKA for return to sports. The improvement of the ADL and sport/recreation scores of the J-KOOS after HCWHTO may support the findings of previous studies.12,22
Regarding the cost-effectiveness of surgical procedures for medial compartmental OA of the knee, several reports had indicated that HTO may be the most cost-effective surgical procedure in patients younger than 60 years of age compared with both TKA and unicompartmental knee arthroplasty.23,24 Furthermore, although the cost-effectiveness of HTO depends on the rates of conversion to TKA, HTO can be effectively postponed or even used to avoid TKA, with the rate of conversion within 10 years of 16%.23,25 Therefore, HTO may be the first choice for patients younger than 60 years of age despite even advanced OA of the knee.
The present study has several limitations. First, the sample size of patients was relatively small, although the post hoc power analysis showed it to be sufficient to detect a minimum effect. Second, regarding the preoperative demographic parameters, the HCWHTO group included young patients, and the BMI of the patients was high compared to that of the TKA group. These two factors may have affected the improvement in the ADL and sport/recreation scores of the J-KOOS. In addition, this study has a design bias, because more active patients were selected for HCWHTO based on our criteria. To avoid bias, studies using matched groups to compare HTO and TKA, with mid-to long-term follow-up durations, are needed. Third, lower-extremity muscle strength measures were not evaluated at the final follow-up. To confirm the change of lower-extremity muscle strength measures, long-term follow-up studies are needed.
Conclusion
In advanced OA of the knee, HCWHTO led to improved lower-extremity muscle strength to the preoperative equivalent levels, and its mid-term clinical outcomes were equivalent to those of TKA. If patients with advanced OA of the knee are young and have a high activity level, HCWHTO is an appropriate treatment for postponing TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.