
Abstract
BACKGROUND:
During one-leg standing (OLS), optimum activity of the gluteus medius (Gmed), multifidus (MF), and quadratus lumborum (QL) muscles relies upon maintaining neutral lumbopelvic alignment. However, no studies have examined how using pressure biofeedback during OLS affects the activity of these muscles and the concomitant alignment of the pelvis and trunk.
OBJECTIVES:
The purpose of this study was to investigate the effect of pressure biofeedback on the activity of the Gmed, MF, and QL and the femoropelvic and trunk lean angles during OLS.
METHODS:
Twenty-four healthy males performed OLS with (PB
RESULTS:
The activity of the Gmed, MF, and QL was greater under both PB
CONCLUSIONS:
These results suggest that pressure biofeedback is a useful modality for increasing the activity of the Gmed and trunk muscles, especially the MF muscle on the non-supporting leg side, and for preventing compensatory movements such as trunk deviation and pelvic lateral deviation during OLS.
Introduction
One-leg standing (OLS) requires balancing while standing on one leg [1]. It is not only used to assess postural stability and movement bias [2, 3], but also as a gluteus medius (Gmed) strengthening exercise [4]. The Gmed stabilizes the pelvis against the fixed femur during OLS [5, 6], producing a force equal to double the body weight to maintain the correct pelvic and trunk posture [6], and produces the greatest moment for its muscle length to meet functional needs such as OLS [6]. Lumbopelvic neutral alignment is required during OLS to increase Gmed activity because Gmed activity is affected by lumbopelvic alignment [7]. Lumbopelvic neutral alignment is maintained by the co-contraction of local and global muscles, including the multifidus (MF), which helps maintain an upright posture and regulates load transfer through the pelvis prior to movement [8, 9]. In addition, the quadratus lumborum (QL) plays an important role as a lumbar stabilizer [10, 11], and the bilateral activity of both QL muscles may control load transfer by ensuring pelvic stability.
During OLS, lateral pelvic deviations occur to maintain the center of mass on the supporting leg [12]. Because the pelvis and lumbar spine are connected by a kinematic link [6, 13], trunk deviation to the supported or unsupported side may occur during OLS.
A previous study reported that the activity of the Gmed was significantly lower when the pelvis was dropped or the trunk was deviated toward the support side [14, 15]. Elevation of the pelvis during OLS increases activation of the ipsilateral QL muscle. In addition, the MF maintains a neutral position to improve lumbopelvic stability [16], and its activation may be reduced if the trunk or pelvic alignment changes. Repeated performance of OLS without control of lumbopelvic alignment is related to musculoskeletal disorders in the low back or pelvis [9, 17]. Therefore, to increase the activity of the Gmed, MF, and QL during OLS, a method that can minimize lateral deviation of the pelvis is needed.
Biofeedback has been used as an effective method to induce correct postural alignment and improve muscle activity by providing real-time information on pressure at the contact site during exercise [18, 19]. Cynn et al. [18] reported that pressure biofeedback between the ground and lumbar side during side-lying hip abduction significantly decreased pelvic lateral tilt angle and muscle activity of the QL and significantly increased the activity of the Gmed. In another report, pressure biofeedback between the ground and abdominals during prone hip extension decreased the activity of the erector muscles and the angle of pelvic anterior tilt while simultaneously increasing gluteus maximus and hamstring activity [19].
Based on these previous findings, we believe that pressure biofeedback can be used for increasing the activity of the Gmed and correct the alignment of the pelvis and trunk during OLS. However, no studies have investigated how pressure-induced biofeedback affects pelvic and trunk alignment and muscle activity of the Gmed and trunk muscles during OLS. In addition, deviation of the pelvis and trunk during OLS occur together, but previous studies have investigated changes in Gmed activity by experimentally controlling pelvic deviation and trunk deviation separately [14, 15]. Thus, it is still necessary to identify changes in Gmed muscle activity together with changes in trunk and pelvic alignment caused by different OLS strategies.
Therefore, the aim of the present study was to investigate the effects of pressure biofeedback on pelvic and trunk alignment as well as Gmed, MF, and QL activity during OLS. We hypothesized that pressure biofeedback would reduce pelvic and trunk deviation and increase the activity of the Gmed, MF, and QL during OLS.
Methods
Participants
Twenty-four healthy male volunteers with right leg dominance (age, 32.46
One-leg standing with and without pressure biofeedback. (A) Preferred one-leg standing without pressure biofeedback. (B) One-leg standing with pressure biofeedback. (C) Real-time pressure change display during one-leg standing.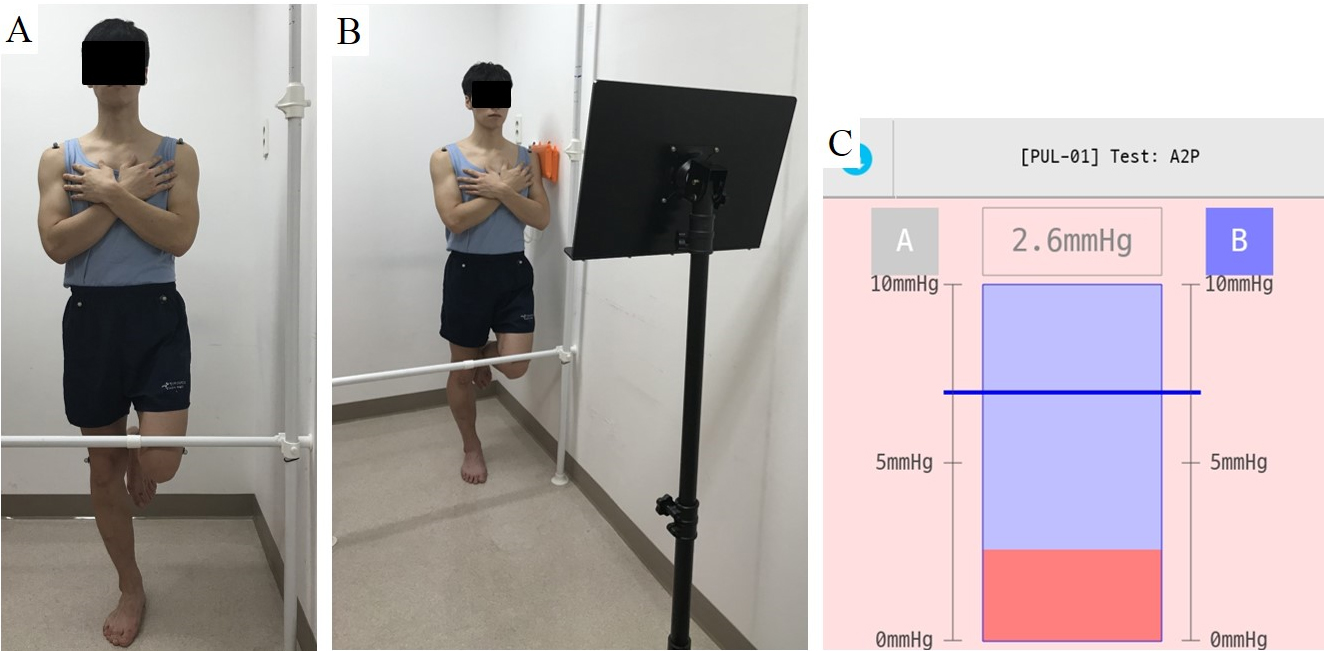
The sample size was determined using the statistical package G*Power 3 based on previous findings [14]. The results of the power analysis showed that at least 22 participants would be required for a power of 0.80 at an
Prior to the experiment, all participants completed a questionnaire relating to demographic parameters. The examiners then measured lumbopelvic alignment and activity of the Gmed, MF, and QL under all OLS conditions with OLS performed at 30
One-leg standing
Prior to performing the experiment, each participant practiced the OLS conditions under the supervision of examiner 1 for 10 min. All participants performed the following three OLS conditions: (1) without pressure biofeedback (PB
To perform under the PB
Before performing under the other PB conditions, a 4D-MT pressure sensor (ReLive, Seoul, Korea) was placed between the lateral surface of left (non-supporting) humerus and the wall with participants standing with their non-supported side next to the wall. The pressure sensor consisted of a cuff and device that receives pressure information. The pressure information was transferred in real-time via Bluetooth to the 4D-MT pressure analysis program (ReLive) on an android tablet PC. Real-time pressure changes were displayed on the tablet PC screen. Calibration was performed by placing the lateral surface of the humerus on the pressure sensor. We performed a pilot test with five subjects to determine the pressure threshold value for PB
Data collection was discontinued if the position of the pressure sensor on the wall changed or the pressure sensor could not be maintained between the humerus and the wall due to postural sway with increased thoracic kyphosis, increased lumbar lordosis or kyphosis, trunk rotation, or knee flexion of the supporting leg. OLS posture was maintained for 5 seconds during each of the three conditions, which, in turn, were repeated three times. Each participant had a 30-s rest time between trials and a 20-min rest time between exercises to prevent muscle fatigue and learning effects.
Pelvic and trunk alignment
The femoropelvic angle and trunk lean angle were measured to analyze trunk alignment during all three OLS conditions [20]. Markers were attached bilaterally to the acromion processes, anterior superior iliac spines (ASIS), and femoral condyles, and a digital camera attached to a tripod was placed 2.5 m from the participants at the height of the ASIS. The femoropelvic angle was calculated as the angle between the line connecting the two ASISs and the line joining the ASIS and lateral femur of the supporting leg. A smaller femoropelvic angle indicates increased pelvic lateral deviation to the supporting leg side or increased hip adduction on the supporting leg side. The trunk lean angle was measured as the angle between the line connecting the midpoint of the two ASISs and the midpoint of both acromion processes and a vertical line (Fig. 2). Greater trunk lean angle indicates lateral trunk lean to the non-supporting leg side relative to the pelvis. The photographic images captured by the digital camera were transferred to a personal notebook and analyzed using ImageJ software (ImageJ 1.44, NIH). The mean of three measurements was used for statistical analyses.
Hip and trunk muscles activation
Wireless TeleMyo DTS (Noraxon, Inc., Scottsdale, AZ, USA) and Myo-Research Master Edition 1.06 XP software were used to collect electromyographic (EMG) data for the Gmed and trunk muscles. This device is an eight-channel portable microcomputer with an eight-channel A/D conversion (12-bit resolution). Before placing the electrodes, the attachment sites were shaved and cleaned using rubbing alcohol to minimize skin impedance. The surface electrode pairs (AG/AGCl) had a pre-gelled diameter of 10 mm, and the inter-electrode distance was 2 cm. First, the electrode on the right Gmed was attached on the proximal side one-third of the distance between the iliac crest and greater trochanter. Then, the electrodes on both QL muscles were attached approximately 4 cm lateral from the muscle belly of the erector spinae, at the mid-point between the iliac crest and 12th rib [21]. Finally, the electrodes on both MF muscles were attached above and below and aligned transversely to the posterior superior iliac spines [22], parallel to the direction of the muscle fibers in the middle of the muscle belly. The raw EMG signals were sampled at 1,000 Hz and calculated using the root mean square (RMS) with a 50-ms interval. A band pass filter of 20–450 Hz and notch filter at 60 Hz were also used.
Measures of femoropelvic angle (A) and trunk lean angle (B).
Normalization of EMG data was performed using a maximal voluntary isometric contraction (MVIC) for 5 s. The Gmed was tested in the side-lying position with the examiner providing manual resistance at the ankle while the participant abducted his hip. The QL was also tested in the same position. When participants elevated the pelvis and ribs off the floor in trunk lateral flexion, the examiner applied manual resistance to the hip and pelvis [23]. The MF was tested in the prone position with the leg strapped to the table. The examiner applied manual resistance to the posterior scapula while the participant extended the trunk. All EMG data were measured for 5 s, and the first and last 1 s were excluded from the analysis. The MVIC was performed three times; participants were given a 3-min rest between trials.
All EMG data are expressed as percentage of MVIC (%MVIC). For each OLS condition, the EMG data for the Gmed and trunk muscles were measured three times for 5 s each, and the first and last 1 s were excluded from the analysis.
Activity of the gluteus medius and trunk muscles under three one-leg standing conditions
Effect size of the muscle activity between conditions
Abbreviations: Gmed, gluteus medius; MF, multifidus; OLS, one-leg standing; PB
All data are presented as mean
Results
The Kolmogorov-Smirnov test indicated normal distribution in all outcome variables. The muscle activity data and femoropelvic and trunk lean angles are shown in Tables 1 and 2.
The activity of the right Gmed, bilateral QL, and bilateral MF muscles was significantly higher under both PB
Lumbopelvic alignment angles during the three one-leg standing conditions
Lumbopelvic alignment angles during the three one-leg standing conditions
There was a significant difference in both the femoropelvic and trunk lean angles between the OLS conditions with and without pressure biofeedback (Table 3). Compared to the PB
The present study showed that pressure biofeedback arising from an interface between the lateral arm on the non-supporting leg side and a wall during OLS led to increased activity of the Gmed on the supporting leg side and the bilateral MF and QL muscles, together with an increase in femoropelvic angle on the supporting leg side and decrease in trunk lean angle to the non-supporting leg side compared to OLS without pressure biofeedback.
Our findings show that Gmed, MF, and QL activity were significantly greater under both PB
Load transfer occurs during OLS and is controlled by the co-activation of local and global muscles [8]. The self-bracing mechanism is generated by activation of the MF in the lumbopelvic neutral position to reduce load transfer [9]. Both PB
Our results demonstrated that the PB
We found no significant differences in muscle activity or lumbopelvic alignment between the PB
There are some limitations in this study. First, because only healthy men participated in this study, the results cannot be generalized to patients with low back pain or lower limb injury, to women, or to elderly people. Second, OLS conditions were performed only on the dominant side. To extend the clinical implications of this study, further studies will need to investigate OLS with biofeedback using both legs. Third, because this study investigated only the immediate effects of pressure biofeedback, no long-term effects are known. Finally, to clarify foot positions/movements and identify their effects on lumbopelvic alignment during OLS tasks, more information (e.g., center of pressure) is needed. In addition, a longer duration for OLS should be considered, as 5 s may be too short for participants to acquire balance during OLS.
Conclusions
We investigated the effects of pressure biofeedback during OLS on the activity of the Gmed and trunk muscles and lumbopelvic alignment. The use of real-time pressure biofeedback during one-leg standing increased the activity of the Gmed, MF, and QL and resulted in a greater femoropelvic angle and lower trunk lean angle compared to one-leg standing without biofeedback. Thus, we recommend using pressure biofeedback during the OLS exercise to increase activity of the Gmed and trunk muscles, especially the MF muscle on the non-supporting leg side, and to prevent trunk deviation and pelvic lateral deviation.
Author contributions
CONCEPTION: Soo-Yong Kim, Il-Young Yu and Min-Hyeok Kang.
PERFORMANCE OF WORK: Soo-Yong Kim, Il-Young Yu and Min-Hyeok Kang.
INTERPRETATION OR ANALYSIS OF DATA: Soo-Yong Kim and Min-Hyeok Kang.
PREPARATION OF THE MANUSCRIPT: Soo-Yong Kim, Il-Young Yu and Min-Hyeok Kang.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Soo-Yong Kim and Min-Hyeok Kang.
SUPERVISION: Min-Hyeok Kang.
Ethical considerations
All participants read and signed an informed consent form approved by the Pusan National University Yangsan Hospital Ethics Committee for Human Investigations (No. 05-2019-042).
Funding
The authors report no funding.
Footnotes
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2018R1C1B5085529).
Conflict of interest
The authors have no conflicts of interest to report.