
Abstract
Background:
Gluteus medius tears are a common cause of lateral hip pain. Operative intervention is usually prescribed for patients with pain despite physical therapy and/or peritrochanteric injections.
Purpose:
To identify clinical features that predict operative intervention in gluteus medius tears.
Study Design:
Case control study; Level of evidence, 3.
Methods:
A matched-pair controlled study was conducted on patients who underwent endoscopic gluteus medius repairs from June 2008 to August 2014 for full-thickness tears. The exclusion criterion was previous hip disorders (eg, Legg-Calve-Perthes disease, avascular necrosis). The control group contained patients with full-thickness gluteus medius tears on magnetic resonance imaging (MRI) who did not require operative intervention. Both groups had a minimum trial of 3 months of nonoperative management. Matching criteria included age within 5 years, sex, and body mass index (BMI) class. The following clinical parameters were analyzed: presence of lateral-sided hip pain, duration of symptoms, power of resisted hip abduction, gait deviation (antalgic or Trendelenburg), greater trochanter tenderness, and hip passive range of abduction.
Results:
Twenty-four patients who underwent isolated endoscopic gluteus medius repairs were identified; all patients were females, with a mean age of 65 years (range, 52-82 years) and mean BMI of 29.2 kg/m2 (range, 21.55-44.398 kg/m2). The matched control cohort contained 12 females treated nonoperatively for gluteus medius tears with mean age of 66 years (range, 52-81 years) and mean BMI of 29.9 kg/m2 (range, 20.20-43.59 kg/m2). There were significant differences between the groups in power of resisted abduction and presence of gait deviation. The operative cohort had a mean power grading of 3.63 (95% CI, 3.28-3.98) compared with 4.58 (95% CI, 4.29-4.87) for the matched cohort (P < .05). Abnormal gait was found in 75% of the operative cohort, compared with 33% of the matched cohort (P < .05). Specifically, 83.3% of the surgical cohort had a Trendelenburg gait, compared with 25% of the matched cohort (P = .002). The odds of requiring surgical intervention was 14-fold higher for patients with a gluteus medius tear and gait deviation compared with those without gait deviation. There were no significant differences in the other parameters.
Conclusion:
Reduced power of resisted abduction and the presence of gait deviation on initial evaluation of patients with gluteus medius tears increases the likelihood of surgical intervention.
Gluteus medius tears are a common cause of lateral hip pain or greater trochanteric pain syndrome. 12 They are more common in women and have a peak incidence within the fourth to sixth decades of life. 17 Patients can present with either acute or chronic symptoms. Chronic presentation is more common, with patients typically complaining of insidious onset of dull pain over the proximal aspect of the lateral hip that may be worsened by lying on the affected hip, walking, or climbing stairs. 1,2 There is usually tenderness on palpation of the greater trochanter, a limp, or lurch on examination and reduced power on resisted abduction of the hip. 14 In contrast, patients with acute symptoms for traumatic tears can precisely pinpoint the onset of their pain. 18
Magnetic resonance imaging (MRI) is commonly used to diagnose gluteal tears. Tears are classified as tendinosis, partial-thickness, or full-thickness tears. 3 Tendinosis appears on MRI as increased signal intensity on T2-weighted images. 11 A partial-thickness tear is diagnosed when the tendon is thickened and there is increased signal intensity on T2-weighted and short inversion time inversion recovery images. 3 Focal discontinuity of the tendon with tendon retraction represents a complete tear. 3 If MRI is equivocal, then peritrochanteric local anesthetic injections may help confirm the diagnosis. 10 Relief of lateral hip pain but persistence of weakness on resisted abduction is usually suggestive of a tear.
Nonoperative management is the first line of treatment in chronic abductor tears. Treatment typically includes short-term use of a nonsteroidal anti-inflammatory medication, physical therapy for stretching and strengthening, and judicious use of corticosteroid plus local anesthetic injection into the trochanteric area. 15 Injection is best performed with image guidance under ultrasound or fluoroscopy to ensure precise anatomical localization. 17 Newer medical therapies include platelet-rich plasma, autologous blood, and high-volume saline injections; however, there is minimal high-level evidence to support their routine use. 15
Operative management for chronic tears is advocated for patients who have persistent pain and functional limitation despite a trial of nonoperative management. 8 Surgery may be performed open or endoscopically with the goal of achieving healing of the tendon to the bone at its anatomic footprint. 4 –6,16,19 –21 Surgery using either technique has demonstrated significant improvements in patient outcome scores, pain, mobility, and abductor strength. 4,5,7,21
Currently, there are no guidelines to predict which patients may ultimately require surgery to treat symptoms from gluteal tears. This information would be useful for prognosis as earlier operative intervention can help avoid the problems of tendon retraction and fatty infiltration that potentially may compromise surgical outcomes. 13 The aim of this study was to identify clinical features that may predict operative intervention in patients with gluteus medius tears.
Materials and Methods
Patient Selection and Matching Process
We conducted a matched-pair control study to determine clinical factors that may predict operative intervention in patients with gluteus medius tears. The inclusion criteria for the operative group consisted of patients who underwent endoscopic repair of the gluteus medius tendon between the period of June 2008 and August 2014. The exclusion criterion was patients with previous hip conditions such as Legg-Calve-Perthes disease or avascular necrosis. The matched-pair control group was selected on a 2:1 ratio based on age within 5 years, sex, a full-thickness gluteus medius tear diagnosed on MRI, and body mass index (BMI). All patients were treated with nonoperative management for 3 months. This consisted of a physical therapy regimen of abductor muscle strengthening and gait retraining. Thirty-one of 36 patients were also treated with 80 mg of methyl prednisone and 9 mL of 1% lignocaine ultrasound-guided injection into the peritrochanteric area. The remaining 5 patients refused or had contraindications to steroid use. Patients with persistent pain and functional impairment following 3 months of nonoperative management were offered surgical intervention. These patients formed the operative cohort. Patients with improvement in pain and function with nonoperative management for 3 months were discharged from review unless their symptoms worsened. Patients who had been discharged from review and had not re-presented for recurrence or worsening of symptoms formed the pool of patients for matching to determine the nonoperative cohort. Data for the study were prospectively collected but retrospectively reviewed. Our institutional review board approved this study.
Clinical Outcomes Assessed
Symptoms and signs were compared between the operative cohort and matched nonoperative cohort. The symptom that was compared was the presence of lateral hip pain. The signs that were compared were presence of greater trochanter tenderness, passive range of hip abduction, gait deviation, and power of resisted hip abduction. A gait deviation was characterized as either an antalgic gait, defined as a shortened stance phase on the affected side, or a Trendelenburg gait, defined as a positive Trendelenburg sign associated with the patient’s contralateral hip sagging or the trunk swaying to the contralateral side on single-leg stance. Power of resisted hip abduction was assessed with the patient in the lateral position and the hip abducted to 30° with the foot internally rotated to isolate the gluteal medius. Power was graded on a 0 to 5 scale, with 5 being strongest, based on the Medical Research Council (MRC) classification (Table 1). 9 The senior author (B.G.D.) assessed all patients.
Medical Research Council Grading of Power

Statistical Methods
The independent t test was used to assess differences between the groups for numerical data (hip abduction and power of resisted hip abduction). For categorical data (presence of lateral hip pain, presence of greater trochanter tenderness, and gait deviation), a chi-square analysis was performed to determine whether the presence of the parameters increases the odds of surgical intervention. There are no previous studies to allow a calculation of adequate sample size. Therefore, a post hoc analysis was performed to determine whether the study was adequately powered. For a sample size of 12 patients, the observed power for a 2-tailed hypothesis was 0.80, suggesting that the study is adequately powered for the differences observed. Statistical analysis was done using Microsoft Office Excel 2007 (Microsoft Corp) and SPSS 12.0 for Windows (IBM Corp).
Results
Table 2 shows the demographic characteristics of our surgical and matched controls. There were 24 patients in the surgical cohort who were matched to 12 patients in the nonsurgical cohort. Each cohort consisted of only women. The mean age of the surgical cohort was 65 years (range, 49-81 years) and 66 years (range, 52-82 years) for the nonsurgical group. The groups were also matched for BMI. The surgical cohort had a mean BMI of 29.23 kg/m2 (range, 21.55-44.398 kg/m2) and the matched control 29.95 kg/m2 (range, 20.20-43.59 kg/m2). The average duration of symptoms in the surgical group at initial presentation was 30.9 months (range, 0-156 months) compared with 39.2 months (range, 2-240 months) in the nonsurgical group. There were no significant differences between any demographic parameters.
Demographic Data Comparing Surgery and No Surgery Groups a

a BMI, body mass index.
There was a statistically significant difference found between the cohorts for power of resisted abduction. The mean power of abduction of the surgical cohort was 3.3 (95% CI, 3.28-3.98) and for the matched cohort 4.58 (95% CI, 4.29-4.87; P = .001) (Figure 1). There was no statistical difference in passive hip abduction between cohorts (Table 3).
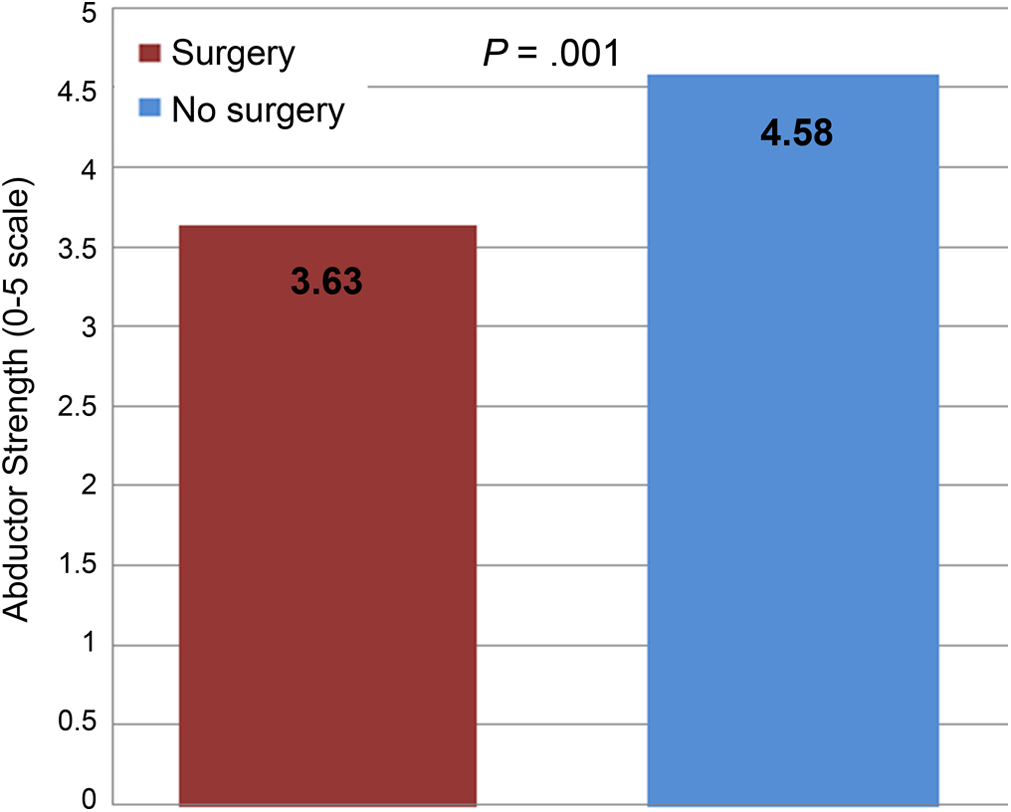
Comparison of abductor strength values for surgery versus no surgery. Abductor strength was graded on a 0 to 5 scale (5 being strongest) based on the Medical Research Council classification.9
Clinical Findings Comparing Surgery and No Surgery Groups a
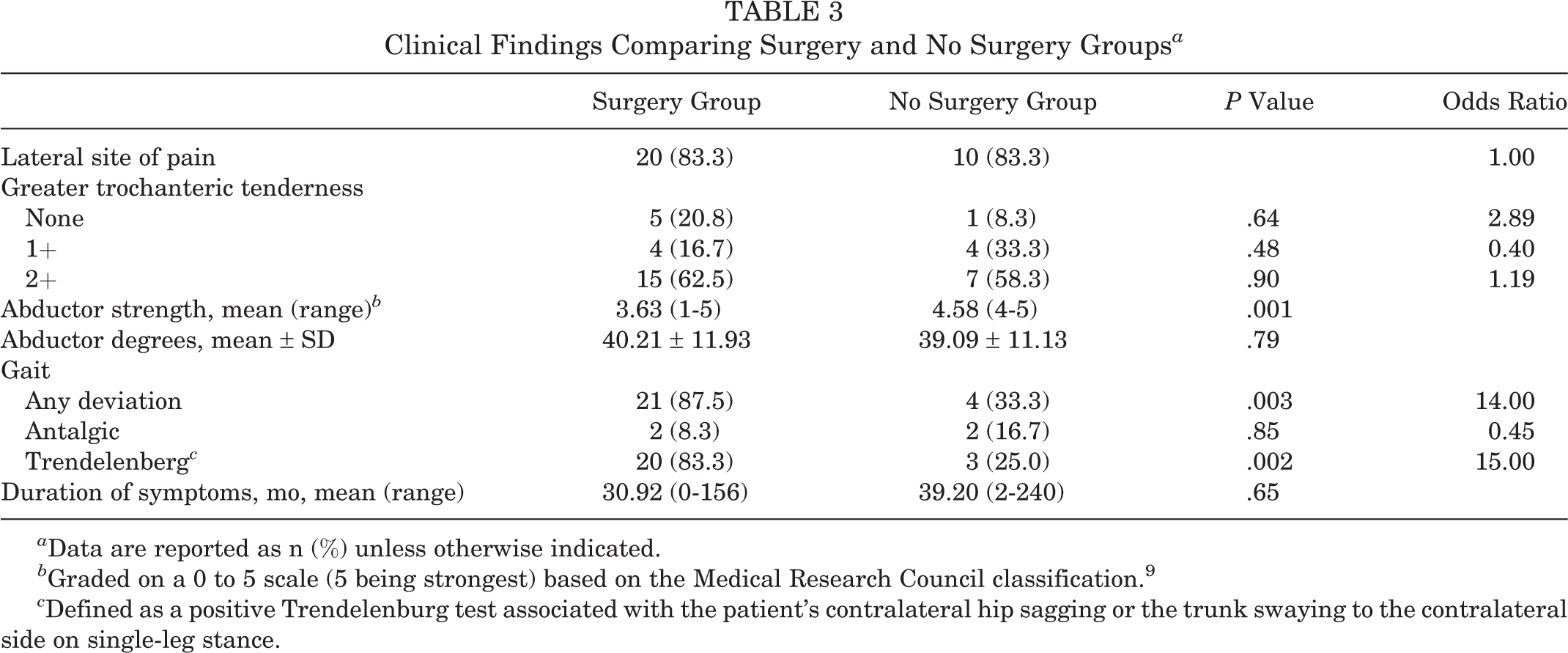
a Data are reported as n (%) unless otherwise indicated.
b Graded on a 0 to 5 scale (5 being strongest) based on the Medical Research Council classification. 9
c Defined as a positive Trendelenburg test associated with the patient’s contralateral hip sagging or the trunk swaying to the contralateral side on single-leg stance.
The majority (87.5%) of patients in the surgical cohort had a gait deviation, compared with 33% in the matched cohort. The gait deviation in the surgical cohort consisted of 8.3% antalgic and 83.3% Trendelenburg, compared with 16.7% antalgic and 25% Trendelenburg in the matched cohort. The odds ratio of requiring surgical intervention with a gait deviation due to a gluteus medius tear was 14 (P = .003). If the patient specifically had a Trendelenburg gait, then the odds ratio was 15 (P = .002). The odds ratio of requiring surgical intervention for the presence of lateral hip pain or the presence of trochanter tenderness was not significant (Table 3).
Discussion
There is currently no algorithm to predict who would benefit from early surgical intervention in patients with chronic gluteus medius tears. Therefore, we conducted a matched-pair controlled study to explore clinical factors on initial evaluation that may predict which patients may require surgical intervention and conversely which patients are likely to fail nonoperative management. We found that patients who presented with power of abduction of MRC grade less than 4 and any deviation of gait pattern were more likely to fail nonoperative management and require surgery. Other clinical factors such as presence of lateral-sided hip pain, duration of symptoms, abduction range of motion, and presence of greater trochanteric tenderness were not associated with increased likelihood of surgical intervention.
There are several studies that have demonstrated improved outcomes following operative intervention for gluteal tears. 4,5,7,16,19 –21 The intervention may be open or endoscopic. One of the parameters that has been found to improve postoperatively is abduction strength. Davies et al 5 reported on the 1- and 5-year outcomes following open abductor repair on a series of 22 patients. Their cohort preoperatively had a mean power of abduction of 3.1, which significantly improved to 4.7 at 1-year follow-up and was maintained at 5-year follow-up. McCormick et al 16 reported on endoscopic gluteal repairs and similarly found a significant improvement in the mean power of abduction from 3.3 to 4.6 at a mean follow-up of 23 months in their cohort of 11 patients.
Gait dysfunction has also been reported to significantly improve following gluteal repair. Walsh et al 21 reported on the largest series of 89 patients who underwent an open gluteal repair. In their series, 5% of patients had a normal gait preoperatively, which improved to 78% postoperatively at a minimum follow-up of 1 year. Davies et al 5 reported that 22 of 22 patients with open gluteal repairs had a positive Trendelenburg sign preoperatively compared with only 4 of 19 postoperatively at 5 years. These results are in agreement with our finding that surgical candidates are more likely to present with gait abnormalities.
There are several strengths to our study. This is the first study that has analyzed clinical factors that predict the need for operative intervention in patients with gluteus medius tears. Our results provided useful prognostic information to patients with lateral hip pain from gluteus medius tears. Specifically, patients have a higher risk of surgery when they have power of resisted hip abduction of less than 4 or an antalgic and/or Trendelenburg gait. The chance of operative intervention is 15-fold higher with a Trendelenburg gait. The matched-pair control methodology has the advantage of reducing the number of confounding factors as it aims to reduce heterogeneity between comparison groups, hence increasing the power of the study.
We recognize there are limitations to this study. The limitations include the limited number of patients in each of our study arms. The small number of patients is a result of the pair matching process. However, a post hoc analysis revealed that a sample size of 12 was of adequate power for the observed differences demonstrated. The matching process made it difficult to match for male patients; however, gluteus medius tears have been widely found to have a much higher prevalence in females. 17 The limited patient numbers may also cause type 2 errors in data analysis; specifically, other clinical parameters analyzed may have been significant with a larger sample size. We attempted to match patients as close as possible with respect to their gluteus medius pathology. Therefore, we only included patients with full-thickness tears. We did not match for the level of retraction of the tendon from its origin or the chronicity of tear as this would limit patient numbers. We presumed that similar to the rotator cuff in the shoulder, tendon retraction and chronicity of tear would most likely not correlate with clinical presentation. Future research may further help define clinical parameters that may predict surgical interventional for gluteal tears. The design would best involve a prospective follow-up of patients and clinical factors to determine which ones are predictive of surgical intervention.
Conclusion
We conducted a matched-pair study to determine clinical factors that may be predictive of surgical intervention for gluteal tears. We report that abduction power of a grade less than 4 and gait dysfunction are predictors of surgery. Moreover, patients presenting with gait deviation have a 14-fold increase of requiring surgical intervention. The findings have useful prognostic implications when discussing management options with patients, as surgical intervention has been shown to improve these outcomes.
Footnotes
One or more of the authors has reported the following potential conflict of interest or source of funding: The American Hip Institute receives indirect research support from Arthrex, MAKO Surgical, Breg, ATI, Pacira, Stryker, Orthomerica, and DJO Global.