Pulse oximetry measures heart rate (HR) and percent oxygen saturation (SpO). For aerobic exercise, whereby cellular oxygen demand and delivery are elevated and maintained for extended periods, HR and SpO values are consistent when measured by pulse oximetry. Yet due to its intermittent nature, HR and SpO values from resistive exercise may exhibit lower data reliability and repeatability.
OBJECTIVE:
Assess intra-rater reliability and repeatability of pulse oximetry HR and SpO values from two identical resistive exercise protocols.
METHODS:
Subjects ( 32) performed two calf press workouts on a flywheel-based ergometer as HR and SpO were measured before, between sets, and after exercise. Workouts entailed a 4-set 15-repetition protocol separated by 120-second rests. Intra-rater reliability was assessed with intraclass correlation coefficients (ICC). Repeatability was measured by the smallest real difference in absolute and relative terms.
RESULTS:
ICC and standard error of estimate results for HR ranged from 0.60–0.79 and 9.1–13.0 respectively. SpO ICC and standard error of estimate results ranged from 0.16–0.71 and 1.44–4.33 respectively. Between sets, smallest real difference values tended to be less for HR.
CONCLUSIONS:
Results demonstrate acceptable intra-rater reliability and repeatability for HR, but not SpO which we attribute to the exercise mode and protocol examined.
Pulse oximetry is a quick and simple to use tool to measure heart rate (HR) and percent oxygen saturation (SpO) values within the blood [1]. While traditionally used clinically to aid detection of numerous cardiorespiratory ailments that now include the COVID-19 virus, pulse oximetry was also examined as persons exercised at sea level and altitude; the latter usage assessed acclimatization and aided diagnoses of acute mountain sickness [2, 3]. For exercise it is assumed steady-state activity, whereby cellular oxygen demand and delivery are elevated and maintained over extended time periods, yield consistent HR and SpO values when measured by pulse oximetry [4, 5, 6]. Yet non-steady state activity such as resistance exercise has been largely ignored. In addition, resistive exercise may also see considerable contributions from oxidative phosphorylation and other aerobic metabolic pathways, particularly when done by women [7, 8].
Greater use of aerobic energy systems during resistive exercise may be indicative of heightened usage of oxidative phosphorylation to meet the body’s energy demands, while such a reliance between sets suggest the metabolic pathway plays a greater role in ATP resynthesis as the body recovers from the prior exercise effort. Resistive exercise SpO values obtained by pulse oximetry may offer insights on oxygen demand and delivery for this non-steady state modality. Due to the intermittent nature of resistive exercise, it is assumed HR and SpO values from this exercise modality would exhibit lower data reliability and repeatability. Despite the popularity of pulse oximetry, arterial catheterization is still considered the gold standard for SpO measurements [4].
As it pertains to HR and SpO values obtained from exercise, there are measurement limitations to pulse oximeters, particularly those that feature fingertip probes. They include finger movement as that produces motion artifacts, gripping objects as the measurement is concurrently attained, and poor perfusion states when skin temperatures are low such as when collected at altitude [1]. Others site light-emitting diode (LED) variability, hypoxemia, skin pigment and signal response as additional measurement limitations seen with pulse oximeters [5]. In addition, pulse oximetry use during exercise sees SpO values impacted by body temperature and pH [1]. It is assumed the variety of potential measurement limitations seen from pulse oximeters equipped with fingertip probes, combined with the intermittent nature of resistive exercise, may yield lower reliability and repeatability values for HR and SpO measurements than seen previously.
Several pulse oximetry studies did not quantify intra-rater reliability and repeatability, but instead used statistical tests such as Pearson correlations to note the level of agreement between measurements [3, 6, 9, 10]. Few papers examined HR and SpO data reliability and repeatability from pulse oximeters [11, 12, 13]. None of those studies entailed data collection during exercise [11, 12, 13]. Results suggest pulse oximetry exhibits highly reliable HR values, while those for SpO may be considerably less [11, 12, 13]. Since there is limited information on HR and SpO reliability and repeatability from pulse oximetry, which includes no papers on data obtained during exercise, this issue warrants further inquiry [11, 12, 13]. Thus, the current study quantifies intra-rater reliability and repeatability from pulse oximetry HR and SpO values obtained before, between sets, and after resistive exercise workouts. Subjects performed two identical workouts from which HR and SpO values were collected and subsequently examined for intra-rater reliability and repeatability. We hypothesize current HR and SpO values will yield results unlike those seen previously, but are nonetheless acceptable in accordance with established standards.
Methods
Subjects and their first visits
This research project received approval for the collection of human subject data from a university-based institutional review board that was compliant with ICMJE requirements. College-age subjects (15 men, 17 women) first gave informed written consent, and then filled out a medical questionnaire which stated they were free of conditions that could compromise their participation, prior to their project involvement. Subjects were healthy non-smokers who each made three laboratory visits close to the same times of day in order to limit the impact of circadian influences on our results. Their data were collected at sea level within a thermoneutral (21–22C, 40–45% humidity) exercise laboratory.
Subject’s first visits entailed their anthropometric data collection and familiarization to our resistive exercise device (YoYo Inertial Technologies; Stockholm, Sweden). Anthropometric values from our female subjects (mean sem) were as follows: height 169.0 1.8 cm, mass 65.5 2.5 kg, body fat percentage 25.2 1.8. Values for their male counterparts were: height 180.0 1.5 cm, mass 82 4.4 kg, body fat percentage 13.8 1.8. Height and mass were recorded with a stadiometer (Saltner Brecknell; Brooklyn NY) as subjects stood barefoot. Bioimpedance (Model BF-350, Tanita Corporation; Tokyo, Japan) measured body fat percentage estimates while subjects were in a euhydrated state. Subjects first visits lasted approximately 45 minutes.
Pulse oximeter
At their second and third visits, subjects wore a fingertip pulse oximeter (American Diagnostics Corporation; Happauge, NY) before, between sets, and after exercise. They wore the pulse oximeter on their right hand’s index finger. It was used and operated in accordance with the manufacturer’s specifications. When not in use, it was stored in accordance with guidelines (temperature, humidity, etc.) provided by the manufacturer. Figure 1 depicts how the pulse oximeter was worn when current data were collected.
Current study pulse oximeter (American Diagnostics Corporation; Happauge, NY) as it was worn when data were collected.
Second and third visits
Second and third visits entailed identical workout protocols, which allowed subject’s HR and SpO data to be compared statistically for their intra-rater reliability and repeatability. Per subject, the time between workouts averaged 17.8 2.6 days. For each workout subjects were instructed to arrive at our laboratory well rested. They began their second and third visits with a warm-up on a stationary cycle ergometer (Model 812E, Ergotest; Stockholm, Sweden) in which they pedaled for five minutes at a low (75–90 watt) workload. After the warm-up concluded, subjects sat on a flywheel-based ergometer for ten continuous minutes. Upon completion of the ten-minute period, subjects performed a 4-set 15-repetition seated calf press protocol on the ergometer. Subjects were encouraged to exert maximal voluntary effort throughout each set. Each repetition required exertion of concentric and eccentric torque provided by the subject’s plantar flexors. Subjects rested 120 seconds between sets. Per workout, HR and SpO data were collected before exercise (after ten continuous minutes of sitting), 60 seconds after sets 1–3, as well as at 0-, 5- and 15-minutes post-exercise.
Ergometer design and instrumentation
For the current study’s exercise mode, we chose to examine seated calf presses on the flywheel ergometer in order to limit finger movement artifacts that could impact results [1, 2, 5]. As subjects sat against the ergometer’s padded chair and backrest, inertial resistance provided by the flywheels was imparted to the footplate through a nylon strap, that alternately wrapped and unwrapped around the axle that connect the ergometer’s flywheels. With subject’s knees fully extended and their ankles dorsiflexed 10–15 degrees, they aligned the balls of their feet against the lower edge of the ergometer’s footplate at the start of each set. Torque imparted by concentric plantar flexor forces overcame the flywheel resistance and caused their rotation at rates proportionate to the torque exerted. Upon full ankle extension, the footplates’ movement was instantly reversed as eccentric forces were exerted and immediately slowed flywheel rotation rates. As the plantar flexors resisted the footplates’ returning motion, 10–15 degrees of dorsiflexion pre-stretched the plantar flexors before the next concentric action.
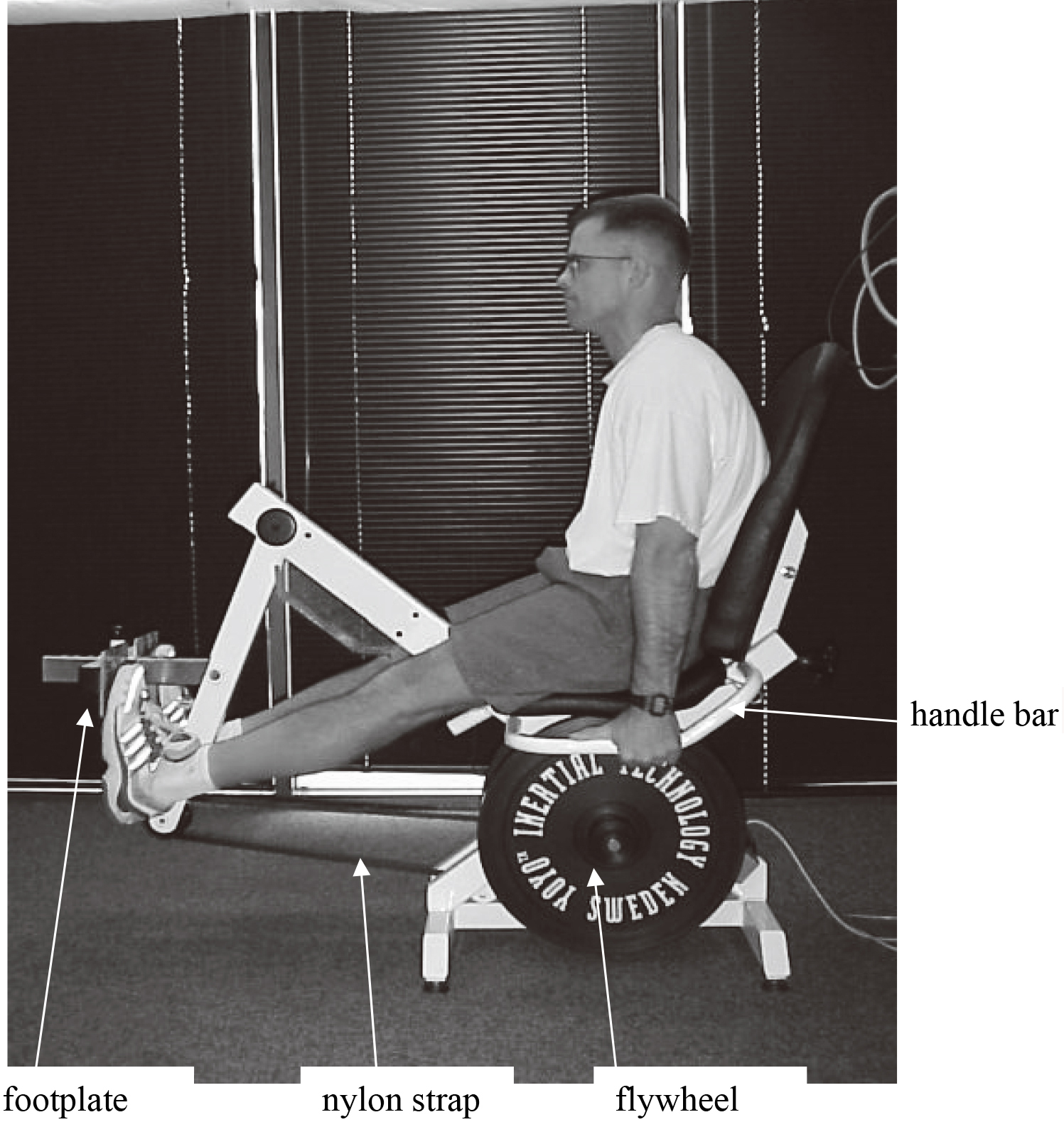
HR and SpO data were collected 60 seconds after sets 1–3 concluded as subjects sat passively on the ergometer without gripping its handlebars to limit the risk of data artifact [1]. To quantify exercise performance, flywheel rotation rates were recorded at 10 Hz with software (Labview Model 8.1; Austin, TX). Concentric, eccentric, and total work values were derived from the following formula: where by rotation inertia and angular velocity. Our instrumentation procedures and validity of data they measure were previously reported as acceptable [14, 15, 16]. Figure 2 depicts the position of subjects as they performed the seated calf press exercise on the flywheel ergometer.
Subject’s position as they performed seated calf presses on the flywheel ergometer (YoYo Inertial Technologies; Stockholm, Sweden).
Statistics
From the two workouts concentric, eccentric, and total work values were compared with -tests for paired samples, as significant differences may impact the intra-rater reliability and repeatability of the current study results. Dependent variable (HR, SpO) values were each examined for intra-rater reliability with intraclass correlation coefficients (ICC) for each of the seven time periods (pre-exercise, 60 seconds after sets 1–3, at 0-, 5- and 15-minutes post-exercise) in which data were collected. ICC analyses were done with a two-way mixed single measures model. Studies show ICC values in excess of 0.75 [17, 18] and 0.80 [19] signify excellent intra-rater reliability. Though subject measurements were collected and compared from two workouts, intra-rater reliability is applied within a context whereby, per subject, a single measure of one rater was performed. To assess intra-rater repeatability, HR and SpO were each calculated with the smallest real difference (SRD) over the seven time periods. SRD%, defined as SRD/mean 100, was also quantified, since SRD is impacted by the magnitude of absolute values.
Results
No subjects were injured from their project participation. Table 1 shows non-significant differences for inter-workout concentric, eccentric and total work values. Raw HR and SpO values appear in Tables 2 and 3 respectively, per time point, workout and subject. Average intra-rater reliability results appear in Table 4. They include ICC values for the seven time points examined at subject’s second and third laboratory visits. Associated with ICC, we included values in Table 4 to reflect on-average differences seen with the 32 sets of subject’s measures. Table 4 also includes standard error of the estimate (SEE) results, which equal the square root of the variance for deviations of observed values for a given variable from those predicted by linear regression [20].
Concentric, eccentric and total work values (mean sem) and results
1 workout
2 workout
-test score
CTW (joules)
8639 513
9041 550
1.8
ETW (joules)
8091 495
8322 500
0.3
TW (joules)
16731 1007
17363 1049
0.4
CTW: concentric total work. ETW: eccentric total work. TW: total work.
Raw HR data. Per column heading, final digits denote workout (1 or 2)
Average intra-rater reliability results obtained from our subjects ( 32)
Measure
pre-ex.
post set 1
post set 2
post set 3
0-post
5-post
15-post
ICC
HR
0.74
0.74
0.79
0.74
0.67
0.60
0.74
SpO
0.40
0.59
0.26
0.31
0.16
0.27
0.71
HR
0.87
0.87
0.89
0.87
0.83
0.80
0.87
SpO
0.70
0.79
0.62
0.65
0.57
0.62
0.85
SEE
HR
9.87
10.33
9.7
13.0
16.2
11.8
9.1
SpO
1.44
1.88
4.33
3.2
3.3
4.9
2.4
ICC: intraclass correlation coefficient. : eta squared. SEE: standard error of the estimate. 0-post, 5-post, 15-post: 0, 5 and 15 minutes post-exercise.
Table 4 includes higher absolute SEE values for HR as compared to SpO, which may simply be a function of score magnitude, as HR typically produces higher absolute values and exhibits a larger range of values, particularly during exercise. results also demonstrate higher values for HR. ICC results exhibit far greater intra-rater reliability for HR, as compared to SpO, values. For SpO changes there is a temporal component to current results, as ICC results were lowest following sets 1–3, but rose during post-exercise recovery. Table 5 shows our intra-rater SRD and SRD% repeatability results. SpO had lower values at the initial and final time points of data collection, and greater score dispersion after sets 2–3 and immediately post exercise (0-post). In contrast, SRD and SRD% HR results were lowest after sets 1 and 2. Administration of the same exercise protocol evoked similar HR changes, and data collection before and after workouts inherently may have elicited more score dispersion for intra-subject HR responses.
Average intra-rater repeatability results obtained from our subjects ( 32)
Measure
pre-ex.
post set 1
post set 2
post set 3
0-post
5-post
15-post
SRD
HR
4.2
3.5
2.7
4.6
5.7
5.6
3.7
SpO
2.2
2.5
5.8
5.4
5.4
4.6
2.1
SRD%
HR
5.4
3.9
3.0
5.0
5.2
7.0
4.8
SpO
2.4
2.7
6.1
5.7
5.8
4.9
2.2
SRD: smallest real difference. SRD%: smallest real difference percentage. 0-post, 5-post, 15-post: 0, 5 and 15 minutes post-exercise.
Discussion
Intra-rater reliability detects differences among persons tested repeatedly over time [21, 22, 23]. Tables 4 and 5 results suggest we can partly affirm our hypothesis, as pulse oximetry produced acceptable intra-rater reliability and repeatability results for HR, but not SpO. It is important to explain current results in relation to prior outcomes. Prior research assessed the reliability and repeatability of HR and SpO data obtained by pulse oximetry. Many of those prior outcomes concur with current HR and SpO results [11, 12, 13]. A study that did not entail exercise compared pulse oximetry HR data to values from two other measurement modes [11]. Pulse oximetry yielded ICC values in excess of 0.93, and was concluded to produce highly reliable HR values [11]. Yet like the current study, pulse oximetry SpO values, measured at multiple PaCO levels, were not as reliable [12]. Pulse oximetry HR and SpO values were measured as subjects sat comfortably under normobaric hypoxic conditions [13]. Much like the current study, HR reliability was high, but SpO values were biased by up to 3.3% [13]. Pulse oximetry probes equipped with a sensor that enabled contact force detection offered SpO errors less than 2%, and was concluded they had the potential to improve SpO reliability [24]. Thus like pulse oximetry studies collected from non-exercising subjects, our intra-rater reliability and repeatability HR and SpO results are like those seen previously [11, 12, 13].
Other pulse oximetry studies assessed data reliability and repeatability for SpO values with different statistical analyses than those used in the current study [12, 25, 26]. With pulse oximetry data collected from subjects at different arterial CO pressure levels, results showed low reliability as assessed by Bland-Altman plots, particularly in hypercapnic patients [12]. In similar fashion, Bland-Altman plots also showed low SpO repeatability and reproducibility from pulse oximetry in critically ill patients [25, 26]. Despite use of different statistical tests, current SpO repeatability and reproducibility values concur with data from prior pulse oximetry studies [12, 25, 26]. Smyth et al. saw higher (4.1–5.4%) SEE values for SpO data collected under normoxic and hypoxic conditions [27]. With an ear probe pulse oximeter, the hypoxic condition produced higher SEE values [27]. Current SEE values are similar to Smyth et al., and imply current SpO data are not accurate during non-steady state activity [27]. Yet some still question O saturation data, even from trained subjects during high-intensity exercise [6, 9].
Current ICC results for SpO are generally lower than those for HR. In addition, SpO had higher SRD% results for data obtained between sets. SpO values obtained during exercise are impacted by body temperature and blood pH which may deviate by up to 4% [1]. Another exercise study saw a similar SpO results in subjects similar to those of the current study [28]. Healthy men were divided into an exercise or control group with no crossover to assess aerobic exercise’s impact on O saturation and pulmonary ventilation [28]. It was hypothesized lower hyperventilation in trained subjects during testing would evoke smaller alveolar-arterial PO differences, while testing control subjects would lead to greater differences in O saturation [28]. Their hypothesis was affirmed by a two-way ANOVA with repeated measures, as trained subjects achieved VO gains through improved cardiorespiratory efficiency, while the untrained group’s O desaturation values were seen to be dependent upon VO levels and subject’s training status [28].
An examination of the repeatability of three different pulse oximeters was studied in male cyclists before and after they performed steady-state graded exercise [4]. Tests were done as cyclists wore a pulse oximeter on each ear lobe, while a third was attached to a fingertip. SpO values were compared to those from arterial catheterization, which was concurrently collected throughout testing. Results showed the fingertip pulse oximeter had higher data repeatability and values closest to those of arterial catheterization. In addition, in contrast to the notion intense exercise elicits lower O saturation, cyclists did not see a drop in that variable, even when tests caused their percent hemoglobin saturation to vary from 72–99% [4]. Differences between the Martin et al. and current studies were likely from the types of subjects and exercise protocols examined [4].
Yet pulse oximetry has produced mixed reliability and repeatability results from data obtained during or after aerobic exercise with fingertip probes [1]. Powers et al. collected SpO data with low SEE (1.4–2.0%) values and concluded pulse oximetry had sufficient accuracy and were useful during exercise tests, which are in contrast to the higher SEE values obtained by Smyth et al. [27, 29]. Perhaps the most comprehensive study on SpO values used three different groups of subjects and a variety of pulse oximeter models [1]. Subjects included healthy non-smoking adults, trained cyclists, and hospital patients with either CHF or COPD [1]. Subjects completed a cycle ergometer VO max test under normoxic conditions at which time their SpO data were collected. They concluded fingertip pulse oximetry produces conservative SpO results that underestimate actual values when used during exercise [1]. Disparities in SEE results for SpO values obtained during or after exercise among various investigations suggest the types of subjects and exercise modes examined may impact data reliability and repeatability [1, 4, 27, 29].
Other factors that may have also contributed to the current study’s low SpO intra-rater reliability and repeatability include carboxyhemoglobin and methemoglobin levels within the blood. Pulse oximetry utilizes multi-wavelength light to project onto a specific area of interest, and then photodetectors identify which wavelengths of light return to derive SpO values [5]. Carboxyhemoglobin and methemoglobin each absorb at similar light wavelengths as oxyhemoglobin, thus they could potentially inflate SpO values. Yet current study SpO values do not imply this was a major cause for the low intra-rater reliability and repeatability results, as Table 3 data from our subjects demonstrate no signs of inflated values, particularly those obtained between resistive exercise sets.
Many [1, 4, 29, 30], but not all [6, 9, 27], studies showed pulse oximetry SpO data collected across multiple workouts exhibited small amounts of data dispersion. Studies that noted low data dispersion used healthy trained subjects as they exercised under steady-state conditions [1, 4, 29, 30]. Such exercise protocols require and demand the delivery of a continual supply of oxygen, particularly during incremental exercise done against progressively heavier workloads [4, 29]. Such was not the case during the current exercise protocol, as some of our SpO data were collected between resistive exercise sets, which makes our investigation unique among pulse oximetry studies. During resistive exercise sets, there’s a modest energy contribution from aerobic metabolism [7, 8]. Yet between sets when ATP replenishment is a high priority, oxygen delivery and transport rise dramatically. Such large and transient changes in oxygen transport and delivery from non-steady state activity across multiple workouts are likely a big contributor to the current study’s greater SpO data dispersion and lower intra-rater results.
To achieve higher SpO intra-rater reliability and repeatability values, basic principles of pulse oximetry operation must be adhered to, such as ensuring probes are securely fastened to a subject’s fingertip, and data should not be obtained from smokers as they have higher carboxyhemoglobin levels [5]. Current results suggest fingertip pulse oximetry values collected before, between sets, and after resistive exercise workouts yield HR values with acceptable levels of intra-rater reliability and repeatability. Yet that was not the case for our SpO values, which we primarily attribute to the exercise mode and protocol examined. While current workouts examined a relatively small muscle group (plantar flexors) as the prime mover, it is anticipated as larger muscles engage in non-steady state exercise there would be even greater SpO data dispersion from higher fluctuations in oxygen delivery and transport.
Author contributions
CONCEPTION: John F. Caruso.
PERFORMANCE OF WORK: Alex C.S. Shefflette.
DATA ANALYSIS: John F. Caruso.
MANUSCRIPT PREPARATION: John F. Caruso.
SUPERVISION: John F. Caruso.
Ethical considerations
This research project received approval for the collection of human subject data from a university-based institutional review board that was compliant with ICMJE requirements. Participants provided written informed consent prior to their involvement in the project.
Funding
Funds came from an internal research grant.
Footnotes
Acknowledgments
We thank our subjects for their participation.
Conflict of interest
The authors have no conflicts of interest to declare. Given his role as an Editorial Board Member, John F. Caruso had no involvement nor access to information regarding the peer review of this article.
References
1.
YamayaYBoggardHJWagnerPDNiizekiKHopkinsSR. Validity of pulse oximetry during maximal exercise in normoxia, hypoxia, and hyperoxia. J Appl Physiol.2002; 92: 162-168.
2.
TannheimerM. The use of pulse oximetry at high altitude. Res Invest Sports Med.2020; 6: 481-483.
3.
TannheimerMKirstenJTreffGLechnerR. Usability of pulse oximetry during severe physical exercise at high altitude. Ger J Sports Med.2018; 69: 351-353.
4.
MartinDPowersSCicaleMCollopNHuangDCriswellD. Validity of pulse oximetry during exercise in elite endurance athletes. J Appl Physiol.1992; 72: 455-458.
5.
MengelkochLJMartinDLawlerJ. A review of the principles and accuracy of pulse oximeter estimates during exercise. Phys Ther.1994; 74: 46-54.
6.
WarrenGCuretonKMiddendorfW. Validity and reliability of pulse oximetry in highly trained endurance athletes. In: Proceedings of the Southeast Chapter of the American College of Sports Medicine Annual Meeting. 1990: 38. Abstract.
7.
DavisonSWRumplerWVBarbosaAGGutierrezEVCarusoJF. Metabolic responses to high-speed exercise measured via whole room calorimetry. Med Sportiva.2014; 18: 185-191.
8.
MorganBWoodruffSJTiidusPM. Aerobic energy expenditure during recreational weight training in females and males. J Sport Sci Med.2003; 2: 117-122.
9.
HansenJECasaburiR. Validity of ear oximetry in clinical exercise testing. Chest.1991; 91: 333-337.
10.
MacounTBotekMKrejciJMcKuneAJ. Vagal activity and oxygen saturation response to hypoxia: Effects of aerobic fitness and rating of hypoxia tolerance. Acta Gymnica2017; 47: 112-121.
11.
Losa-IglesiasMEBeccero-de-Bengoa-VallejoRBeccero-de-Bengoa-VallejoKR. Reliability and concurrent validity of a peripheral pulse oximeter and health-app system for the quantification of heart rate in healthy adults. Health Informatics.2016; 22(2): 151-159.
12.
MuñozXTorresFSampolGRiosJMartiSEscrichE. Accuracy and reliability of pulse oximetry at different arterial carbon dioxide pressure levels. Eur Respir J.2008; 32: 1053-1059.
13.
LauterbachCJRomanoPAGreislerLABrindleRAFordKRKuennenMR. Accuracy and reliability of commercial wrist-worn pulse oximeter during normobaric hypoxia exposure under resting conditions. Res Quart Exerc Sport. doi: 10.1080/02701367.2020.1759768.
14.
AlknerBTeschP. Efficacy of a gravity-independent resistance exercise device as a countermeasure to muscle atrophy during 29-day bed rest. Acta Physiol. Scand.2004; 181: 345-357.
15.
CarusoJFHernandezDAPorterASchweikertTSaitoKChoM, et al. Integrated electromyography and performance outcomes to inertial resistance exercise. J Stren Cond Res.2006; 20: 151-156.
16.
CarusoJFWilliamsJAHariPMcCoyJDCodayMARamseyCA, et al. Data reproducibility from the instrumentation of an inertial resistance exercise device suggested for use during space travel. Isok Exerc Sci.2006; 14: 371-382.
17.
FlansbjerUBHombackAMDownhamDPattenCLexallC. Reliability of gait performance tests in men and women with hemiparesis after stroke. J Rehabil Med.2005; 37: 75-82.
18.
KovelskiJEIngersollCDKnightKLMaharCP. Reliability of the BTE dynatrack isotonic dynamometer. Isok Exerc Sci.1996; 14: 53-62.
19.
KovelskiJEHeitmanRJGurichekLRErdmannJWTrundleTL. Reliability and effects of leg dominance on lower extremity isokinetic force and work using the closed chain rider system. J Sports Rehabil.1997; 6: 319-326.
20.
MorganBWoodruffSJTiidusPM. Aerobic energy expenditure during recreational weight training in females and males. J Sport Sci Med.2003; 2: 117-122.
21.
KropohlDJShawPK. Fundamentals of Polygraph Practice, 2015.
22.
MarinoRJJonesLKirshblumSTalJDasguptaA. Reliability and repeatability of the motor and sensory examination of the international standards for neurological classification of spinal cord injury. J Spinal Cord Med.2008; 31: 166-170.
23.
MokkinkLBTerweeCBPatrickDLAlonsoJStratfordPWKnolDL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international delphi study. Qual Life Res.2010; 19(4): 539-549.
24.
LiuCCorreiaRBallajiHKKorposhSHayes-GillBRMorganSP. Optical Fibre-based pulse oximetry sensor with contact force detection. Sensors.2018; 18: 3632.
25.
SeifiSKhatonyAMoradiGAbdiANajafiF. Accuracy of pulse oximetry in detection of oxygen saturation in patients admitted to the intensive care unit of heart surgery: comparison of finger, toe, forehead and earlobe probes. BMC Nursing.2018; 17: 15.
26.
Van de LouwACraccoCCerfCHArfADuvaldestinPLemaireFBrochardL. Accuracy of pulse oximetry in the intensive care unit. Intensive Care Med.2001; 27: 1606-1613.
27.
SmythRJD’UrzoADSlutskyASGalkoBMRebuckAS. Ear oximetry during combined hypoxia and exercise. J Appl Physiol.1986; 60: 716-719.
28.
MiyachiMKatayamaK. Effects of maximal interval training on arterial oxygen desaturation and ventilation during heavy exercise. Jpn J Physiol.1999; 49: 401-407.
29.
PowersSKDoddSFreemanJAyersGDSamsonHMcKnightT. Accuracy of pulse oximetry to estimate HbO2 fraction of total Hb during exercise. J Appl Physiol.1989; 67: 300-304.
30.
HadeliKOSiegelEMSherrillDLBeckKCEnrightPL. Predictors of oxygen desaturation during submaximal exercise in 8,000 patients. Chest.2001; 120: 88-92.