
Abstract
BACKGROUND:
No studies so far have investigated the effectiveness of the short-term intervention on the capacity of the ISP during throwing motion in baseball player with throwing disorder.
OBJECTIVE:
To investigate the effectiveness of short-term intervention on ISP during throwing motion and of physical examination in baseball player with throwing disorder.
METHODS:
Twenty-seven male baseball players with throwing disorder were hospitalized for 1 week and received physical therapy for 1 hour a day. In the pre- and post-hospitalized period, participants were evaluated using physical examinations (Hara test) and ISP and posterior deltoid muscle activity during throwing motion.
RESULTS:
The ISP during the late-cocking phase and follow-through phase at the time of hospital discharge were significantly greater than that at the hospital admission (
CONCLUSIONS:
The ISP in throwing motion is important to the stability of the glenohumeral joint during follow-through phase. Our results indicated that the improvements in the physical examination reflected favorably on the ISP during the throwing motion.
Introduction
The overhead throwing motion is involved with baseball predisposes the upper extremities to acute and chronic injuries [1]. These injuries primarily occur in pitchers; more than 25 percent result in extended sports time loss (10 days or more) [2, 3, 4]. In collegiate baseball, shoulder and elbow pain were involved in 36% of all injury complaints [4]. Injury rates in professional baseball players are increasing, with nearly half of the injuries occurring in the shoulder and elbow [2, 5]. Possible risk factors for these injuries that have been investigated include hip range of motion (ROM) deficits, parameters for workload such as pitch count and innings being pitched, pitch velocity, and throwing mechanics [6, 7, 8, 9]. Likewise, alterations in shoulder and elbow ROM have been linked to shoulder and elbow injuries in baseball players [10, 11]. Humeral retrotorsion, posterior capsular thickening, and infraspinatus muscle stiffness have been held responsible for the alterations in shoulder ROM for throwing athletes [12, 13]. Posterior shoulder tightness has been linked to internal and subacromial impingement due to superior migration of the humeral head. Identifying the primary mechanisms of posterior shoulder tightness will have the potential to provide the best approaches to resolving throwing-related ROM deficits. Unfortunately, the primary tissue mechanisms that are responsible for these ROM deficits remain elusive.
The rotator cuff muscles are most active when the forces on the shoulder joint are the highest. The infraspinatus contributes significantly to compressive forces at the glenohumeral joint [14]. Measurements of muscle activity have indicated that the infraspinatus is starting to be highly active at ball release and the level of activity remains elevated throughout all of the follow-through phase [14]. When the shoulder is close to the end range of stability, the infraspinatus is highly active and keeps the shoulder in the glenoid cavity [15]. In baseball players with throwing disorder, a high eccentric load is presumably applied to the infraspinatus by the throwing motion. However, no studies to date have investigated infraspinatus activity during throwing motion in baseball player with throwing disorder.
The throwing motion comprises a kinetic chain that is associated with the infraspinatus muscle activity during throwing motion. Furthermore, every movement in this kinetic chain is considered to influence its consequences. Thus, it is important to evaluate the physical examination considering the kinetic chain. The Hara test is useful for assessing abnormalities in the kinetic chain of upper extremity leading to shoulder pain in patients with throwing disorder [16]. Physical therapy for throwing disorder is aimed at improving the outcome of the physical examination. The Hara test provides a more effective basis to understand the clinical course for a return to pitching [16]. In addition, a better understanding of when and how much the infraspinatus muscle is active during throwing motion is helpful for physicians, therapists, trainers, and coaches in an effort to provide appropriate treatment and training and rehabilitation protocols for these athletes. The Hara test also allows health professionals to understand the mechanism of shoulder injuries. However, no studies to date have investigated the effect of short-term intervention on the clinical course of the physical examinations and the infraspinatus muscle activity during the throwing motion. Therefore, the objective of this study is to investigate the effectiveness of short-term intervention on infraspinatus muscle activity during throwing motion and physical examination in baseball players with throwing disorder. We hypothesized that infraspinatus activity in overhead throwing athletes with shoulder joint disorder would indicate different activity from those with intact shoulder joint that has been reported in the previous study. Thus, we investigated whether or not short-term physiotherapy intervention would positively change infraspinatus activity during the throwing motion.
Methods
Participants
A total of 27 male baseball players (mean age
A priori power analysis by G*power revealed that a power of 0.80 at an effect size of 0.70 with an alpha level of 0.05 required a sample size of at least 19 participants
Intervention
All participants have undergone physical therapy for 1 hour a day, and trained for 1 hour a day. Training sessions including warm-up, exercises, rest periods, and cool down were carried out under the supervision of the physical therapists.
The entire rehabilitation programs were completed once recovery of ROM, balanced movement of the joint capsule, proper proprioception, and dynamic stability were ensured with minimum pain or tenderness. The players could subsequently resume activity [16]. Thus, following general physical therapy, all participants could undertake flexibility exercise for posterior shoulder muscles (i.e., cross-body horizontal adduction stretch and sleeper stretch), rotator-cuff muscle strength and endurance training, rhythmical stabilization exercise, scapular retraction and protraction exercise, scapular stability muscle exercise (i.e., serratus anterior, middle trapezius, and lower trapezius), core muscle and lower body training.
Procedures
Electromyography measurements
The infraspinatus and posterior deltoid activities were recorded by surface electromyography (EMG) according to the recommended procedure [17]. For the infraspinatus, electrodes were placed two fingerbreadths inferior to the center of the spina scapulae. For the posterior deltoid, electrodes were placed two fingerbreadths inferior to the posterior margin of the acromion process. A ground electrode was placed on the acromion process. EMG data were collected using Telemyo 2400 EMG system (Noraxon, USA) operating at a sampling rate of 1500 Hz. Self-adhesive bipolar surface electrodes (Blue Sensor Ag/AgCl; AMBU A/S, Denmark) were then attached. Correct electrode placement was confirmed by inspection of all EMG signals on an oscilloscope during resisted contractions of each muscle.
Measurement of the muscle activation during throwing motion
The throwing motion was analyzed on the video footages recorded by two high-speed cameras (Sports Coaching Cam; Sports Sensing, Japan) to determine the throwing phase. The throwing motion was divided into four event segments as follows: early cocking phase, late cocking phase, acceleration phase, and follow-through phase [18]. The participants were given as much time as about 15 minutes to warm up according to their normal pregame or pre-practice warm-up procedure.
Each participant was individually prepared for electrode placement by cleaning and slight abrasion of the skin surface at the electrode sites. The electrodes were attached with their self-adhesive backing and then secured in place to the athlete’s arm by overwrapping with flexible athletic tape. The wires from the electrodes were then connected to a wireless transmitter worn at the participant’s waist. Before the pitching trials started, each individual participant was allowed to throw several trial pitches at full speed so as to become comfortable with the electrodes and wires.
All participants threw the ball from a designated starting position in the middle of the video capture field of vision towards a target area on a net in front of them, which was located approximately 16 feet from the simulated mound. The participants had an unlimited amount of time to throw a total of 5 pitches. One of the most satisfactory trials by the participant was employed as an analysis target.
Maximum voluntary isometric contraction measurement
Once the pitching trials were completed, maximal muscle activity was measured during a 5-s maximum voluntary isometric contraction (MVIC) against manual resistance. The MVIC tests for the infraspinatus muscles were performed while the participant was in a sitting position with the elbow being flexed at a 90 degrees angle. The MVIC tests for the posterior deltoid muscle were performed while the participant was in a prone position with the shoulder abduction at a 90 degrees angle and elbow flexed at a 90 degrees angle. The EMG data from the MVIC trials were processed in the same manner as those of the throwing trials. The MVIC was used as a normalizing value (100%).
Physical examination
In this study, we used the Hara test as a physical examination. The Hara test [16] is effective in assessing the upper-extremity kinetics for abnormalities that are responsible for shoulder pain patients with throwing disorder. The Hara test consists of 11 physical examinations items that are associated with the scapular and humeral kinetic chain: 1) scapula-spine distance (Fig. 1), 2) elbow extension test (Fig. 2), 3) elbow push test (Fig. 2), 4) muscle strength of abduction, 5) muscle strength of external rotation, 6) muscle strength of internal rotation, 7) combined abduction test (Fig. 3), 8) horizontal flexion test (Fig. 4), 9) capsular laxity tests, 10) subacromial impingement tests, and 11) hyper-external rotation test (Fig. 5). The total score (i.e., the number of “intact” results) for the Hara test and the abnormalities in each examination item were evaluated. The number of “intact” results among the 8 physical examination items except muscle strength test was recorded as the total Hara test score for each participant. The maximum total score (8 points) represented all “intact” results (i.e., no abnormality found); participants with lower scores are considered to have a potential problem in the upper-extremity kinetic chain. The abnormal rate of each examination item was also used for comparison in this study.
In the scapula-spine distance test, the distance from the medial edge of the scapular spine to the spinous process of the thoracic spine is measured with the arms at the sides.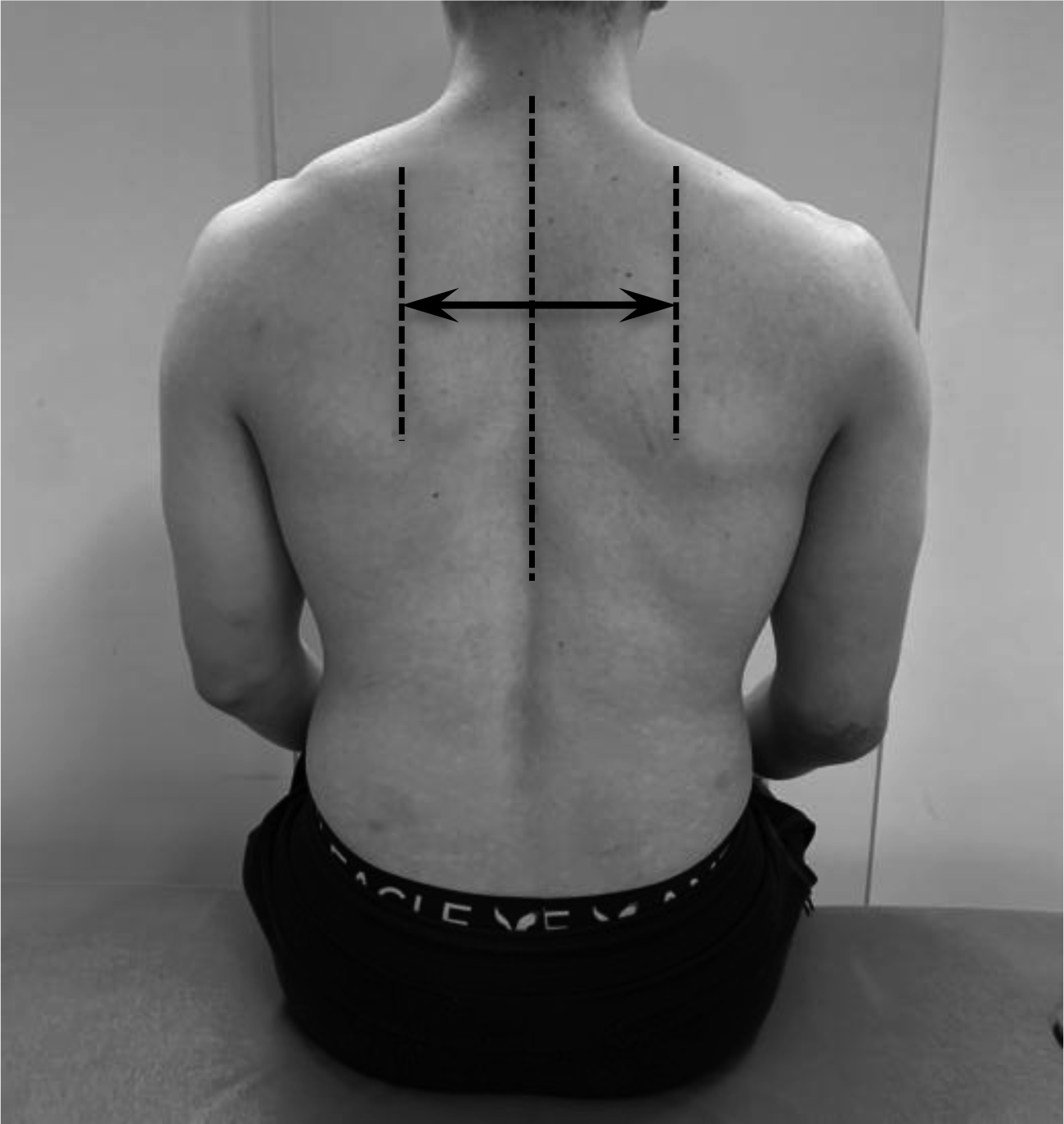
(1) Elbow extension test and (2) elbow push test for assessment of scapular stability. These tests are performed with the shoulders in 90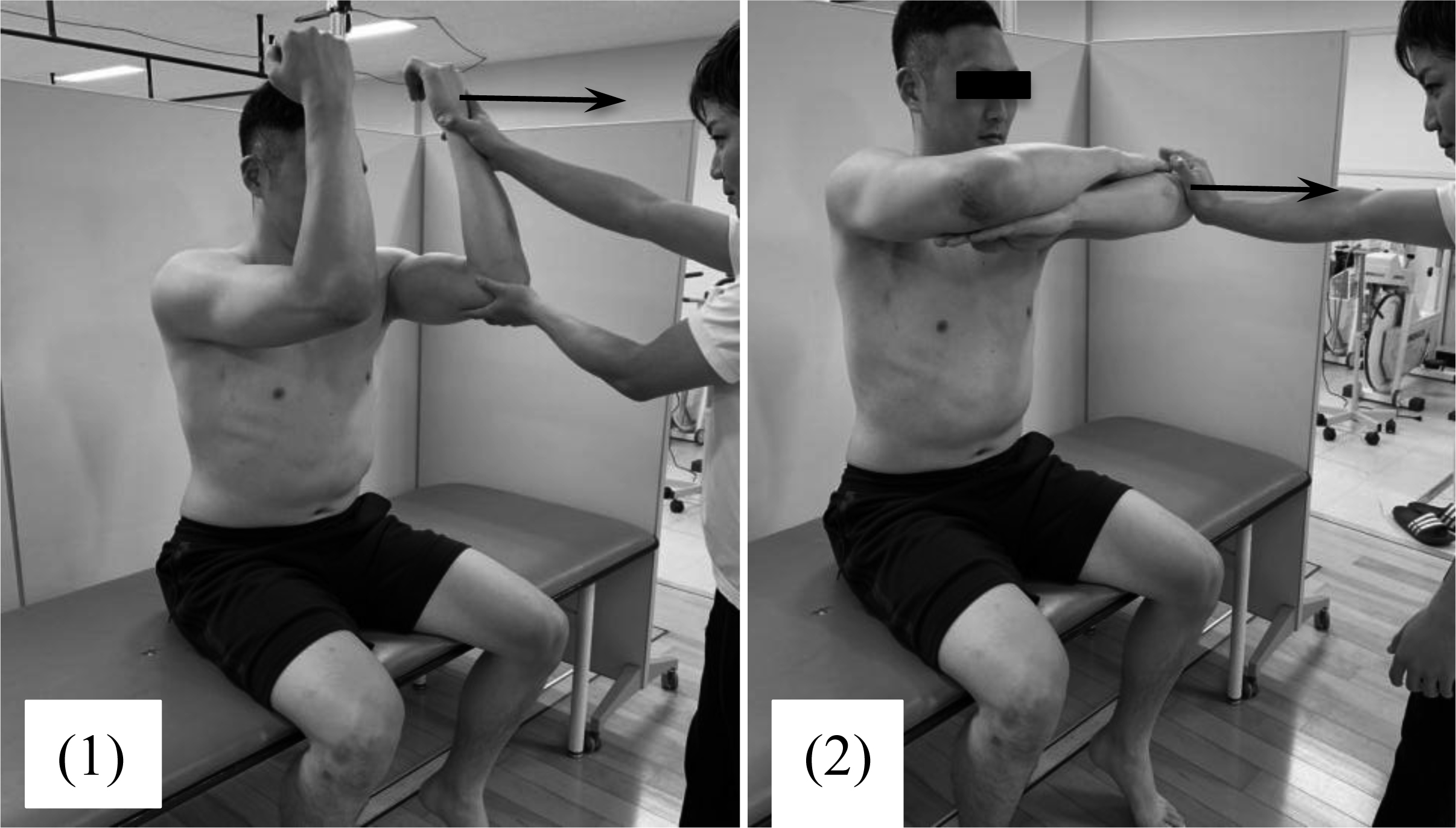
Combined abduction test for assessment of posterior shoulder tightness. The examiner completely prevents any movement of the scapula by holding it.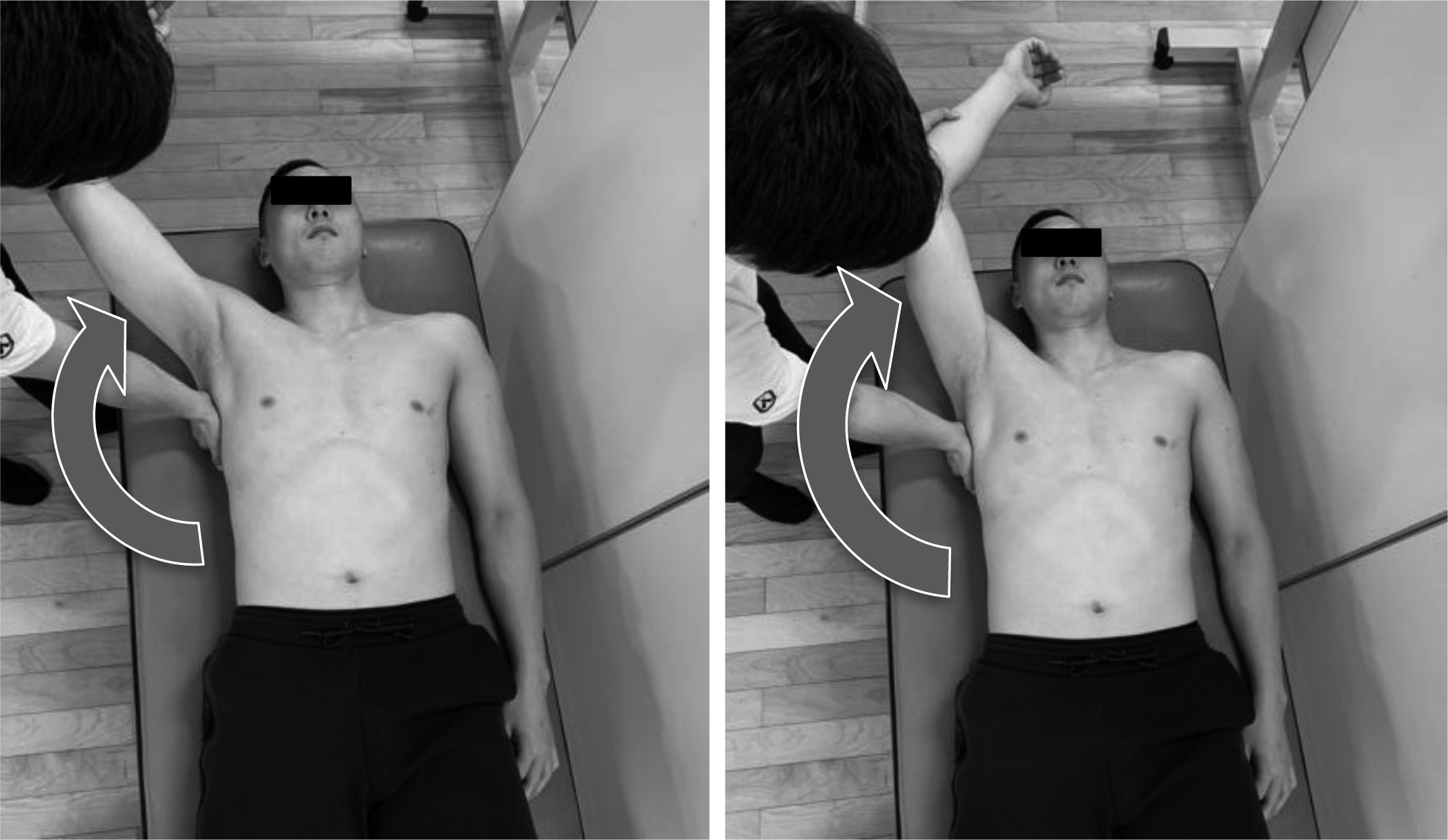
Horizontal flexion test for assessment of posterior shoulder tightness. The examiner completely prevents any movement of the scapula by holding it and horizontally flexes the humerus.
The hyper-external rotation test, which evaluates peel back of the superior labrum and pathological internal impingement, is performed in 90
The scapula-spine distance, elbow extension test, elbow push test, and subacromial impingement tests underwent while the participant was in a sitting position. Patients lay supine for the combined abduction test, horizontal flexion test, capsular laxity tests, and hyper-external rotation test.
To assess the scapular alignment, the scapula-spine distance test, we measured the distance from the medial edge of the scapular spine to the spinous process of the thoracic spine with their arms being held at their sides (Fig. 1). The reference point on the thoracic spine was identified as the nearest spinous process. When there was more than 1.0 cm difference between the left and right sides, the result of the scapula-spine distance test was considered to be abnormal. To assess the scapular stabilizers, the elbow extension test and elbow push test were performed on patients with their shoulders in forward flexion of a 90 degrees angle (Fig. 2). For the elbow extension test, the participant extended his elbow joint from forward flexion of a 90 degrees angle by employing their maximum force while the examiner held the participant’s forearm to counteract his extension force (Fig. 3). For the elbow push test, the participant with his contralateral elbow being grabbed by each hand pushed each elbow in turn anteriorly with maximum force while the examiner counteracted it by holding the elbow of the participant (Fig. 4). We determined the results of the elbow extension test and elbow push test to be abnormal when the muscle strength on the dominant side was less than that on the non-dominant side. To assess the posterior tightness of the shoulder joint, participants performed the combined abduction test and horizontal flexion test while the examiner fixed the scapula and prevented it from moving by holding it. The humerus was passively abducted in the coronal plane for the combined abduction test (Fig. 3) and horizontally flexed for the horizontal flexion test (Fig. 4). If the participant’s upper arm failed to touch his head during glenohumeral abduction with his scapula fixed, the combined abduction test was graded as abnormal. The horizontal flexion test was determined to be abnormal when the participant was unable to reach around the contralateral shoulder to touch the bed during horizontal flexion with his scapula being fixed. Capsular laxity was evaluated by load-and-shift testing in the anterior, posterior, and inferior directions. Likewise, anterior apprehension and relocation tests were also done. When the dominant side showed increased laxity or when the participant felt that the shoulder was unstable during any test, capsular laxity was determined to be abnormal. To evaluate subacromial impingement, we performed the Neer [19], Hawkins [19], and Yocum tests [20]. If the participant felt shoulder pain during any of these tests, subacromial impingement testing was graded as abnormal. The hyper-external rotation test (Fig. 5), which evaluates peel back of the superior labrum [21, 22] and pathologic internal impingement [23, 24], was performed in a 90 degrees angle of shoulder abduction with the elbow being flexed at 90
Finding on outcome measures at admission and at discharge by short-term hospitalization
Abnormal rate of Hara test at admission and discharge
*Indicates a significant difference at discharge compared with at admission (
The Shapiro-Wilk test was used to assess the normality of the data. The infraspinatus and posterior deltoid muscle activities were compared between admission and discharge using the Wilcoxon signed-rank test. The total Hara test scores were compared between admission and discharge using the paired
The effect size was calculated using the equation
Results
Muscle activity of infraspinatus and posterior deltoid muscles
Table 1 depicts the significant difference in infraspinatus muscle activities at admission and discharge. The infraspinatus activity during the late-cocking and follow-through phases at discharge (26.3
Abnormal rate in Hara test
The total Hara test scores at discharge (5.1
Discussion
The most important finding of this study was that short-term intervention on upper-extremity kinetic improved abnormal physical examination and infraspinatus muscle activity during throwing motion also changes.
In this study, we measured shoulder external rotator muscle activities during throwing motion of the baseball players with throwing disorder. Furthermore, we compared the abnormal rate of the physical examination at admission to the hospital and at the time of discharge. To the best of our knowledge, this is the first study to investigate the effect of a one-week physical therapy intervention on infraspinatus muscle activity during throwing motion in baseball players with throwing disorder. First, the infraspinatus muscle activity during acceleration phase at admission showed greater than the other pitching phases. Previous studies reported that the infraspinatus and teres minor muscle activity had similar patterns to the peak activity in the late cocking and follow-through phases [18]. In addition, the infraspinatus muscle activity of the throwing motion is important to the stability of the glenohumeral joint during the follow-through phase. These reports are intended for healthy baseball players while the results of this study, in which the electromyographic activity of infraspinatus reached the peak in the acceleration phase, represented the characteristics of throwing disorder. The acceleration phase begins when the humerus has reached maximum external rotation and ends with ball release. In this phase, the angular velocity of the humerus reaches 7,000
Eight physical examination items except for rotator cuff strength test of Hara test improved at discharge compared to admission. The improved test items included the combined abduction test and horizontal flexion test to assess the posterior tightness of shoulder joint; elbow extension test and elbow push test to assess the scapular stabilizers; and capsular laxity test to assess loose of the glenohumeral joint. Glenohumeral internal-rotation deficit, rotator cuff strength deficit, and scapular dyskinesis were recently identified as potential risk factors in the population of baseball players [29, 30]. In particular, pre-season training reduced internal rotation range of motion, while a strength deficit in the external rotators increased the risk for overuse chronic shoulder pain in these athletes. Posterior shoulder tightness is a common adaptation, if not the most common, that is seen on the dominant side of overhead throwing athletes of multiple sports disciplines [28]. This manifests itself clinically as decreased combined abduction test and horizontal flexion test results and is believed to be the result of both capsular tightness and muscular contracture. It is hypothesized that the cumulative loads on the posterior shoulder during deceleration of the throwing motion could cause microtrauma and scarring of this soft tissue [28]. The improvement of posterior shoulder tightness noted after rehabilitation was considered to be the effect of continued and well-executed passive and ballistic stretches, which should always be incorporated in a part of the rehabilitation program to reach a complete and balanced shoulder ROM. Normalization of humeral rotation means that the humeral head is located near the center of the glenoid fossa, being kept the shoulder in the glenoid cavity by infraspinatus activity [15]. Scapular stabilizers (i.e., elbow extension test, elbow push test) significantly improved at the discharge. Merolla et al. reported that scapular dyskinesis is a starting point in the chain of events that lead to the supraspinatus and infraspinatus weakness [31]. Therefore, it is conceivable that improved the scapular stabilizer led to rotator cuff function improvement result. During overhead activities, the scapular stabilizing and rotator cuff muscles function in a balanced manner to maintain a centered relationship between the humeral head and the glenoid fossa [32]. This dynamic stability mechanism is crucial to glenohumeral joint stability during the mid-ranges of arm movement [33].
The infraspinatus muscle activities during the late-cocking and follow-through phases were significantly greater at discharge than at admission. After short-intervention for one weak, which provided the baseball players with throwing disorder, as intended, with minimum pain or tenderness in order to complete recovery of ROM, proper proprioception, the infraspinatus muscle activity increased in the late-cocking and follow-through phases. In particular, the effect sizes revealed large effects for follow through phase. This suggests that the feature of the infraspinatus muscle activity after short-term intervention has approached that of healthy player as reported by Jobe et al. [18]. As a result, providing short-term intervention to abnormal physical examination of the shoulder had a positive influence on infraspinatus muscle activity during the throwing motion.
No date on healthy baseball players was not included in the present study. This is the major limitation of the present study. However, the present study was a preliminary study aimed at investigating changes in infraspinatus muscle activity during throwing motion due to short-term hospitalization that has been planned to improve the physical examination results of baseball players with throwing disorder. Our future focus is to investigate the differences in infraspinatus muscle activity during throwing motion in baseball players with throwing disorder versus healthy baseball players. Another limitation of this study was that the players of various positions were included. Therefore, our results cannot be generalized beyond this sample to the greater population of position. Moreover, only EMG was used to assess throwing performance. This means that we did not measure ball velocity or kinematics of the shoulder during the throwing motion. However, despite changes in the infraspinatus activity noted at discharge, the posterior deltoid muscle activity did not change. Based on these findings, a possible interpretation is that the physical therapy that has been provided during the short-term intervention had a lesser influence on throwing performance, such as ball velocity and kinematics of the shoulder.
Conclusions
This is the first study to examine the effects of the short-term intervention on the infraspinatus muscle activity during throwing motion and physical examination results in baseball players with throwing disorder. Our results indicated that the improvement in physical examination results lead to changes in infraspinatus muscle activity during the throwing motion. This finding provides significant insights into the development of a new assessment framework for the baseball players that is suffering from throwing disorder and may help elucidate the mechanism of shoulder injury.
Footnotes
Conflict of interest
None of the authors declare any conflicts of interest associated with this study.