
Abstract
Background:
Previous studies have reported visually observed apparent muscle atrophy in the infraspinous fossa of the dominant arm of overhead athletes. Several mechanisms have been proposed as etiological factors, including eccentric overload, compressive spinoglenoid notch paralabral cysts, and cumulative tensile suprascapular neurapraxia.
Purpose:
To report the prevalence of apparent infraspinatus atrophy in male professional tennis players and to determine whether the suspected atrophy correlates with objectively measured weakness of external rotation.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 153 male professional tennis players underwent a musculoskeletal screening examination that included visual inspection of the infraspinous fossa. Infraspinatus atrophy was defined as hollowing or loss of soft tissue bulk inferior to the scapular spine in the infraspinous fossa of one extremity that was visibly different from the contralateral extremity. This finding was observed and independently agreed upon by both an orthopaedic surgeon and a physical therapist during the examination. Also assessed were rotator cuff instrument-assisted manual muscle testing, visual observation of scapular kinesis (or motion), and glenohumeral joint range of motion for internal and external rotation and horizontal adduction.
Results:
In the 153 players, dominant-arm infraspinatus atrophy was observed in 92 players (60.1%), and only 1 player (0.7%) was identified with nondominant infraspinatus atrophy. A Pearson correlation showed a significant relationship between the presence of dominant-arm infraspinatus atrophy and dominant-arm external rotation strength measured in neutral abduction/adduction (at the side) (P = .001) as well as between the presence of dominant-arm infraspinatus atrophy and bilateral external rotation strength measured at 90° of glenohumeral joint abduction (P = .009 for dominant arm and .002 for nondominant arm). No significant correlation was found with scapular dyskinesis, glenohumeral range of motion, or instrument-assisted manual muscle testing of the supraspinatus (empty-can test).
Conclusion:
Visually observed infraspinatus muscle atrophy is a common finding in the dominant shoulder of asymptomatic male professional tennis players and is significantly correlated with external rotation weakness. This condition is present in uninjured players without known shoulder pathology and is not related to glenohumeral joint internal rotation, total rotation range of motion, or scapular dysfunction. Players with visually observed infraspinatus atrophy should be evaluated for external rotation strength and may require preventive strengthening.
Atrophy of the infraspinatus muscle has been reported in unilaterally dominant upper extremity athletes and in patients with shoulder pathology. 1,5,35 The reported prevalence of dominant-arm infraspinatus atrophy in the overhead athlete has ranged between 4% and 52% in volleyball, baseball, and tennis players. ** Visual observation has been the primary method of identifying atrophy in the infraspinous fossa of the scapula on clinical examination and in carrying out preventive screening evaluations. 11,12,15,52
Several causative mechanisms have been proposed for the pathogenesis of infraspinatus atrophy in the overhead athlete. These include eccentric overload, compressive spinoglenoid notch paralabral cysts, irritation of the suprascapular nerve at the spinoglenoid notch, cumulative tensile suprascapular neurapraxia, and compression via enlarged venous structures. 4,8,16,32,35,45,47,52 High levels of muscle activation have been reported in the posterior rotator cuff and scapular musculature during the follow-through phase of the tennis serve and forehand groundstroke. 26,43 This specific activation subjects these muscles to repetitive eccentric overload, 26,43 supporting the proposed pathomechanics of eccentric overload and glenohumeral and scapulothoracic distraction. However, the pathophysiologic process of isolated infraspinatus atrophy in healthy, uninjured overhead athletes is currently unknown, with no definitive cause identified in the literature. 28,29,38,39,40,44,52
Numerous studies have studied the glenohumeral joint range of motion (ROM) in the overhead athlete. †† Using goniometric assessment, consistent findings of reduced dominant-arm internal rotation and increased dominant-arm external rotation have been reported in these athletes. An additional proposed mechanism for isolated infraspinatus atrophy includes posterior shoulder tightness (shoulder internal rotation ROM loss or glenohumeral internal rotation deficit), which in tennis players could result in intermittent compression of the suprascapular nerve as the glenohumeral joint is placed in adduction and internal rotation during the follow-through phases of the serve and forehand. 35,52 Plancher et al 36 reported that the spinoglenoid ligament, which spans the top of the spinoglenoid notch, has portions that insert directly into the posterior capsule. 37 Combined positions of scapular protraction and glenohumeral joint adduction and internal rotation have been reported to produce tension in the spinoglenoid ligament through the posterior capsular attachment and could increase compression on the suprascapular nerve in the overhead athlete. Oyama et al 34 showed increases in dominant-arm scapular internal rotation and protraction in elite-level tennis players and in other overhead athletes. This scapular positional modification could further exacerbate suprascapular nerve compression. 18 Finally, Sandow and Ilic 45 proposed that the superior aspect of the infraspinatus may impinge on the suprascapular nerve at the spinoglenoid notch in positions of abduction and external rotation, which corresponds to the position of the glenohumeral joint during the cocking phase of the tennis serve. 19,26,35
The purpose of this study was to report the prevalence of isolated infraspinatus atrophy in professional male tennis players and determine its relationship to external rotation strength, glenohumeral joint ROM, and scapular dysfunction. We hypothesized that dominant-arm infraspinatus atrophy would be prevalent in this population and would be correlated with external rotation strength.
Methods
Participants
In this institutional review board–approved study, 153 male professional tennis players were evaluated at Association of Tennis Professionals (ATP) Tour and Grand Slam (International Tennis Federation) tournaments by the same physical therapist (T.S.E.) and orthopaedic surgeon (G.S.W.) as part of a voluntary comprehensive musculoskeletal injury prevention program. None of the players had significant injuries that would prevent them from participating fully in a professional tennis tournament. Players were not excluded if they had subtle pain or soreness. No player in this study sample had a history of shoulder surgery. The orthopaedic surgeon obtained a detailed musculoskeletal injury and surgical history as part of the musculoskeletal screening.
Procedures
For the visual assessment of infraspinatus atrophy, the examiners assessed the player from a posterior view with the player’s feet placed together for standardization. The assessment took place with the participant’s arms (1) resting at his sides and (2) placed on his hips with the thumbs pointing posteriorly (hands-on-hips position). A yes/no (present/absent) classification for infraspinatus atrophy was used to record the findings on an evaluation form that was later transferred to an Excel spreadsheet. No grading was used to quantify the severity of atrophy in this investigation. For the purposes of this study, infraspinatus atrophy was defined as “hollowing or loss of soft tissue bulk inferior to the scapular spine in the infraspinous fossa of one extremity that was visibly different from the contralateral extremity” (Figure 1). Players with no distinguishable difference between sides did not meet the definition of infraspinatus atrophy for this investigation. Evaluation of each player occurred simultaneously by the 2 examiners, who independently recorded their findings on a data evaluation form. There was 100% agreement between the orthopaedic surgeon and physical therapist in all 153 player evaluations.

Posterior view of an elite tennis player with right unilateral infraspinatus atrophy.
Manual Muscle Testing
All 153 participants underwent evaluation for rotator cuff strength, shoulder ROM, and scapular dyskinesis. Muscle testing was performed bilaterally for external rotation strength both at the side (0° of abduction/adduction) and in 90° of coronal plane abduction using a hand-held dynamometer (Lafayette Instrument Company) with the participant in a seated position. The examiner used one hand to stabilize the participant’s elbow while the dynamometer was placed just proximal to the wrist joint for testing. These test positions have been validated by prior research and represent a primary focus on infraspinatus strength in 0° of abduction/adduction and greater contribution of relative teres minor activation in 90° of abduction. 20,27,41 A “make” test was used, recording the best of 2 trials; measurements were recorded in kilogram-force (kgf). Participants were also tested bilaterally for supraspinatus strength in 90° of abduction in the scapular plane with full internal rotation (empty-can position). 22,41 Riemann et al 41 has established the reliability of instrument-assisted manual muscle testing for shoulder strength including external rotation.
Scapular Evaluation
Evaluation of scapular kinesis (movement) to detect the presence of possible scapular dyskinesis was performed using visual observation and the procedure outlined by Kibler et al. 25 Participants were given a 1-kg weight (Theraband Soft Weight; Performance Health) for each hand. With the participant standing and the examiners viewing from a posterior position, the participant was asked to slowly and deliberately elevate his arms fully overhead, performing several repetitions in both forward flexion (sagittal plane) and abduction (coronal plane). A yes/no grading classification was used, and agreement was needed between the orthopaedic surgeon and physical therapist for inclusion. 25,48 Each scapula (dominant and nondominant side) was assessed and graded individually.
Range of Motion
Testing for glenohumeral joint ROM was performed using methods with scapular stabilization to minimize substitution and compensation. 14,50 All measures were performed with the participant in the supine position. Bilateral internal and external rotation ROM was measured in 90° of coronal plane abduction with no overpressure used at end ROM. Gravity served as the standard endpoint force. Stabilization of the scapula by the examiner’s hand on the spine of the scapula and coracoid minimized contribution from the scapulothoracic articulation to better isolate glenohumeral joint motion. 50 The test-retest reliability of this measurement technique has been previously published. 14,50
Shoulder horizontal adduction ROM was measured bilaterally using a standardized technique with the participant in a supine position. One of the examiner’s hands provided stabilization to the lateral border of the scapula starting in 90° of shoulder flexion in the true sagittal plane. From this starting position, the participant’s upper arm was guided with no overpressure into horizontal adduction. A digital inclinometer (Pro 3600 SPI-Tronic) was placed along the lateral border of the upper arm to obtain the degree of horizontal adduction relative to neutral. The reliability of this measurement has been published previously for this instrument and technique. 30
All strength and ROM measurements were taken by the same physical therapist throughout this investigation. An order of convenience was followed during the musculoskeletal screenings, with no randomization of starting extremity.
Data Analysis
Statistical analysis was performed using SPSS (IBM) to generate descriptive statistics and analysis. A Pearson correlation was used to determine the relationship between visually observed infraspinatus atrophy and external rotation and supraspinatus strength as well as glenohumeral joint ROM and scapular dyskinesis. The Kolmogorov-Smirnov and Shapiro-Wilks tests confirmed the normality of the data variables. Independent t tests were used to compare means between players who did have visually observed infraspinatus atrophy in the dominant arm versus those who did not. We used 17 independent t tests with a Bonferroni correction to minimize the possibility of a type I error. Significance was set at the P < .002 level for this investigation with this correction.
Results
All 153 participants in this study were male, with a mean age of 25.6 ± 3.57 years. Most (84.3%) of the participants were right-handed, and most (81.5%) had a 2-handed backhand. Visually observed dominant-arm infraspinatus atrophy was present in 92 of the 153 participants (60.1%), with only 1 of the 153 participants (0.7%) demonstrating infraspinatus atrophy on the nondominant arm.
Pearson correlations showed several significant findings, detailed in Table 1. Dominant-arm infraspinatus atrophy was negatively correlated with dominant-arm external rotation strength in neutral abduction/adduction (at the side), as well as with both dominant- and nondominant-arm external rotation strength at 90° of abduction. These were the only 3 parameters with any significant correlation with visually observed infraspinatus atrophy on the dominant shoulder. No relationship was found with shoulder internal, external, or total rotation ROM; horizontal adduction (cross-body) ROM; or scapular dyskinesis.
Pearson Correlation Summary of Infraspinatus Atrophy and Objectively Measured External Rotation Strength

Independent t tests showed no significant difference in ROM measures, age, weight, or ranking between players with visually observed dominant-arm infraspinatus atrophy (n = 92) and those without (n = 61). Table 2 summarizes these parameters for both groups of players. A significant difference in external rotation strength on the dominant shoulder in neutral (abduction/adduction) (P = .001) was noted, with a mean deficit of approximately 1.5 kgf (12.2%) in the group with dominant-arm infraspinatus atrophy versus without. Differences in external rotation strength at 90° of abduction by 1 kgf were noted between players with and without dominant-arm infraspinatus atrophy, however these were not statistically significant.
Comparison of Testing Variables Between Players With and Without Visually Observed Infraspinatus Atrophy a
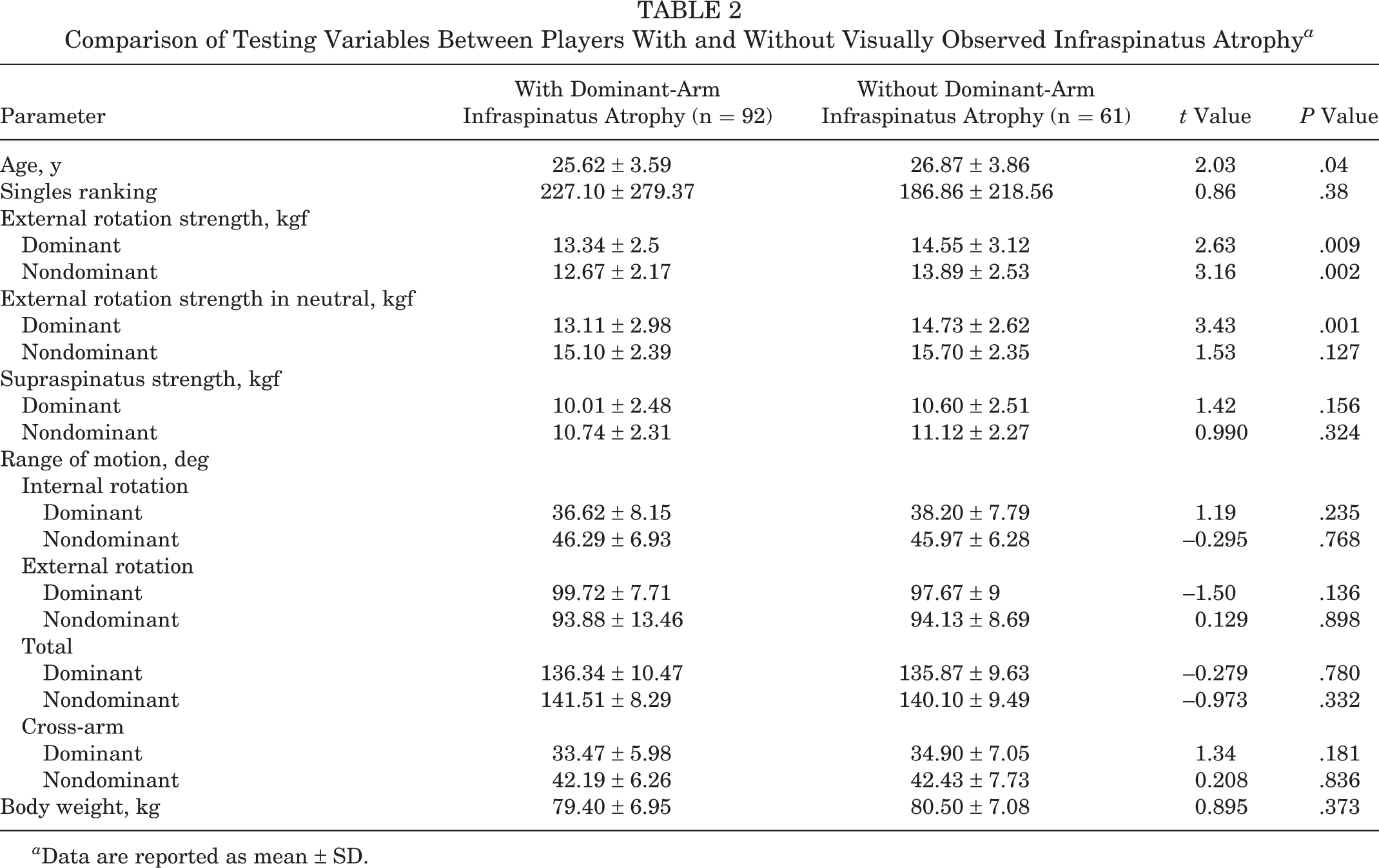
a Data are reported as mean ± SD.
Discussion
This study found visually observed infraspinatus atrophy in the dominant extremity of 60.1% of elite male professional tennis players. The finding of dominant-arm infraspinatus atrophy also negatively correlated with external rotation strength both in neutral position (0°) and 90° of abduction. Young et al 52 previously reported a very high prevalence of dominant-arm infraspinatus atrophy (52%) in female professional tennis players on the WTA Tour. This high prevalence reported in professional female tennis players is in agreement with our finding in male players on the ATP Tour. Before these studies in tennis, volleyball players had the highest prevalence of infraspinatus atrophy in the sports medicine literature, ranging between 13% and 34%. 17,21,28,29,44,51
In addition to determining the prevalence of unilateral dominant-arm infraspinatus atrophy in male professional tennis players, the present study also sought to determine whether infraspinatus atrophy had any correlation with other shoulder measures evaluated during a preventive musculoskeletal screening. Consistent with prior studies in the literature, no physical examination finding (scapular dysfunction, glenohumeral joint ROM measurement, supraspinatus strength) other than dynamometer-measured external rotation strength was correlated with the finding of infraspinatus atrophy on the dominant extremity. 39,40 A comparison of external rotation strength in neutral abduction/adduction at the side between players with and without infraspinatus atrophy revealed a significant deficit of approximately 1.5 kgf (12.2%) (P = .001). In a study of professional female tennis players, Young et al 52 did not use objective dynamometer testing for external rotation strength but did state that 11% of players in their sample had external rotation weakness with manual muscle testing. Lajtai et al, 29 examining a sample of 35 male professional beach volleyball players, reported significantly lower external rotation strength on the dominant side (12.9 kg) compared with the nondominant side (14.3 kg). Those investigators reported that the players in their sample with dominant-arm infraspinatus atrophy (n = 12) had significantly less (P < .05) external rotation strength than in their contralateral extremity, similar to this investigation; however, Lajtai et al did not provide actual values for the deficit in external rotation strength between players with and without dominant-arm infraspinatus atrophy. The present study showed a statistically significant correlation between dominant-arm infraspinatus atrophy and objectively measured external rotation strength, as well as a significant difference in external rotation strength when comparing players with versus without dominant-shoulder infraspinatus atrophy. The finding of a significant correlation between visually observed atrophy and external rotation weakness at both 0° of abduction/adduction and 90° of abduction can be explained by high levels of muscular activity of the infraspinatus in both positions. Gerber et al 20 found that the infraspinatus was the main external rotator in all positions of abduction, with the teres minor contributing <20% to force development at any position of abduction. Therefore, the finding of a significant correlation both in neutral abduction/adduction (0°) and in 90° on the dominant arm when dominant-arm infraspinatus atrophy was present can be explained by the key role the infraspinatus plays in both positions of external rotation. The reason for the significant correlation between dominant-arm infraspinatus atrophy and nondominant external rotation strength at 90° of abduction is unclear.
Several studies 9,36,37,39,40 have highlighted the close anatomic relationship between the spinoglenoid ligament and the posterior capsule of the shoulder. These reports theorized that the glenohumeral joint position during the follow-through phase of the overhead throwing or serving motion (adduction and internal rotation) could produce tightening of the ligament through the posterior capsular attachments and result in compression of the suprascapular nerve. Our study of male professional tennis players did not find any correlation between internal rotation ROM, total rotation ROM, or cross-arm adduction ROM and visually apparent dominant-arm infraspinatus atrophy. Additionally, we found no significant difference in any of these ROM values between the players with and without infraspinatus atrophy. This is in agreement with the findings of Young et al 52 in professional female tennis players and Reeser et al 39,40 in elite volleyball players. Those studies did not identify a relationship between internal rotation ROM loss and infraspinatus atrophy.
A theory proposed by Sandow and Ilic 45 suggests that the position of abduction and external rotation (cocking phase) results in physical compression of the suprascapular nerve at the spinoglenoid notch. Because the tennis serve produces less external rotation than the throwing motion in baseball, 19 this would contradict the reported prevalence research; a relatively lower prevalence of dominant-arm infraspinatus atrophy was shown in baseball pitchers (4%) by Cummins et al 7 compared with those found in male and female 52 professional tennis players.
The common finding of dominant-arm infraspinatus atrophy in professional tennis players and its correlation with external rotation weakness indicates a possible need for external rotation strengthening interventions. Weakness of the external rotators and, specifically, decreases in the ratio of external to internal muscle strength have been linked to shoulder injury in professional overhead athletes. 2 The fact that infraspinatus atrophy appears to be a common finding in both male and female professional tennis players should alert clinicians who evaluate these athletes and provide guidance and a rationale for the addition of external rotation strengthening programs to prevent injury. This simple screening, entailing visual observation and bilateral comparison of the soft tissue bulk inferior to the scapular spine in the overhead athlete, can assist clinicians during clinical evaluation or preventive screening assessments.
A limitation of this study is that we did not objectively measure suprascapular nerve function with electrophysiologic testing. Additionally, we used visual observation alone to identify infraspinatus atrophy. No additional imaging was done to validate the visual appearance of hollowing as a true measure of muscle atrophy or to quantify the degree of atrophy. The method used in this study was similar to that used in both clinical and athletic medicine settings. Future studies in overhead athletes could provide additional confidence and validate our findings by using imaging modalities to objectively quantify muscle volume and comparing it bilaterally in this population to ensure that visible infraspinatus atrophy is not due to hypertrophy of dominant-arm periscapular musculature in overhead athletes.
This study identified dominant-arm infraspinatus atrophy as a common finding in male professional tennis players. Dominant-arm infraspinatus atrophy is easy to identify through visual observation as used in this study. Clinicians who find infraspinatus atrophy should perform testing to determine whether shoulder external rotation weakness is present. The finding of external rotation weakness should result in the implementation of specific interventions to improve external rotation strength and muscular endurance.
Conclusion
Visual observation of the scapula in a sample of 153 male professional tennis players identified apparent infraspinatus atrophy in 92 players (60.1%) on the dominant extremity. Additionally, the finding of dominant-arm infraspinatus atrophy was significantly correlated with external rotation strength in both the neutral and the 90° abducted positions. No other significant correlations were identified between infraspinatus atrophy and glenohumeral joint internal rotation and horizontal cross-arm adduction, as well as scapular dyskinesis. Based on the results of this study, the finding of dominant-arm infraspinatus atrophy is common in elite-level tennis players but, given the correlation with external rotation weakness, may indicate the need for focused external rotation strengthening and clinical monitoring.
Footnotes
Final revision submitted April 10, 2020; accepted April 22, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.M.D. has received royalties from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Physiotherapy Associates (registration No. IRB00010155).