
Abstract
BACKGROUND:
Rate of torque development (RTD) could serve as a useful index for the readiness and fatigue of soccer players.
OBJECTIVE:
The identification of RTDs time-course changes after a Loughborough Intermittent Shuttle Test (LIST), the effect of bovine colostrum (BC) supplementation on RTD changes, and to explore the relationships between RTD and selected muscle damage blood markers.
METHODS:
Twenty-two soccer players completed a pre-supplementation LIST (LIST1). Subsequently, subjects were randomly divided into whey protein (WP,
RESULTS:
RTD declined after LIST1 (
CONCLUSIONS:
LIST induces a significant decline in RTD of soccer players. BC could be a promising supplement alleviating the impairment of RTD after a soccer game.
Keywords
Introduction
Soccer is a very demanding, high intensity, form of intermittent physical activity. Elite players cover about 9–12 Km/game. Two to three Km are covered at high intensities as well as about 500 m of sprinting [1]. Soccer players frequently perform repetitive explosive movements, with strong eccentric components, leading to exercise performance decrements and increased fatigue [2, 3]. Competitive soccer matches cause exercise induced muscle damage (EIMD), neuro-muscular and neuro-mechanical alterations, inflammation and oxidative stress [3, 4, 5, 6] which are slowly reversed during the post-match period, but they remain impaired up-to 72 h post match [1, 2, 4, 5, 7, 8]. Elite soccer players frequently experience a very busy schedule, including 2–3 matches/week and several training sessions/week, which do not allow full recovery after a match or a training session [9]. This can increase the risk and rate of injuries, while player’s fitness and performance decrease during the competition period [8]. It is therefore obvious that easy, reliable, objective, cost-effective and accurate methods of recovery monitoring is of high interest for both sports scientists and professionals.
Several studies investigated the time course of players’ performance and EIMD during their recovery period after real or simulated of soccer matches. A recent meta-analysis highlighted the importance of monitoring players’ performance (especially through countermovement jump; CMJ) along with biochemical and perceptual indices [6]. Indeed, biochemical indices provide direct evidence about the physiological status/stress and time course of muscle damage, while the evaluation of CMJ could inform about the functionality and the readiness of players. Repetitive evaluation of muscle damage is beneficial to soccer teams but can only provide evidence for the peripheral factors of fatigue or EIMD. However, it not assesses neural and/or neuromuscular system fatigue. In contrast CMJ performance could provide evidence of the status of neuromuscular readiness, but post-match changes of CMJ performance are small and do not always follow or represent changes to the EIMD markers [6]. In addition, there are two studies indicating the use of maximum isometric force or Torque (MIF or MIT) [10] as an alternative indirect method to monitor players’ readiness [6]. In contrast, it was recently proposed that the rate of force or torque development (RFD or RTD respectively) can estimate in a more specific and sensitive manner EIMD [11]. It was proposed that RFD depends on numerous biological factors, in a time dependent manner, including muscle size, neural function, muscle activation, fiber type composition, muscle-tendon mechanics and architecture, while MIT depends highly on muscle size, function and cross sectional area of muscle fibers [12, 13, 14, 15]. In addition, the above biological factors, seem to affect differentially the RTD performance depending on the examined time interval from the onset of muscle contraction. Specifically, early RTD, eg. the RTD from the onset of muscle contraction until the first 100 ms of the effort, seems to depend mainly on the neural system function, and at least in power-trained athletes by the percentage area (%CSA) of Type II, and especially Type IIx, muscle fibers [12, 13, 14, 15]. In contrast, late RTD (
Bovine colostrum (BC) is the first milk produced by the mammary glands of the mother during the final days of pregnancy and the first days postpartum (1–4 days). It is a natural, multi-ingredient supplement and recent studies support its protective role against exercise-induced immune decline [18, 19] and gut permeability [20]. Despite its wide use as a recovery supplement, no strong evidence supports this action. Recent work at our laboratory showed a low-dose, 6-week bovine colostrum (BC) supplementation maintains performance and attenuates inflammatory indices following a Loughborough Intermittent Shuttle Test (LIST) in soccer players [7]. Animal models demonstrated the ability of colostrum supplementation to protect against oxidative stress in muscle [21] while colostrinin, a proline-rich polypeptide complex found in colostrum, has strong antioxidant and immunomodulatory properties [22]. However, whether this effect could also improve neuromuscular function, either directly or indirectly, is not known.
Participants characteristics and baseline values for LIST1 and 2
Participants characteristics and baseline values for LIST1 and 2
Values are mean
Thus, the aim of the present study was to identify the time-course changes of RTD and explore the relationships between time-course changes of RTD and selected EIMD blood markers, up to 72 hours post LIST. In addition, the present study aims to investigate the effect of a low-dose, short-term BC supplementation on post-LIST RTD and EIMD blood markers responses. We hypothesized (1) LIST induced fatigue would lead to a significant reduction of RTD performance up to 2 hour post LIST, (2) the extent of muscle damage, will be associated with the decline of RTD after LIST, and (3) BC could attenuate the post-LIST RTD decrements.
Participants
Twenty-two players completed the pre-supplemen- tation LIST1 (Table 1). Then they were allocated to either the whey protein group (WP,
Experimental design.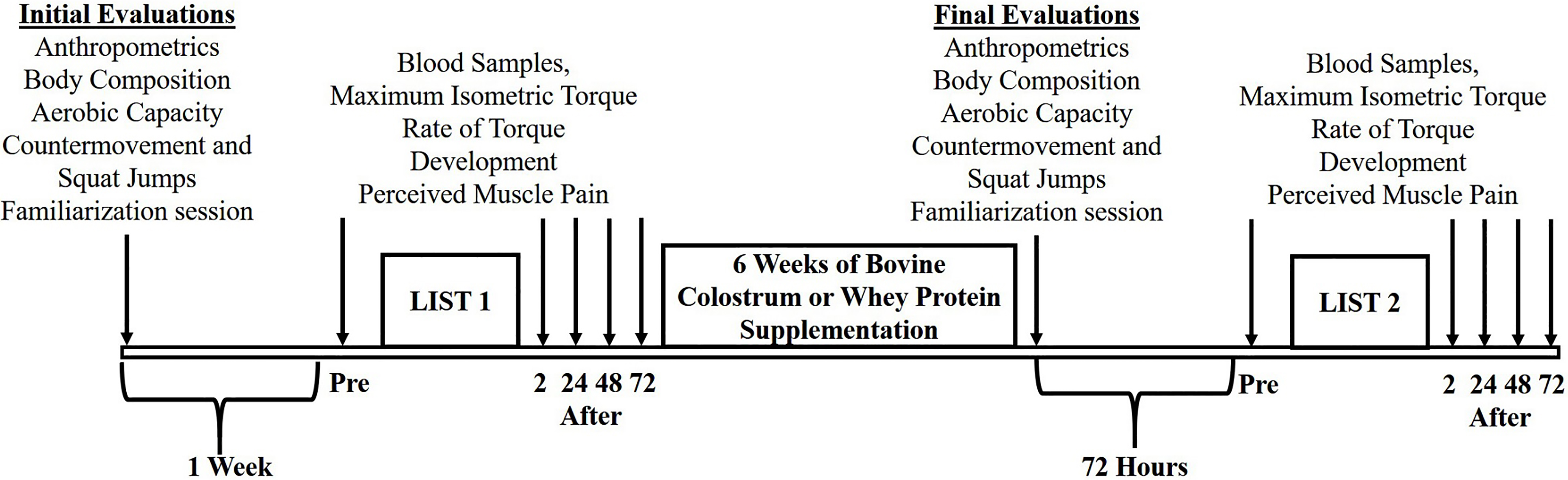
The study had a double-blind, randomized, placebo-controlled, parallel group, design which was previously described in detail [7]. Here, we present the data on the kinetics of early and late RTD after LIST, the associations between the percent changes of RTDs and the respective changes of muscle damage and inflammation indices, and finally the effect of bovine colostrum supplementation on RTDs kinetics. In brief, participants were recruited via advertisements in soccer clubs of the Greek National league third and fourth division. Responders visited the laboratory where they completed the necessary medical and health questionnaires and had a medical examination by a trained physician. Twenty-two players of the third and fourth division of the Greek National league were recruited according to the following criteria: at least eight years of systematic soccer training, active participation at national league games, absence of orthopaedic/neuromuscular maladies, age range between 18 to 35 years and absence of drugs abuse or medications. During their first visit to our laboratory participants signed the informed consent form while anthropometric measurements, body composition analysis, cardiopulmonary assessment and familiarization with all the performance evaluations of the present study took place. Two days later, countermovement and squat jump performance were evaluated. A week later they completed the pre-supplementation LIST (LIST1) and muscle damage indices, leg extension RTD and maximum isometric torque (MIT) performances were monitored for 72 h post-exercise. Participants reported to the laboratory between 07:00 and 08:00 am after an overnight fast. A resting blood sample was taken and muscle strength-RTD were measured. Afterwards, subjects consumed a standard meal giving approximately 397 Kcal; 59 g carbohydrates, 11 g fat, 15 g protein [7]. After 1 hour from the initial (baseline) evaluation, each participant performed LIST1. EIMD biochemical markers, muscle performance and perceived muscle pain were evaluated before, 2, 24, 48 and 72 h post LIST. Participants who successfully completed LIST1 were randomly allocated to either whey protein (WP) or BC group receiving 3.2 g
Supplementation
Participants of the BC group received 3.2 g
Loughborough Intermittent Shuttle Test
The 90-min shuttle run test was conducted according to Thompson et al. on an artificial surface soccer pitch [23]. Volunteers were required to run between two lines, 20 m apart, at various speeds dictated by an audio signal based on the velocities corresponding to their individual 55% and 95% of VO
Anthropometric and body composition measurements
A total body scan was performed with dual energy x-ray absorptiometry [DPX-L; LUNAR Radiation, Madison, WI, USA; ICCs ranged between 0.85 and 0.98 [13].
Cardiopulmonary assessment
The players performed an incremental (0.5 km
Percentage changes from the baseline evaluations and incremental area under the curve (iAUC; absolute values) of maximum isometric torque, rate of torque development, hematological and inflammatory blood markers, until 72 hours post LIST1 (
22)
Percentage changes from the baseline evaluations and incremental area under the curve (iAUC; absolute values) of maximum isometric torque, rate of torque development, hematological and inflammatory blood markers, until 72 hours post LIST1 (
Values are mean
Squat jump (SQJ) and countermovement jump (CMJ) tests were conducted using a photocell device (Optojump, Microgate, Italy) according to previous reports [25, 26]. Individuals started with a five-minute warm up on a stationary bicycle and five minutes of stretching of the lower extremities’ major muscle groups. Then three countermovement jumps with submaximal but progressively higher intensity were performed. Subsequently three maximal efforts for each jumping technique, with hands placed on hips, were performed, with two minutes of rest between attempts. Jumping height was automatically calculated. The best effort was used for analysis. The ICC for the SQJ and the CMJ were 0.90, (95% CI: Lower
Evaluation of maximum isometric torque and rate of torque development
All subjects performed a specific submaximal protocol on an isokinetic dynamometer (BIODEX System 3 Pro, NY, USA; sampling frequency 100 Hz) to familiarize themselves with the isokinetic device and test procedure. Knee angle was set at 90
Blood sampling and biochemical assays
Venous blood samples were obtained from each subject. Complete blood count was determined in EDTA anticoagulated whole blood with a Mindray BC-3000 hematology analyzer (Mindray, Shenzhen, China). The activity of creatine kinase (CK) was determined spectrophotometrically by a commercially available kit (Biosis, Athens, Greece) modified for 96-well plates according to manufacturer’s instructions. High-sensitivity C-Reactive Protein (CRP) and Interleukin 6 (IL-6) were determined in serum by commercially available ELISA kits (Quantikine, R&D Systems, Abingdon, UK).
Statistical analyses
All data are presented as means and standard deviation (
Results
Acute effect of LIST
The first part of this study examined the effect of LIST on RTD. For this reason, we conducted a pooled analysis from the data obtained after LIST1 (pre-supplementation LIST). The group of this analysis included the volunteers of WP and BC groups along with the volunteers who successfully completed LIST1 but dropped out from LIST2 (Table 1). Both early (0–100 ms from the onset of muscle contraction) and late (
Pearson’s correlation coefficients and adjusted R squared (in parentheses) between maximum oxygen consumption, lower extremities lean body mass, baseline rate of torque development (RTD) and incremental area under the curve (iAUC) of RTDs until 72 hours post LIST1. Only significant correlations are presented
Pearson’s correlation coefficients and adjusted R squared (in parentheses) between maximum oxygen consumption, lower extremities lean body mass, baseline rate of torque development (RTD) and incremental area under the curve (iAUC) of RTDs until 72 hours post LIST1. Only significant correlations are presented
(
RTDs percentage changes from the baseline evaluations after LIST1. 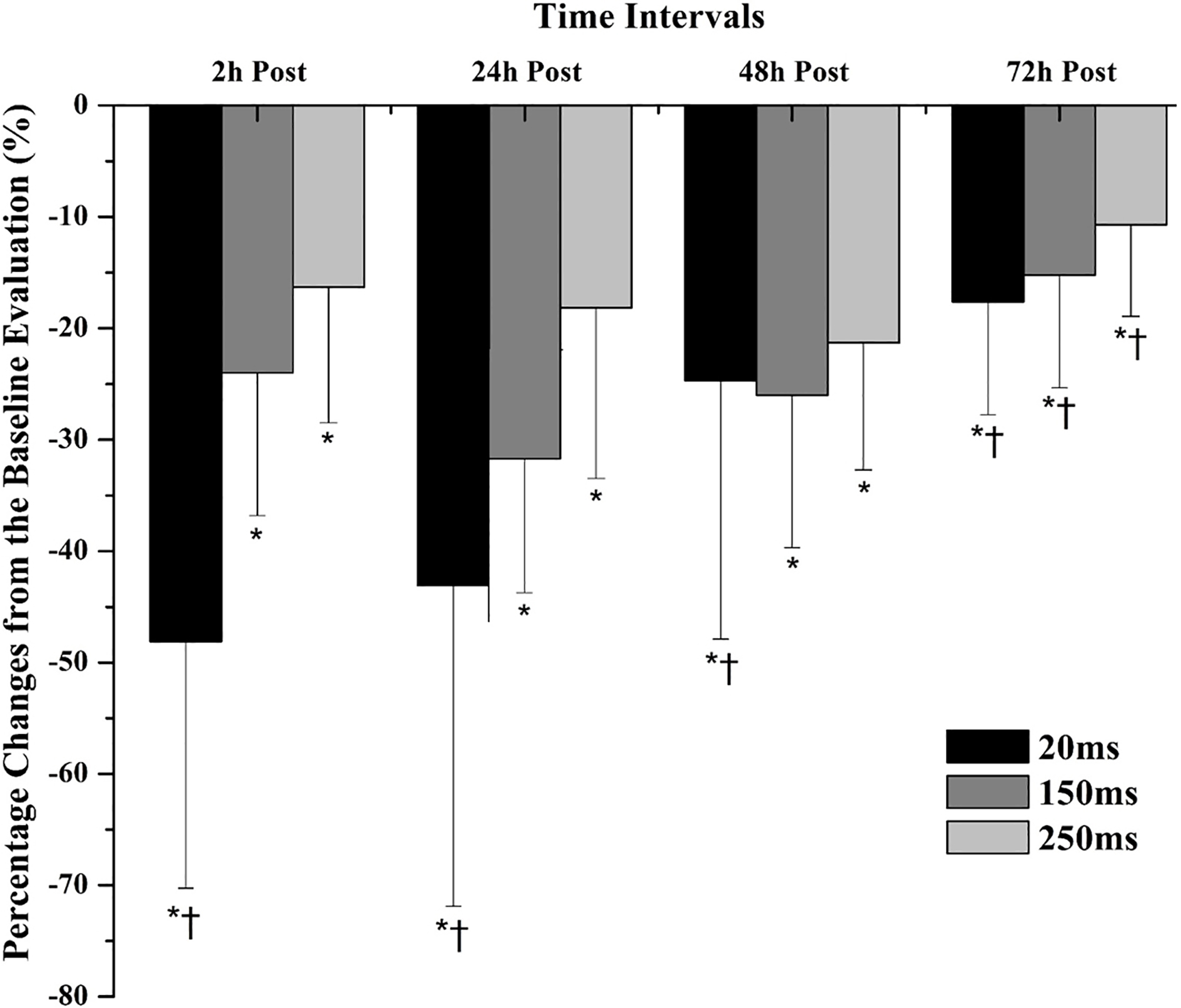
In addition, LIST1 induced a sustained decrease of MIT 2–48 h post LIST1. It also induced CK and CRP significant elevations up to 72 h, reaching their highest percentage changes at 24 h (CK: 252.8
Pearson’s correlation coefficients and adjusted R squared (in parentheses) between iAUCs of RTD and Creatine kinase, Interleukin-6, C-reactive protein (
IL-6: Interleukin-6; CRP: C-reactive protein; CK: Creatine kinase. (
Correlation plots between A) maximal oxygen consumption and iAUC of RTD at 250 ms, B) baseline RTD at 150 ms and iAUC of RTD at 150 ms and C) iAUC of CRP and iAUC of RTD at 150 ms, after LIST1.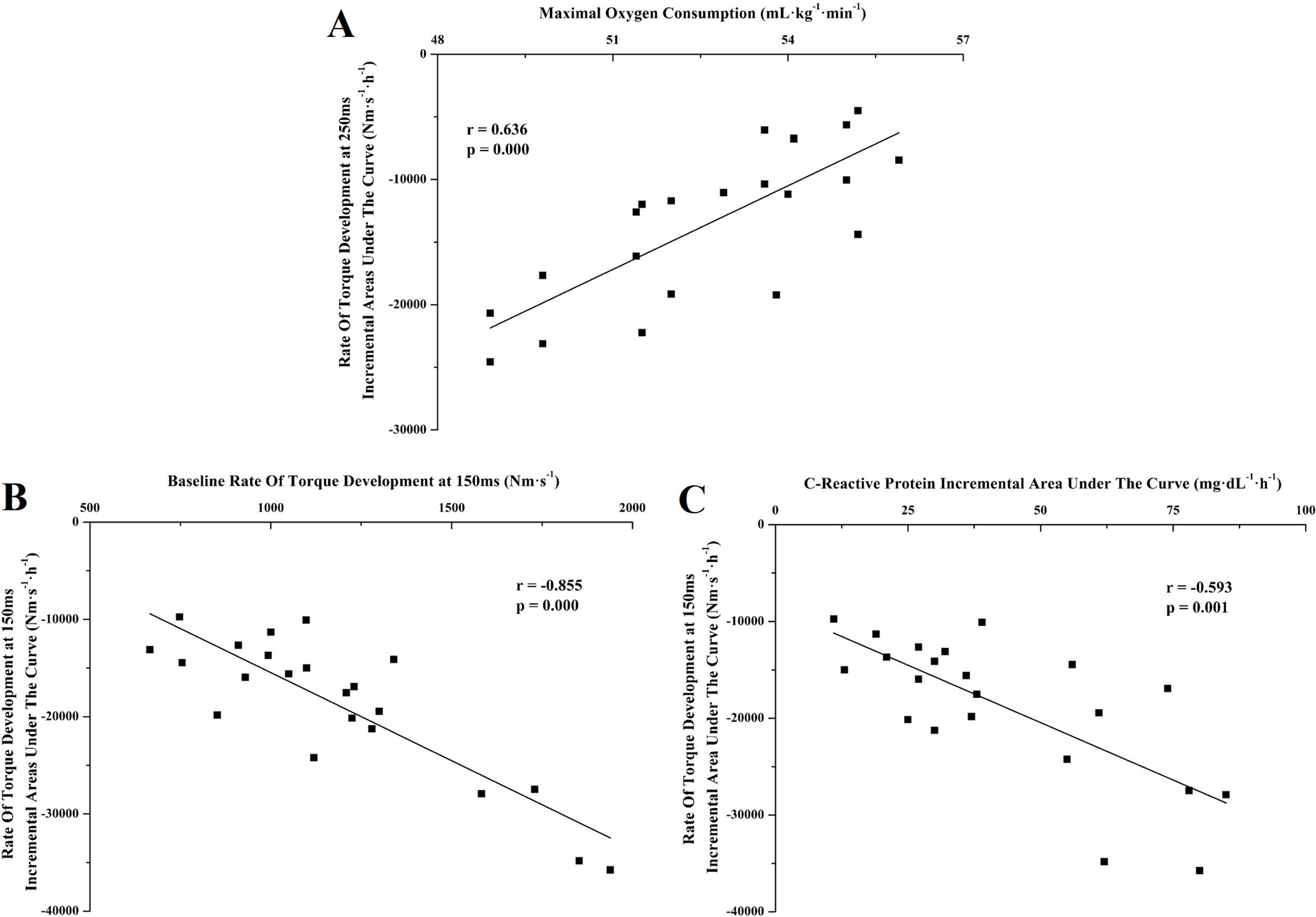
Pre LIST1 maximum oxygen consumption was positively correlated with both early and late (80–250 ms) RTD iAUC (
Percentage changes from the baseline evaluations after LIST1 and 2 for rate of torque development at 150 ms, for both groups. 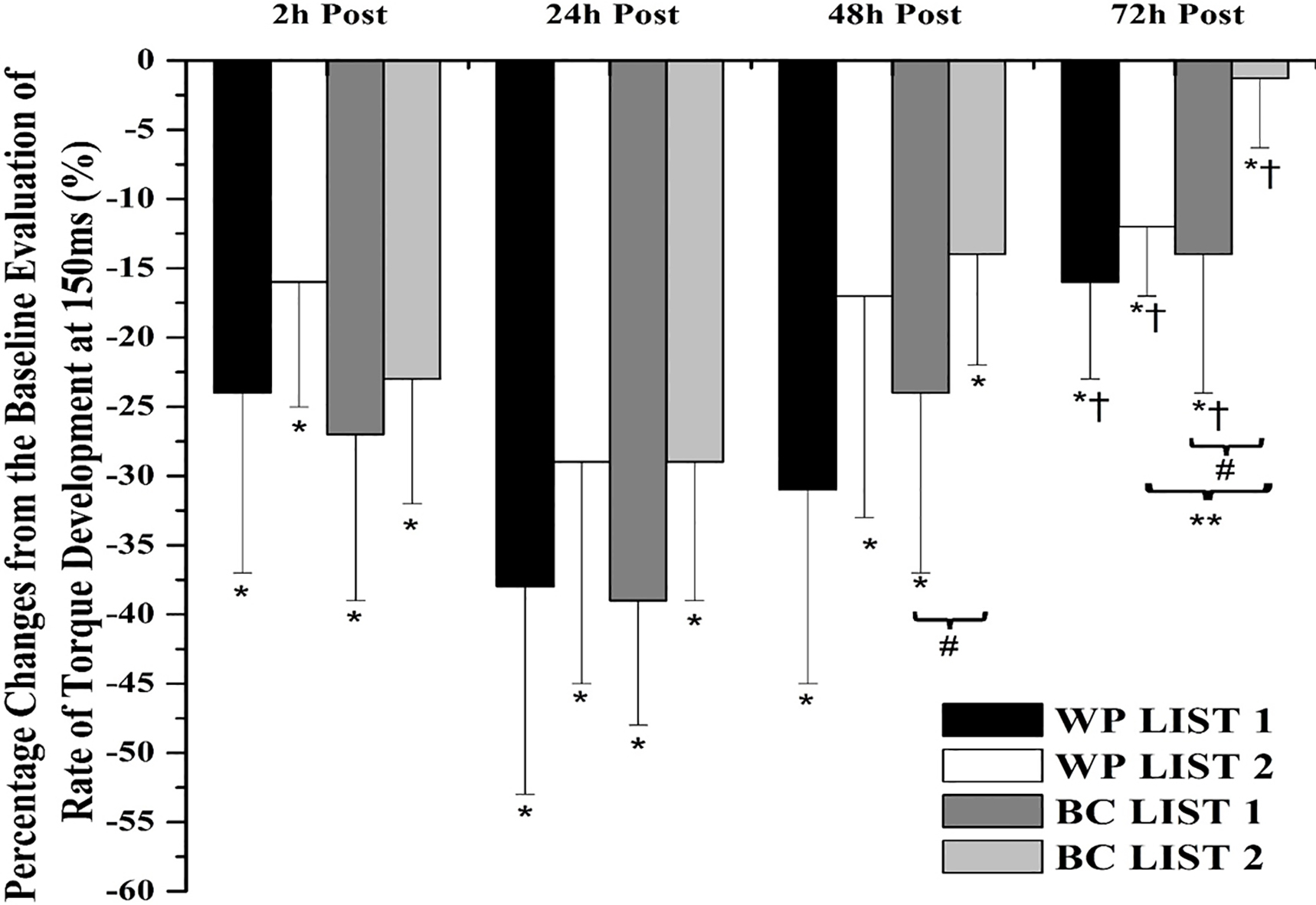
In an effort to identify whether the magnitude of alterations in EIMD and inflammation markers induced by LIST correlate with the degree of RTD decline, we proceeded to correlation analyses between the iAUCs of the aforementioned variables. Significant negative correlations were found between the iAUCs of both early and late RTD and those of creatine kinase, interleukin-6 and C-reactive protein (Table 4 and Fig. 4C). Partial correlation analysis revealed both VO
Effect of WP and BC supplementation on RTD changes after LIST
The baseline values of performances and blood biochemical indices, of both LISTs and Groups, are presented in Table 1. No significant differences were found either between or within the two groups for the baseline evaluations in any trail (
Supplementation of either WP or BC did not affect significantly the percentage changes of early RTD until 72 h post LIST2 compared to those of post LIST1. The only significant differences were found for the late RTD percentage changes, and only at 48 and 72 h post LISTs (
The changes of the absolute values of hematological and inflammatory markers were presented previously [7].
Discussion
The main findings of the present study were that: a) RTD is highly affected by LIST, showing a decline up to 72 hours post LISTs, b) its negative changes are related to the responses of selected muscle damage and inflammatory blood markers c) low doses of either WP or BC, have a positive effect on post LIST RTD reductions up to 72 h post testing, thus shortening the recovery period and d) BC has a somewhat larger positive effect compare to WP (no significant differences between them). The results of our study provide strong evidence that evaluation of RTD post LIST, and proba-
Percentage changes from the baseline evaluations of RTDs and MIT, until 72 hours post LIST1 and 2, for both Whey Protein (WP;
8) and Bovine Colostrum (BC;
10) groups
Percentage changes from the baseline evaluations of RTDs and MIT, until 72 hours post LIST1 and 2, for both Whey Protein (WP;
Values are mean
bly post-match, is a very specific and sensitive estimation of muscle damage-muscle function. Furthermore, it may provide significant information to sports scientists and professionals about the readiness of their players, for either a training session or a match.
RTDs significantly declined up to 72 h post LIST. These decrements were greater than those of MIT at the same time-intervals, providing further support to a previous study [11]. Almost identical reductions of RTD performance, either during [16] or immediately after [17] a match or a match-simulation, were previously reported. However, the current study provides time course RTD reductions up to 72 h post LIST in trained semi-professional soccer players for the first time. As it was previously described, RTD/RFD performance depends on several biological and mechanical properties, including muscle size and activation, fiber type composition, muscle-tendon mechanics and architecture [12, 13], as well as the muscle fibers
metabolic function [30]. In contrast MIT depends highly on muscle size, function and cross sectional area of muscle fibers [12, 13]. It is well established, that after a soccer match or a soccer simulation trial, all the above parameters are strongly and negatively affected for up to 72 hours thereafter [6], with interplay between peripheral and central fatigue mechanisms [2, 5, 6, 31].
The greater reductions in RTD were observed at the early stages of the onset of muscle contractions, at least for the first 24 h after the interventions. The function of the nervous system, which seems to be the major determinant of early RTD/RFD [11, 12, 28, 29], is highly impaired after a soccer or a soccer simulation trial, with the greatest reductions observed 24 hours post-intervention [6, 16, 17, 31]. In support of this finding, it was suggested that reductions in force/power production capability, after an eccentric exercise, are primarily affected by the failure of muscle fibers excitation and contraction mechanisms, and less to the generation and mechanical transmission of muscle force [32]. Furthermore, previous studies reported soccer or soccer simulation trials-induced decrements in RFD (until the first 24 h post interventions) were accompanied by similar reductions of neural function [16, 17]. Thus, these reports, can partly explain the stronger reductions of early RTD at 2 and 24-hour post LISTs seen in the current study.
Excluding the central-related fatigue theory, a wide spectrum of peripheral factors, including muscle fibers, metabolic, structural and biochemical alterations, that occur after a match or a simulated play [2, 3, 5, 6, 17, 31] also strongly impair RTD performance by affecting directly or indirectly, muscle fiber homeostasis, regulation and function. In turn the mechanical properties of muscle fibers which determine rapid force production and thus early RTD performances, are also impaired leading to reduced force generation, transmission and rapid force production [28, 30]. We also observed significant correlations between the changes of selected blood inflammatory and EIMD markers (like IL-6, CRP, CK) to those of early RTD performance, indicating LIST-induced EIMD also has a significant contribution to the reduction of early RTDs. Taken together all the above, it could be hypothesized the stronger reductions of early RTD performances, at least as they observed until the first 24 h post LISTs, are a result of both LIST-induced neural and muscle perturbations.
In contrast to early RTD performance, late RTD showed smaller declines after LIST. These reductions were almost stable until 72 h post LIST, compared to those of early RTD. Late RTD is thought to be determined primary by the muscle size and function [11, 12, 13]. Significant LIST-induced muscle damage should lead to all the structural and metabolic dysfunctions of muscle fibers that were described previously, and thus should have greater impact on the later RTD performances. Indeed, previous studies report late RTD performance reflects more the kinetics of cross-bridge mechanism, which is strongly affected by the structural and metabolic dysfunctions of muscle fibers, after EIMD [11, 30]. In support of this idea stronger correlations were observed between the iAUCs of blood markers and those of late RTDs, as compared to those of early RTDs. According to these observations and reports it may be concluded that late RTDs are mostly affected by dysfunction and alterations of muscle fibers structure. Thus, players with lower muscle damage can achieve better late RTD performance. Several studies on this subject, investigated the use of maximum isometric force or Torque (MIF or MIT) as an alternative indirect method for monitoring players’ readiness [6, 10]. However, as it was previously described [11] and also verified in the present study, the assessment of RTD performance is a more specific and sensitive indirect estimation of EIMD than MIT, while it could provide important information about the status and the readiness of both neural and muscular systems for at least 72 h after a soccer match.
We also wanted to investigate whether low dose, long term BC supplementation could affect the kinetics of RTD after LIST. In an effort to avoid the possible interference of a repeated bout effect on our results, trained soccer players were selected. It is generally accepted repeated bouts of the same training stimuli lead to very specific muscle adaptations that protect from extensive muscle damage [33]. In addition, to avoid repeated bout effect, the intervention was familiar to soccer players. Thus LIST was selected, which simulates the activity pattern of a real soccer match, and induce the same muscle damage and neuromuscular fatigue as those in their weekly soccer matches [34].
Unfortunately, we couldn’t monitor the training and game loads of each participant during the supplementation period because our subjects belonged to different teams. However, since no significant differences were found between and within groups for all measured variables (anthrpometric, body composition, aerobic fitness, jumping, RTD, hematological and biochemical) at the initial evaluations prior to LIST1 and 2 (
Our BC and WP doses were significant lower than those usually recommended for either protection against EIMD and/or faster recovery [35, 36, 37, 38]. However it was recently suggested, a dose of BC similar to that of our study, could protect against exercise-induced oxidative stress in rats [21]. We also considered the relatively high cost of BC and whether a long term, low dose dosage scheme could be efficiently in modulating post-LIST EIMD and neuromuscular function. Finally, even if BC is not prohibited by WADA, and it doesn’t seem to raise IGF-1 levels [39] we couldn’t rule out the possibility that significantly higher amounts of BC per day for six weeks would influence the outcome of typical anti-doping test.
The comparison of RTD kinetics before and after WP and BC supplementation showed lower declines post supplementation in both BC or WP groups. The highest differences were observed for late RTD and after 24 h. In addition, the lower changes of RTD performance at these time intervals, were accompanied by an equally lower change of muscle blood inflammation markers, indicating both nutritional interventions protected against muscle damage, with a trend favoring to BC. Early RTD seems to be less affected from BC and WP supplements than late RTD, while the highest positive effects of the two supplementations were found 24 h post LIST2. The weaker effect of BC and WP on early RTDs were expected, since early RTD is affected primary from the function of the nervous system. It is well known, that the positive effects of both BC and WP on muscle function and force/power generation capacity, by suppressing EIMD [7, 40, 41, 42, 43, 44], while a positive effect on the neural system has never been reported. A low dose of WP over a normal player’s daily protein intake, is expected to cause an additional increase in muscle protein synthesis which can lead to a greater and faster muscle remodeling, at least after extensive resistance training [36, 40, 41, 43]. In addition it seems to depress concentrations of blood inflammation markers, confer antioxidant protection and augment the recovery of muscle function, probably through an essential amino acid mechanism [36, 40, 41, 42, 44, 45]. In addition to the properties of WP, BC contains bioactive nutrients and microconstituents with antimicrobial and immunomodulatory properties [37]. As a consequence, lower changes of post-LIST IgG2, salivary IgA and lysozyme [37], neutrophils degranulation [37] and protection against exercise-induced gut hyper-permeability [46] are expected, leading to less suppression of immune system. Additionally, BC has been reported to elevate resting levels of essential and branched-chain amino acids [47]. It also protects epithelial integrity and attenuates gut permeability partly by reducing temperature-induced apoptosis of epithelial cells and induction of the cytoprotective heat-shock proteins [46]. While, in rats, it was found to increase the specific activity of superoxide dismutase and of total antioxidant capacity [21]. It is concluded that both BC and WP have a protective capacity against the LIST-induced muscle damage, minimizing and/or shortening the alterations of metabolic and mechanical properties of muscle which control the extent of the damage by accelerating the remodeling process to produce less RTD reductions and faster recovery times. The trend observed in the present study, in favor to BC, may be the result of its aforementioned actions. However, the exact mechanisms underlying the ability of BC to affect the recovery process after one bout of exercise are still speculative, and further research is needed.
The present data suggest evaluation of RTD after LIST is a very specific and sensitive estimation of muscle damage-function, which may provide significant information to sports scientists and professionals about the readiness of their player. Six weeks of a low dose of WP and especially BC supplementation, have positive effect on LIST induced muscle damage and RTD decline shortening the recovery period and augmenting players’ performances.
Footnotes
Acknowledgments
The study was partially funded by LR Health and Beauty Systems. The study was investigator initiated and the sponsor had no involvement in the design and conduct of the study neither in the collection, management analysis and interpretation of the data nor in the preparation, review or approval of the manuscript.
Conflict of interest
Yiannis Kotsis worked as a part time scientific consultant for LR Health and Beauty Systems at the time of the study. All authors report no conflict of interest.