
Abstract
Background:
The relationships between hip abductor and extensor strength and frontal plane hip and knee motions that are associated with anterior cruciate ligament injury risk are equivocal. However, previous research on these relationships has evaluated relatively low-level movement tasks and peak torque rather than a time-critical strength measure such as the rate of torque development (RTD).
Hypothesis:
Females with greater hip abduction and extension RTD would exhibit lesser frontal plane hip and knee motion during a single-leg jump-cutting task.
Study Design:
Descriptive laboratory study.
Methods:
Forty recreationally active females performed maximal isometric contractions and single-leg jump-cuts. From recorded torque data, hip extension and abduction RTD was calculated from torque onset to 200 ms after onset. Three-dimensional motion analysis was used to quantify frontal plane hip and knee kinematics during the movement task. For each RTD measure, jump-cut biomechanics were compared between participants in the highest (high) and lowest (low) RTD tertiles.
Results:
No differences in frontal plane hip and knee kinematics were identified between high and low hip abduction RTD groups. However, those in the high hip extension RTD group exhibited lower hip adduction (high, 3.8° ± 3.0°; low, 6.5° ± 3.0°; P = .019) and knee valgus (high, –2.5° ± 2.3°; low, –4.4° ± 3.2°; P = .046) displacements during the jump-cut.
Conclusion:
In movements such as cutting that are performed with the hip in a relatively abducted and flexed position, the ability of the gluteus medius to control hip adduction may be compromised. However, the gluteus maximus, functioning as a hip abductor, may take on a pivotal role in controlling hip adduction and knee valgus motion during these types of tasks.
Clinical Relevance:
Training with a specific emphasis on increasing explosive strength of the hip extensors may be a means through which to improve frontal plane hip and knee control during high-risk maneuvers such as cutting.
Keywords
Excessive hip adduction and knee valgus motion is proposed as a common risk factor for a variety of acute and overuse lower extremity injuries, including anterior cruciate ligament (ACL) sprain, 14,18 patellofemoral pain syndrome, 11,39 and iliotibial band friction syndrome. 10 As a result, substantial research has been geared toward identifying modifiable factors that can influence frontal-plane hip and knee motion such that they might be targeted in primary prevention or rehabilitation programs.
One common intervention to minimize knee valgus motion is to focus on controlling hip adduction, as greater adduction is associated with increased knee valgus angles during athletic movements. 26 The hip muscle most often targeted clinically to control the magnitude of hip adduction is the gluteus medius. Weakness of this primary hip abductor could result in greater hip adduction during landing, which in turn can lead to greater frontal plane knee motion. 39 In contrast, weakness of the gluteus maximus has been theorized to contribute to greater knee valgus motion via reduced control of hip internal rotation given the role of the gluteus maximus as an external rotator of the hip. 27,33,39 However, from a functional perspective, the gluteus maximus should be divided into upper and lower portions, with the upper portion primarily serving as a hip abductor. 15,16,39 Therefore, weakness of the gluteus maximus could also directly contribute to reduced control of hip adduction and in turn greater knee valgus motion during athletic movements.
The results of previous research evaluating relationships between hip muscle function and frontal plane hip and knee kinematics have been inconsistent. Multiple researchers have reported a relationship between lesser hip adduction or knee valgus motion and greater hip extension or abduction strength, 7,17,22,28,29,45 but others have not identified this relationship. 21,24,35,38,42 –45 While much of this inconsistency is likely due to differences in movement tasks and participant populations, another potential limitation is that the overwhelming majority of these studies have quantified strength by measuring the peak torque produced during a maximal voluntary isometric contraction (MVIC). However, it takes at least 250 ms after torque onset to attain peak torque during MVIC. 1,2 In contrast, peak hip adduction and knee valgus during landing generally occur less than 150 ms after initial contact. 31,36 Thus, being able to rapidly develop sufficient torque during time-critical periods using the hip musculature (ie, the rate of torque development) may be more influential for controlling frontal plane hip and knee motions during landing than absolute peak torque–producing capacity. Furthermore, while peak torque and the rate of torque development (RTD) are related, 4,6 Holtermann et al 23 reported a 63% increase in explosive strength (as measured by RTD) compared with only a 16% increase in peak strength after training. These results suggest that RTD is not only modifiable but that this measure provides different information about muscle performance than peak torque.
Therefore, the purpose of this study was to determine the influence of explosive hip abductor and extensor strength on frontal plane hip and knee kinematics during a single-leg jump-cut task. We hypothesized that females with greater explosive hip abductor and extensor strength, respectively, would exhibit lesser hip adduction and knee valgus motion compared with females with lesser rates of torque development.
Methods
Participants
Forty healthy, recreationally active female volunteers between 18 and 30 years of age (mean age, 21.0 ± 1.7 years; mean height, 167.4 ± 7.8 cm; mean mass, 65.9 ± 8.5 kg) were recruited from the local college population and surrounding area as participants in this investigation, which was approved by the Institutional Review Board at Oregon State University. Recreationally active was defined as participating in at least 150 minutes of moderate to vigorous physical activity per week. 13 All participants reported (1) no history of lower extremity surgery, (2) no current injury or illness limiting their physical activity level, (3) no leg or low back injury in the past 6 months that limited their physical participation, (4) no previous ACL injury, and (5) participation in an activity involving cutting or jumping within the previous 6 months. They were also asked not to partake in any strenuous exercise 24 hours prior to testing. Participants reported to the Biomechanics Laboratory where they were informed of the study procedures and risks of participation before providing written consent to participate. All participants were outfitted in spandex shorts and tank tops and wore their own athletic shoes during testing. The height and mass of each participant was recorded prior to data collection for biomechanical model generation and standardization of the dependent variables. Leg dominance was determined by which leg participants used to complete at least 2 of the following 3 tasks: (1) kicking a ball for distance, (2) stepping onto a 25-cm box, and (3) recovering from a small perturbation from behind. 20 Participants then completed a 5-minute warm-up at moderate intensity on a stationary bike.
RTD Assessment
RTD was measured using a Biodex System 3 dynamometer (Biodex Medical Systems Inc) interfaced with The MotionMonitor motion analysis software (Innovative Sports Training). Participants performed 3 MVICs of the hip abductors and 3 MVICs of the hip extensors with 1 minute of rest between trials. For each MVIC trial, participants were instructed to contract “as hard and fast as possible” for 3 seconds in response to a light stimulus, with verbal encouragement provided during the duration of each trial. Torque-time curves were immediately evaluated after every MVIC trial for an initial countermovement and a plateau on the curve. The plateau was to ensure peak torque was achieved. Trials exhibiting a countermovement or no plateau were not used and the trial repeated.
For hip abduction, the participant was positioned in a side-lying position on the nondominant side with the hip center of rotation aligned with the dynamometer axis of rotation (Figure 1). The hip was stabilized with a strap over the iliac crest, and the resistance pad of the movement arm was placed just superior to the lateral epicondyle. The participant was strapped with the test leg in 15° of extension and 0° of hip abduction and external rotation. The participant was instructed to push their leg straight up into the resistance pad, and verbal encouragement was provided during the trial.

Participant testing position for assessment of hip abductor rate of torque development.
Hip extension RTD was measured with the participant placed prone with the legs off the end of the Biodex (Figure 2). The greater trochanter was aligned with the dynamometer axis of rotation. The resistance pad of the movement arm was placed just superior to the popliteal fossa with the test leg placed in 30° of hip flexion and 90° of knee flexion. The participant wrapped her arms around the chair and the low back was strapped down. The participant was instructed to kick her thigh straight backward while maintaining 90° of knee flexion.

Participant testing position for assessment of hip extension rate of torque development.
Lower Extremity Biomechanics Assessment
After RTD testing, lower extremity biomechanics were assessed during a single-leg jump-cut task. Participants were outfitted with a retroreflective marker set (27 static, 23 dynamic) placed bilaterally on the acromion process, anterior superior iliac spine, posterior superior iliac spine, greater trochanter, anterior thigh, medial and lateral femoral epicondyles, anterior shank, medial and lateral malleoli, and the sacrum. Also, markers were placed bilaterally on the shoes over the approximate locations of the calcaneus and the first and fifth metatarsal heads. Nine motion capture cameras (Vicon Inc) were used to record participant kinematics during single-leg jump-cuts after a static subject calibration trial. Participants performed the jump-cut task as previously described by Frank et al 9 (Figure 3). Briefly, participants stood a distance of 50% of their body height from the nearest edge of a force plate (Type 4060-08; Bertec Corp) and a 17-cm-high hurdle was placed 25% of their body height in front of the force plate. The participant performed a double-leg jump over the hurdle, landed on the dominant leg with the foot positioned entirely on the force plate, and then cut at a 60° angle in the direction opposite the dominant leg as fast as possible (eg, landing on the right leg required a cut to the left). Participants performed at least 3 practice trials before completing 5 testing trials with at least 30 seconds of rest between trials.

Right leg–dominant participant performing the single-leg jump-cut task.
Data Sampling, Processing, and Reduction
The raw voltage signal from the Biodex System 3 dynamometer was sampled at 1560 Hz using The Motion Monitor software during the isometric contraction trials. The recorded voltage signal for each trial was digitally low-pass filtered at 10 Hz using a fourth-order Butterworth filter, converted to torque (N·m) via a calibration equation function, and corrected for the effects of gravity on the leg using custom written computer software (LabVIEW; National Instruments Corp). Then, this same custom software was also used to calculate RTD during each MVIC trial during the 200 ms after the onset of muscle contraction (ie, time point when torque exceeded 2.5% of peak torque). RTD was calculated as the slope of the line that best fit the torque-time curve over the period of interest (0-200 ms). This specific RTD time interval was chosen as it provides information specific to the explosive force-producing capacity of muscle function 3 but would not be less than the time that is required to reach peak hip adduction and knee valgus angles during landing. 31,36 The maximum RTD value across the 3 trials for each motion was normalized to body mass and used for statistical analysis.
The kinematic and force plate data during the single-leg jump-cut task were sampled at 120 and 1560 Hz, respectively, using the Vicon Motion Analysis software. Raw 3-dimensional kinematic coordinates and force plate data were imported into the Motion Monitor motion analysis software for biomechanical model generation (Innovative Sports Training). Ankle and knee joint centers were defined as the midpoint of the medial and lateral malleolus and the medial and lateral femoral epicondyle markers, respectively. The hip joint center was predicted using external landmarks as described by Bell et al. 5 The local coordinate systems of the shank, thigh, and sacrum were defined with the positive x-axis directed anteriorly, positive y-axis directed to the left, and the positive z-axis directed superiorly. Kinematic data were low-pass filtered at 10 Hz using a fourth-order zero-phase lag Butterworth digital filter, time-synchronized to force plate data and resampled at 1560 Hz. Joint angular positions were calculated based on a right hand convention using Euler angles in a Y (flexion/extension), X′ (adduction/abduction), Z″ (internal/external rotation) rotation sequence with motion defined about the knee as the shank relative to the thigh and about the hip as the thigh relative to the pelvis. Custom computer software (LabVIEW) was used to identify dominant limb initial contact and peak hip adduction and knee valgus angles as well as angular displacements for each trial between initial contact (vertical ground reaction force >10 N) and the time of peak knee flexion. All dependent variables were averaged across the 5 trials prior to statistical analysis.
Statistical Analysis
After data reduction, subjects were divided into tertiles for the hip abduction and hip extension RTD measures independently. All data were then checked for consistency and tested for violations of the assumption of normality. To test the hypotheses that females with greater RTD would exhibit lesser hip adduction and knee valgus, separate 1-tailed, independent-samples t tests or Mann-Whitney U tests were used as appropriate to identify significant differences in the dependent variables between the highest (high) and lowest (low) tertiles for each RTD measure. A 1-tail test was chosen in the design of this study due to the fact that the only potentially relevant clinical implication was if females with greater RTD exhibited lesser frontal plane hip and knee motion. The alternative finding, that females with lesser RTD exhibited lesser frontal plane hip and knee motion, would have no more clinical relevance than if there were no significant differences between groups. In either of these instances, we would not have suggested that RTD be decreased to improve frontal plane kinematics. Though uncommon, this approach has been used in previous research evaluating group differences in strength and landing mechanics. 24 All statistical procedures were performed using SPSS Statistics 23.0 (IBM Corp).
Results
Post hoc analysis indicated moderate-high within-session reliability for hip abduction (ICC 2,1 = 0.76, SEM = 80.0 (N·m/s)/kg) and hip extension (ICC 2,1 = 0.83, SEM = 86.5 (N·m/s)/kg) RTD. The allocation of participants into tertiles was successful in creating high and low hip abduction (high, 10.0 ± 1.9; low, 5.1 ± 1.2 (N·m/s)/kg; P < .001) and hip extension (high, 11.1 ± 1.9; low, 4.9 ± 1.4 (N·m/s)/kg; P < .001) groups with significantly different RTDs (Figures 4 and 5).
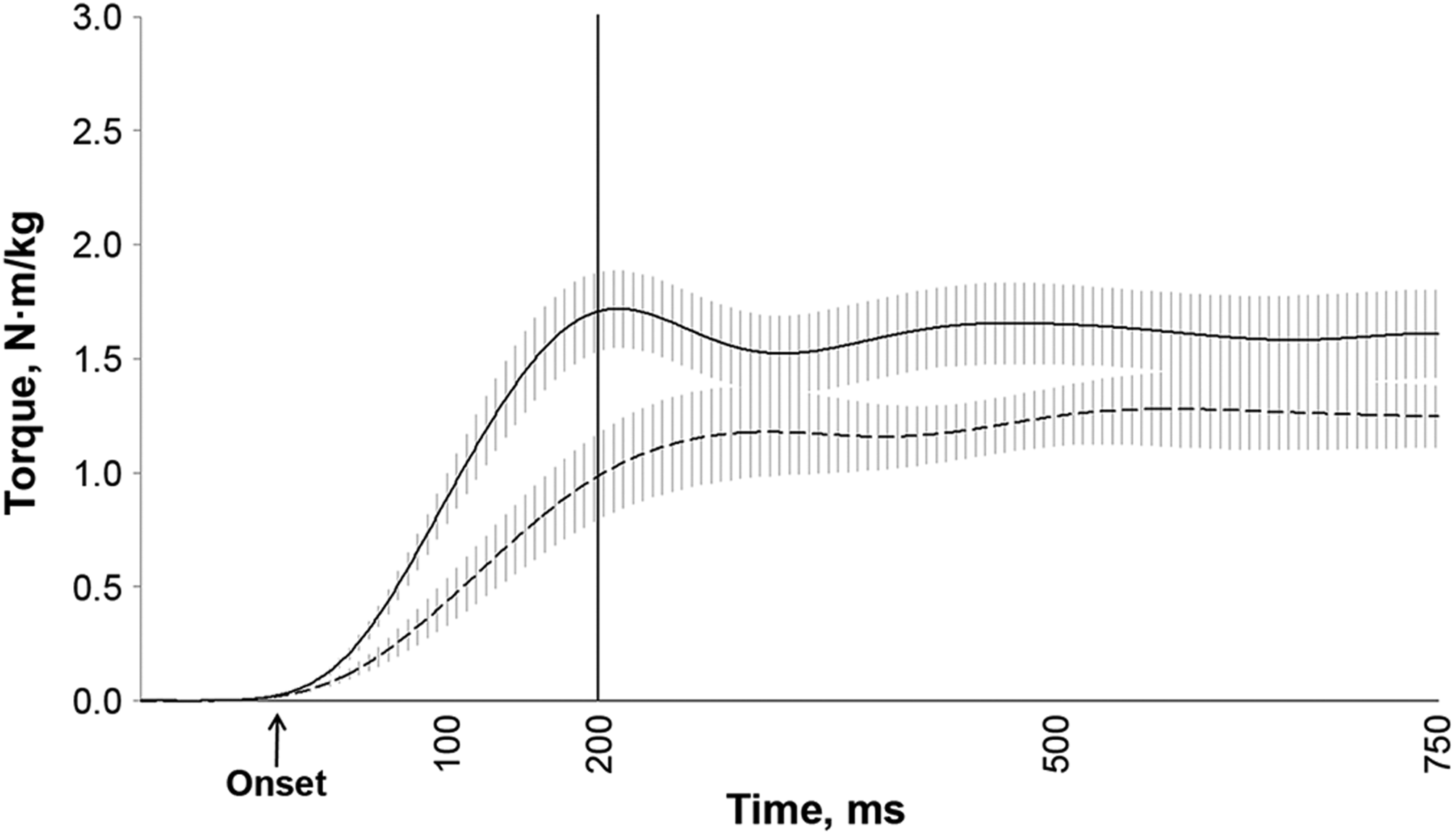
Ensemble torque-time curves with 95% confidence intervals for the high (solid line) and low (dashed line) hip abduction rate of torque development groups.
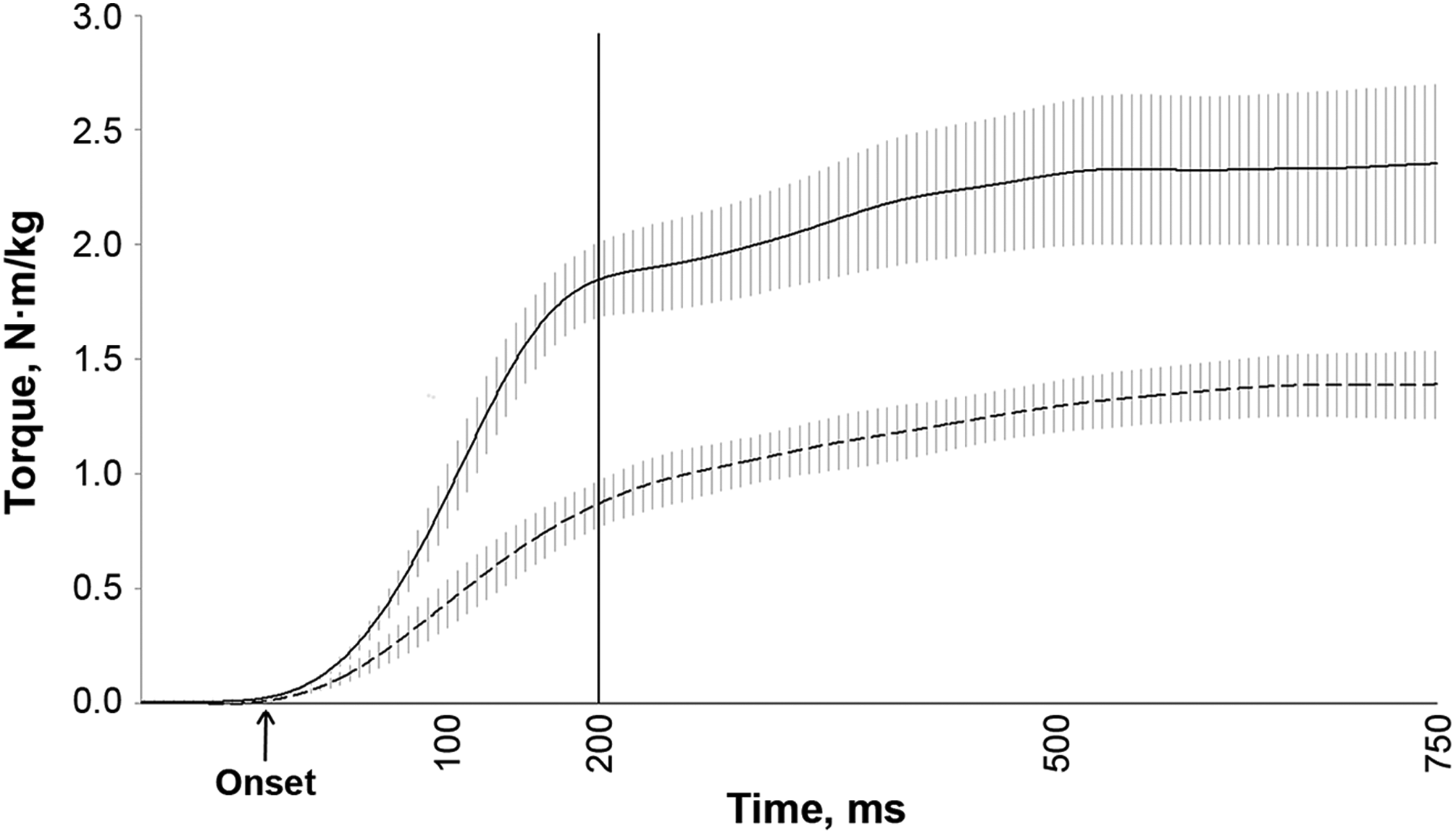
Ensemble torque-time curves with 95% confidence intervals for the high (solid line) and low (dashed line) hip extension rate of torque development groups.
No significant differences in frontal plane hip or knee kinematics were identified between high and low hip abduction RTD groups (Table 1). For hip extension RTD, the low group exhibited significantly greater hip adduction and knee valgus angular displacements than the high group (Table 2). Furthermore, while both groups maintained a relatively abducted hip position during the jump-cut task, the peak frontal plane hip angle of the low hip extension RTD group was approximately 5° closer to neutral than the high hip extension RTD group. No other significant group differences in frontal plane hip and knee kinematics were identified.
Comparison of Frontal Plane Hip and Knee Kinematics Between High and Low Hip Abduction RTD Groups a
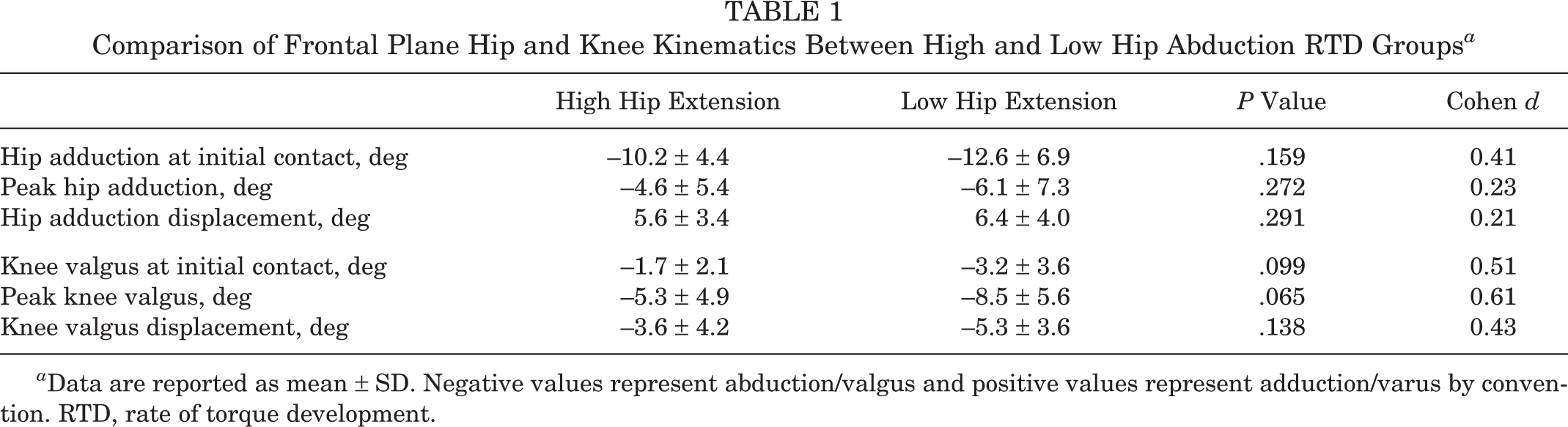
a Data are reported as mean ± SD. Negative values represent abduction/valgus and positive values represent adduction/varus by convention. RTD, rate of torque development.
Comparison of Frontal Plane Hip and Knee Kinematics Between High and Low Hip Extension RTD Groups a
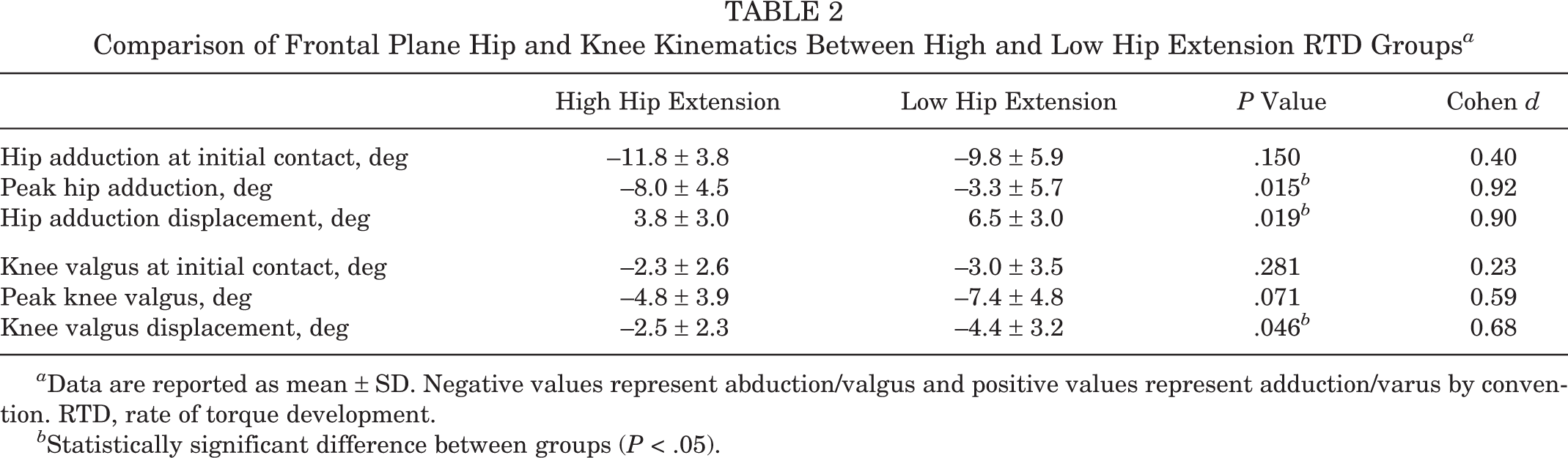
a Data are reported as mean ± SD. Negative values represent abduction/valgus and positive values represent adduction/varus by convention. RTD, rate of torque development.
b Statistically significant difference between groups (P < .05).
Discussion
The purpose of this investigation was to determine the influence of explosive hip abductor and hip extensor strength on frontal plane hip and knee kinematics during a single-leg jump-cut task. Our primary finding was that while hip abductor RTD was not related to frontal plane hip or knee kinematics, females with greater explosive hip extension strength exhibited lesser hip adduction and knee valgus motion when performing a single-leg jump-cut.
Contrary to our hypothesis, the capacity to explosively generate hip abduction torque did not influence frontal plane hip or knee kinematics (initial contact, peak, or displacement) during the movement task. While previous reports on the relationship between hip abduction strength and frontal plane kinematics are equivocal, ∥ we theorized that the lack of an association in some of these studies was due to the use of relatively low-level tasks such as double-leg landings and forward lunges 24,43 because investigations using more demanding tasks such as treadmill running and single-jump landings did associate greater hip abduction strength with lesser hip adduction or knee valgus motion. 17,29 However, in the present study, we did not identify significant differences in frontal plane kinematics between healthy females with greater and lesser RTD when completing a relatively demanding single-leg jump-cut task. One potential reason for the lack of group differences is that, consistent with previous studies that have investigated cutting movements, 25,41 participants were in a relatively abducted hip position as they landed and changed direction. Females in this investigation generally landed with 10° to 13° of hip abduction and remained abducted during the entire loading phase. As a result, the gluteus medius, which acts as the primary hip abductor, was in a suboptimal position to control hip adduction. 33 Specifically, despite being the primary producer of hip abduction torque, the gluteus medius’ ability to produce force decreases in a nearly linear fashion as the hip moves from 10° of adduction and into an abducted position. 8,33,34,37 In addition to performing single-leg jump-cuts in an abducted position, secondary analysis of our data indicated that, on average, participants were in about 30° of hip flexion at initial contact and throughout the loading phase of the single-leg jump-cut. Increased hip flexion also serves to decrease the hip abduction torque–producing capacity of the gluteus medius. As the hip flexes from 0° to 40°, the moment arm vector component of the gluteus medius for hip abduction decreases, resulting in a reduction in torque production. 8 Therefore, the combined use of an abducted and flexed hip likely served to significantly reduce the capacity of the gluteus medius to control hip adduction, and in turn knee valgus, motion during this task and may explain why participants with greater hip abduction RTD did not exhibit differences in frontal plane hip and knee displacements compared with those with less explosive hip abductors. These results indicate that explosive hip abductor strength may not be as influential for controlling hip adduction and knee valgus motion during all types of movement tasks as has been previously proposed.
In contrast, we identified that greater hip extension RTD was related to lesser peak hip adduction and adduction displacement suggesting that explosive strength of the gluteus maximus might be important for controlling frontal plane hip motion during movement tasks such as a single-leg jump-cut that are performed with the hip in a relatively abducted and flexed position. While the gluteus maximus is primarily viewed as a hip extensor and external rotator, 33 there is evidence that the upper portion of the gluteus maximus functions as a hip abductor, with this action becoming more pronounced as the hip becomes more flexed. 12,15,16,32,40 Shen 40 and Gao 12 reported that in children with gluteus maximus contracture, the frontal plane position of the hips is neutral while standing. However, when patients flexed the hips past 30°, the thighs assumed an abducted position suggesting that at least some portion of the gluteus maximus has an abduction line of action. Lyons et al 32 reported that the activation amplitude and timing of the upper portion of the gluteus maximus mirrored the gluteus medius during free walking and stair ascent and suggested that the upper gluteus maximus acts as a hip abductor during the loading response and single-leg support. Moreover, Grimaldi et al 16 demonstrated that the upper and lower portions of the gluteus maximus respond differently to hip joint pathology and concluded that the gluteus maximus should be considered to have 2 functional groupings with the upper gluteus maximus part of a hip abductor synergy that also includes the tensor fascia latae. 15,16 Therefore, it is possible that during the single-leg jump-cut, the gluteus maximus, by virtue of its upper fibers, was able to take on an important role in controlling frontal plane hip motion in place of the gluteus medius, whose function was compromised by the abducted and flexed hip position used by participants. This notion is supported by our data, which demonstrate that those categorized as having more explosive gluteus maximus strength (ie, high hip extensor RTD group) exhibited significantly lesser hip adduction displacement than those categorized with lesser explosive gluteus maximus strength.
In addition to the significant differences in frontal plane hip kinematics between the hip extension RTD groups, we also identified lesser knee valgus displacement in participants classified as having greater explosive hip extensor strength, which is consistent with previous research evaluating hip extensor strength and activation and frontal plane knee kinematics. 21,22 Hollman et al 21 reported that increased gluteus maximus activation was associated with a decrease in peak knee valgus angles during a single-leg step down and that greater hip extensor strength and activation were predictive of lesser peak knee valgus angles during a jump-landing task. 22 Though the difference in knee valgus displacement identified in the current investigation was statistically significant, the mean difference between groups was only 1.9°. While the magnitude of this difference elicited in a laboratory setting is not immense, it is possible that in more demanding landing and cutting tasks such as those encountered in sporting activities, individuals with less explosive hip extensors might experience greater hip adduction and knee valgus motion, thereby potentially increasing their risk for acute and overuse lower extremity injuries.
The primary limitation of this investigation is that the sagittal plane position of the hip during the hip abduction RTD assessment was 15° of extension, which differed from the 30° of hip flexion exhibited by participants at initial contact and throughout the jump-cut task. In contrast, hip extension RTD was assessed with the hip positioned in a similar sagittal plane position to that subsequently utilized by participants during the jump-cut (approximately 30°). While it is possible that these testing positions influenced our results, we chose to measure hip abduction RTD in slight hip extension to mimic clinical practice and in an attempt to isolate the gluteus medius from the other hip abductors. 19,30 In addition, as muscle activation of the upper and lower portions of the gluteus maximus were not measured, it is not possible to determine whether greater utilization of the upper portion of the gluteus maximus was in fact the primary contributor to lesser hip adduction and knee valgus motion. Therefore, it is important that future studies directly examine neuromuscular activation of the gluteus maximus.
Conclusion
Despite being somewhat unexpected, this investigation presents novel findings that may be immediately relevant to researchers and clinicians alike. The results highlight the potential importance of explosive gluteus maximus strength in controlling frontal plane motion at the hip and knee during certain types of activities and suggest that including specific training to increase explosive hip extensor strength may be crucial in the primary prevention and rehabilitation of a variety of lower extremity injuries. While the gluteus medius has long been believed to be the primary muscle to be targeted in rehabilitation and prevention programs in terms of reducing frontal plane hip and knee motion, the present results do not support that paradigm to uniformly exist during all types of movement tasks. Our findings indicate that in tasks such as jump-cuts that are performed with the hip in an abducted and flexed position, the gluteus maximus may play a pivotal role in controlling frontal plane hip and knee motion. As a result, we propose including training with a particular emphasis on increasing explosive strength of the gluteus maximus, through the use of contractions with an intention to move quickly, during injury prevention and rehabilitation programs may be important for improving frontal plane hip and knee kinematics and reducing injury risk. However, future interventional and prospective studies are necessary to confirm this hypothesis.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Notes
Acknowledgment
The authors thank Anne Pollard, Roy Almog, Christopher Asplund, and Michelle Correia for their assistance with data collection.