
Abstract
BACKGROUND:
The abdominal draw-in maneuver (ADIM) has been suggested to increase trunk stabilizing muscle activity; however, no study has identified the effects of the ADIM on trunk muscles and trunk movements during lifting and lowering (L & L) tasks.
OBJECTIVE:
We examined the effects of the ADIM on transversus abdominis (TrA) thickness during standing, the activity of the TrA, internal oblique (IO) and multifidus (MF), and the kinematics of the lumbo-pelvic-hip complex during L & L tasks.
METHODS:
Fifteen male participants practiced expirations without and with the ADIM using ultrasound biofeedback. After training for each condition, the participants performed expirations with and without the ADIM in the standing position and during L & L tasks. TrA thickness during the standing position and muscular activities (EMG) of the bilateral TrA/IO and MF, and the peak angle of the lumbo-pelvic-hip complex in the sagittal plane during L & L tasks were measured.
RESULTS:
TrA thickness during standing was increased with expiration with ADIM compared to that without the ADIM (
CONCLUSIONS:
The ADIM could be an effective strategy to improve trunk stability and reduce lumbar flexion during L & L tasks.
Introduction
Manual material handling tasks, including L & L tasks, are frequently performed during the course of daily activities and in the workplace. Unfortunately, such tasks pose a risk for low back pain (LBP) [1, 2]. It has been reported that trunk instability and repeated excessive lumbar flexion increase mechanical stress on the lower back, leading to LBP [1, 2, 3]. Although the squatting posture has been recommended to decrease repeated excessive lumbar flexion and mechanical stress on the lower back, stooping while lifting is often preferred due to lower perceived exertion, delayed onset of fatigue, better balance control, and greater convenience, among others [4]. Therefore, injury prevention strategies targeting improved trunk stability and decreased lumbar flexion should be considered to minimize mechanical stress on the lower back during L & L tasks performed in a stooped posture.
For active trunk stabilization, the roles of the tran-sversus abdominis (TrA), internal oblique (IO), and multifidus (MF) muscles have been emphasized [3, 5, 6]. Because these muscles attach to the lumbar spine directly or indirectly via the thoracolumbar fascia, their activation increases stiffness of the spine, thereby improving lumbar stability [3, 6]. To facilitate TrA activation, the abdominal draw-in maneuver (ADIM), which is the most common component of lumbar stabilization exercise programs, has been especially recommended [3, 7]. In a previous study, ADIM facilitated TrA activation more effectively relative to that of other superficial muscles [8]. Furthermore, the ADIM increases IO muscle activity [7, 9], leading to co-contraction of the MF muscles [10] and consequently enhanced trunk stability.
Although previous studies demonstrated that the ADIM leads to effective TrA activation [11, 12], precise training in the maneuver is difficult in clinical settings because of the impracticality associated with fine wire electromyography (EMG), as well as the difficulty of targeted palpation of the TrA [8, 12]. Thus, clinicians use ultrasound biofeedback to detect TrA activation during ADIM [7, 12]. Ultrasound biofeedback guidance allows more effective and precise ADIM training [7, 12]. Furthermore, greater TrA activation occurs with ultrasound biofeedback, compared with the tactile or verbal feedback that can be provided by a clinician [7].
A recent study demonstrated that short-term ADIM training with ultrasound biofeedback increased TrA thickness during a functional reaching task [12]. Moreover, other studies showed that ADIM increases spinal stiffness [13] and decreases unnecessary lumbo-pelvic movement during lower extremity movements [14]. Taken together, these findings indicate that the ADIM facilitates activity of the trunk stabilizer muscles, thereby increasing trunk stiffness and decreasing unnecessary lumbopelvic movements. Considering that decreased lumbar flexion increases hip flexion during activities involving forward-bending and return from forward-bending tasks [15], the improved trunk stability and altered lumbo-pelvic movements induced by the ADIM may influence hip movement during L & L tasks. Also, according to a biomechanical model, lifting tasks in a stooped posture require the activation of transversely oriented muscles such as the TrA and IO muscles for lumbo-pelvic stability [16]. In line with this biomechanical model, previous studies have demonstrated that weight-bearing tasks facilitate greater TrA and IO muscle activation during ADIMs in healthy individuals [17, 18]. Thus, it is possible that the ADIM leads to greater trunk stabilizer muscle activation to achieve lumbo-pelvic stability during L & L tasks under weight-bearing conditions. However, it is unclear as to whether the ADIM changes trunk stabilizer muscle activity and the kinematics of the lumbo-pelvic-hip complex during L & L tasks. Therefore, the aim of the present study was to examine the effects of the ADIM on TrA thickness during standing, EMG activity of the trunk stabilizer muscles, and kinematics of the lumbo-pelvic-hip complex during the performance of L & L tasks.
Methods
Participants
Fifteen healthy males (mean age
The sample size was calculated based on a large effect size (
Ultrasound imaging
Ultrasonography (MyLabOne; Esaote SpA, Via Siffredi, Italy) with a 7.5-MHz linear probe was used to measure TrA thickness and perform ultrasound biofeedback. The probe, placed at the mid-point between the last rib and the iliac crest on the right side, was manipulated to find the optimal fascial plane [8, 11]. The probe position was marked with tape. Small movement (
Transversus abdominis (TrA) thickness measured by ultrasonography. Abbreviation: TrA, transversus abdominis.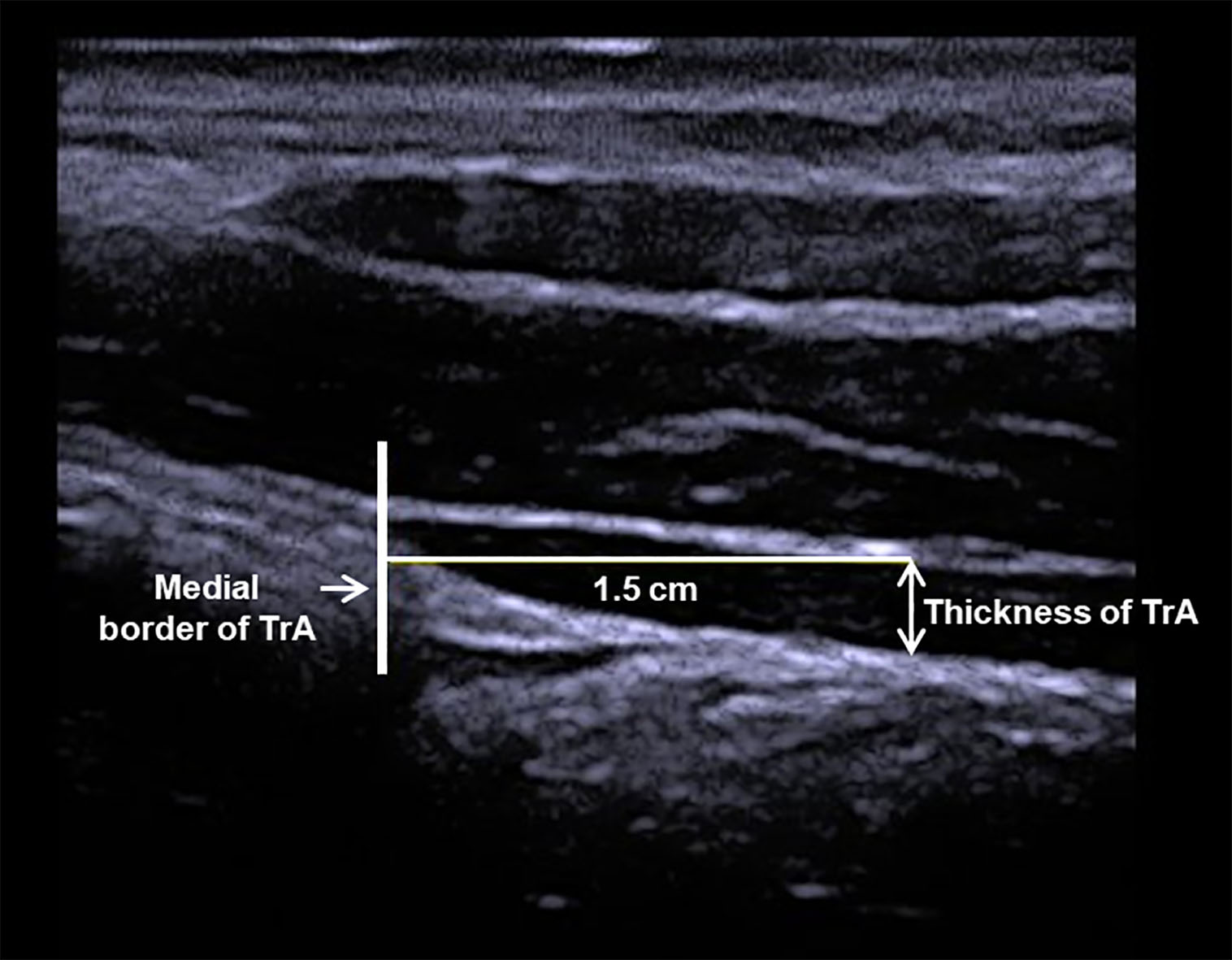
EMG activities of the bilateral transversus abdominis/internal oblique (TrA/IO) and multifidus (MF) muscles during performance of the L & L tasks were measured using a Delsys Trigno Wireless EMG system (Delsys, Boston, MA, USA). Because we used a surface EMG, combined activity of the TrA and IO muscles (TrA/IO) was measured. Previous studies showed that surface EMG activities of the TrA/IO and MF muscles correlate significantly with TrA and MF muscle activities, respectively, as measured using fine wire EMG [21, 22]. In the present study, the sampling rate of the EMG signal was 1,000 Hz, with a bandwidth of 20–450 Hz. All EMG data were full-wave rectified and converted to root-mean-square (RMS) values. To record bilateral TrA/IO activity, EMG sensors were placed at a location approximately 2 cm medial and inferior to the bilateral anterior superior iliac spines, at which the TrA and IO muscles are fused with no overlapping of the external oblique (EO) muscle [23]. The EMG sensors were attached at a location 2 cm lateral from the L5 spinous process to record bilateral MF activity [21].
All EMG data were normalized to the maximum voluntary isometric contraction (MVIC) of each muscle according to maneuvers suggested by previous studies [24, 25]. Each MVIC maneuver was performed twice for 5 s with a rest time of 1 min between maneuvers. The average value of the middle 3 s of two MVIC trials was calculated for normalization of TrA/IO and MF values.
Kinematic data recording
The VICON MX-T10 motion capture system (Vicon Motion Systems Ltd., Oxford, UK), which has eight cameras operating at a sampling rate of 100 Hz, was used to measure kinematic data during performance of the L & L tasks. In accordance with the Vicon Plug-in-Gait model, reflective markers were attached bilaterally to the anterior superior iliac spines, posterior superior iliac spines, lateral thighs, and lateral knees (for pelvic and thigh segments). Four additional reflective markers were attached to the L1 and L2 spinous processes, and to both sides of the L2 spinous process, for the lumbar segment [15]. A single reflective marker, attached to the front of a 4.5 kg box, was positioned 30 cm in front of the participant to record vertical motion of the box. Nexus software (ver. 1.7; Vicon Motion Systems Ltd.) was used to calculate the angle of the lumbo-pelvic-hip segments and displacement of a single reflective marker, attached to the front of the box, in the sagittal plane. The lifting task was defined as the time between moving the box from its lowest to its highest point, while the lowering task was defined as the time between moving the box from its highest back to the lowest point (Fig. 2). The highest point of the box was defined as the point at which the marker, attached to the box, was highest in the sagittal plane according to the Nexus software.
L & L tasks.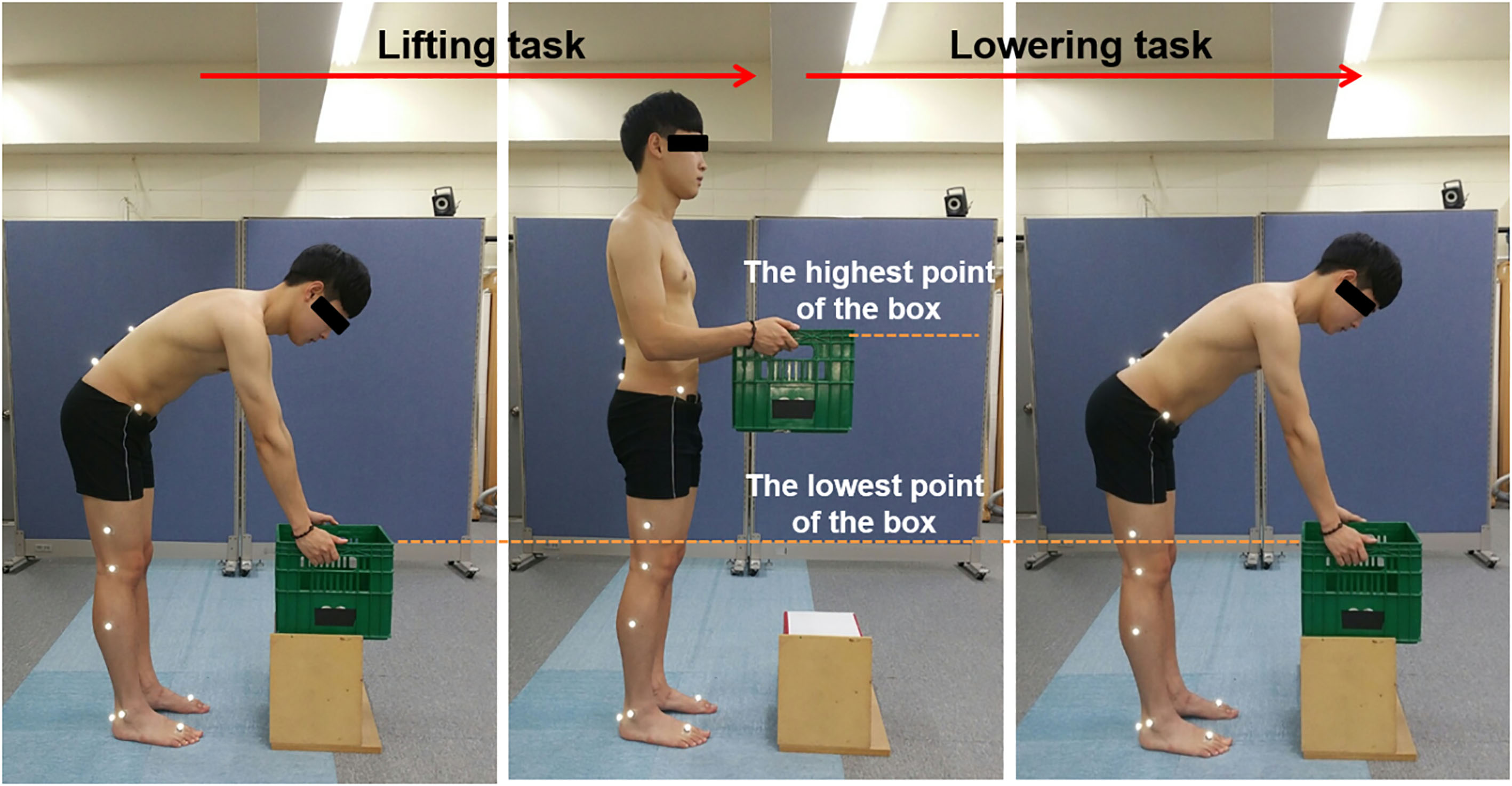
The angles of the lumbar spine and hip were calculated according to the motion of the lumbar and hip segments, respectively, relative to the pelvic segment according to Cardan angles [24, 27]. The pelvic angle was defined as the motion of the pelvic segment with respect to a laboratory-based reference coordinate system [15]. Positive values denoted lumbar flexion, hip flexion, and pelvic anterior tilt.
An investigator instructed participants on correct expiration performance while in the standing position, with and without ADIM. To control respiration, participants were instructed to exhale and hold their breath, in both the ADIM and the non-ADIM conditions [11, 12]. Participants were also asked to use the following two strategies: (1) for expiration without ADIM: “Take a deep breath. Afterward, exhale and hold the exhalation for 10 s”; and (2) for expiration with ADIM: “Take a deep breath. Afterwards, draw your belly button up and into your spine while exhaling. Hold your breath for 10 s [11]”. All participants practiced for 20 min, or until they had performed three successive, normal breaths [28] in the without-ADIM condition. Afterwards, all participants practiced expiration in the with ADIM condition. Ultrasound biofeedback was provided so that participants could recognize TrA activation during the ADIM. All participants again practiced for 20 min, or until they had performed three successive, correct maneuvers [7, 20].
Participants were asked to perform the L & L tasks under the two expiration conditions with and without the ADIM as described above. The box height was adjusted using wooden plates so that its handle was at knee joint level. The participants stood with feet shoulder-width apart and grasped the box while flexing the lumbar spine and maintaining extension of the elbow and knee. Each participant was instructed to lift the box until the trunk was upright with 90
Data analysis
The average TrA thickness (mm) for three trials in the standing position, for both ADIM conditions during expiration (with and without the ADIM), was calculated to evaluate the effects of the ADIM on TrA thickness. In the normalized EMG data (%MVIC), the peak TrA/IO and MF values and kinematic data (
The normality of distribution of the data was assessed using the Shapiro-Wilk test. The difference in TrA thickness between the two ADIM conditions during expiration (with or without the ADIM) was assessed using a one-way repeated-measures analysis of variance (ANOVA). The EMG and kinematic data during the L & L tasks were assessed using a two-way repeated-measures ANOVA, with the ADIM condition during expiration (with or without the ADIM) and task (lifting or lowering) as the within-subject factors. Post hoc analysis using the Bonferroni correction was performed when significant interactions or main effects were observed. Partial eta squared (
Results
TrA thickness was significantly greater in the expiration with versus without ADIM condition (5.38
Although no significant ADIM condition during expiration-by-task interactions were seen for any of the kinematic data (all
Descriptive data on muscle activities and kinematics during performance of L & L tasks
Descriptive data on muscle activities and kinematics during performance of L & L tasks
The findings of the present study demonstrate that ADIM facilitates TrA/IO and MF muscle activities, as well as pelvic and hip movements, while also minimizing lumbar flexion during the performance of L & L tasks.
Our result is in agreement with previous studies, where ADIM training with ultrasound biofeedback led to an increase in TrA thickness [7, 12]. The ADIM is a training maneuver that leads to selective TrA activation by drawing in the lower abdomen [7, 8, 11]. Previous studies showed that the ADIM using verbal cues increased the TrA thickness in the supine and standing positions [8, 11]. However, objective TrA activation during the ADIM could not be identified when only providing a verbal cue. On the other hand, ultrasound biofeedback can reveal real-time changes in TrA thickness, which may result in more effective performance of the ADIM. A previous study demonstrated that ADIM training with ultrasound biofeedback led to greater TrA thicknesses compared with ADIM training with tactile and verbal feedback [7]. Thus, we infer that the combined training effects of both the ADIM and the application of ultrasound biofeedback resulted in an increased TrA thickness during expiration with versus without the ADIM.
We performed training for TrA activation using the ADIM with ultrasound biofeedback and measured the change in TrA thickness in the same standing position. Van Vliet and Heneghan [30] suggested that it is essential to perform functionally orientated exercises to improve motor control for trunk stability enhancement. Because L & L tasks are performed in the standing position, we considered that the standing position is more appropriate than the supine position for ADIM training. Although real-time feedback of TrA thickness could facilitate TrA activation when performing the ADIM with ultrasound biofeedback, it could not ensure that subjects can facilitate correct TrA activation using the ADIM method with biofeedback removed. Thus, it needs to be confirmed whether TrA activation is increased during the ADIM without biofeedback after training with ultrasound biofeedback. Considering that the change in TrA thickness differs according to the position in which the ADIM is performed [8], TrA activation needs to be measured in the same position as the training or task position. Thus, we performed training for and the assessment of TrA activation in the same standing position, although ultrasound biofeedback was not applied when assessing changes in TrA thickness during the ADIM.
Greater TrA/IO muscle activity during expiration with versus without the ADIM was observed during both the L & L tasks (
Our findings reveal that ADIM leads to greater co-contraction not only of the IO muscles, but also of the MF muscles during L & L tasks. Because the MF muscles are a crucial lumbar segmental stabilizer, their contraction has frequently been targeted in rehabilitation programs, to reduce pain and functional disability [5]. Matthijs et al. [10] demonstrated that ADIM results in co-contraction of the MF muscles while in a standing position. Considering the strong correlation between surface and fine wire EMG recordings with respect to MF muscle activities [21], it can be inferred that co-contraction of the MF muscles during ADIM contributes to increased surface MF muscle activity during the performance of L & L tasks. In addition, our study demonstrated greater MF muscle activity during the lifting versus lowering task (
The lumbar flexion angle was significantly decreased using the ADIM in both the L & L tasks performed in the present study (
Increases in pelvic anterior tilt and hip flexion angle, together with decreased lumbar flexion, were observed with ADIM during performance of the L & L tasks (
Some limitations of the present study should be noted. First, we trained the subjects for TrA activation using the ADIM with ultrasound biofeedback and measured the TrA thickness under the same standing position condition. We found significant differences in TrA thickness between the expiration with versus without ADIM conditions in the standing position; however, changes in TrA thickness between the expiration with versus without ADIM conditions were not measured during the L & L tasks. Although we infer that TrA thickness may be increased under the ADIM condition during L & L tasks based on the increase in EMG activity of the TrA/IO and MF muscles, future studies should use a direct approach to measure changes in TrA thickness during L & L tasks with the ADIM. Second, only healthy subjects participated in our study: future studies should assess differences in outcome between healthy subjects and LBP patients. Also, the sample size of the present study was relatively small. Future studies should include more subjects, including healthy subjects and/or LBP patients. Lastly, although we found a significant increase in TrA thickness under the ADIM condition during standing, the difference in TrA thickness between the with and without ADIM conditions was about 2 mm. Therefore, it is difficult to assert whether this difference is clinically significant.
Conclusions
In conclusion, increased TrA thickness when standing was seen during expiration with versus without ADIM. Additionally, increases in the EMG activities of the TrA/IO and MF muscles, as well as in the peak angle of pelvic anterior tilt and hip flexion, were observed together with a decrease in peak lumbar flexion during the performance of L & L tasks with versus without the ADIM. These findings suggest that the ADIM can be an effective strategy for improving trunk stability and decreasing lumbar flexion during L & L tasks.
Footnotes
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. 2015R1D1A1A01056853).
Conflict of interest
None declared.