
Abstract
BACKGROUND:
While interval training is considered an effective modality for improving performance, its effectiveness among athletes may be influenced by previous training experience.
OBJECTIVE:
To investigate whether differences in training background are reflected in the development of exercise capacity and level of muscle damage following a single bout of repeated maximal sprints after an 8-week intervention of high-intensity interval training (HIIT), sprint interval training (SIT), and endurance training (ET).
METHODS:
Three groups of male cyclists were studied: E1 (
RESULTS:
After intervention, VO
CONCLUSIONS:
A history of high-volume moderate-intensity training can induce beneficial performance adaptations by reducing muscle damage and allowing greater work output. It is suggested that interval training be preceded by a longer period of high-volume training in athletes.
Introduction
Sprint interval training (SIT) and high-intensity interval training (HIIT) are known as two potent exercise strategies in the development of aerobic and anaerobic capacity [1, 2, 3]. The former involves several bouts of short maximal intensity exercise (Cca. 30 s) separated by recovery intervals of 15 s–4 min duration [4, 5, 6]. In the latter, the repeated exercise is either performed for several minutes at an intensity exceeding 90% maximal oxygen uptake (VO
In addition to limited information on the combination of different interval modalities, there is lack of documented evidence on the effects of athlete training background. The most majority of interval training studies have stratified their population samples according to VO
Despite many beneficial changes induced by interval training, several negative effects have been identified with muscle damage as the most prominent [18]. It is worth noting that significant exercise-induced muscle fiber damage can result from not only interval training but steady-state exercise performed at moderate or high intensity [19]. Research also suggests that muscle fiber damage is a necessary precursor for the onset of important physiological adaptations [20]. In the literature, some biochemical markers of muscle damage are increased myoglobin concentration (Mb) and creatine kinase activity (CK) in blood plasma following exercise [21, 22]. Interestingly, current findings suggest that eccentric muscular contractions induce greater increases in Mb and CK than concentric contractions [23] and that Mb and CK can also be triggered by increased oxidative stress [21]. However, it is unclear what changes occur to Mb and CK during SIT-based exercise particularly among trained athletes with varied training backgrounds (different macrocycle volume and intensity). This is of interest as many coaches continue to apply the Matveyev model of training periodization [24], in which training progresses from a low-intensity high-volume phase to a high-intensity low-volume phase. This model theoretically would best prepare the athlete for the high loads entailed in interval training. However, there is a modicum of scientific evidence for this model particularly among advanced athletes [24]. An assessment of the acute changes in serum Mb and CK in response to SIT should show the degree of experienced muscle damage among athletes with different training backgrounds. Furthermore, interval training has been strongly promoted as a time-efficient exercise strategy that induces enhanced adaptations compared with longer-duration and more monotonous endurance training [3]. However, little attention has been paid to whether the participant or athlete can tolerate the high loads of SIT, again suggesting the need for research on the effects of this training modality on muscle damage.
Anthropometric and physiological characteristics of groups E1, E2, and C
Anthropometric and physiological characteristics of groups E1, E2, and C
VO
Scheme of the experiment (SIT – sprint interval training; HIIT – high-intensity interval training; CET – continuous endurance training; VET – varied-intensity endurance training; ITP – incremental testing protocol; SITP – sprint interval testing protocol).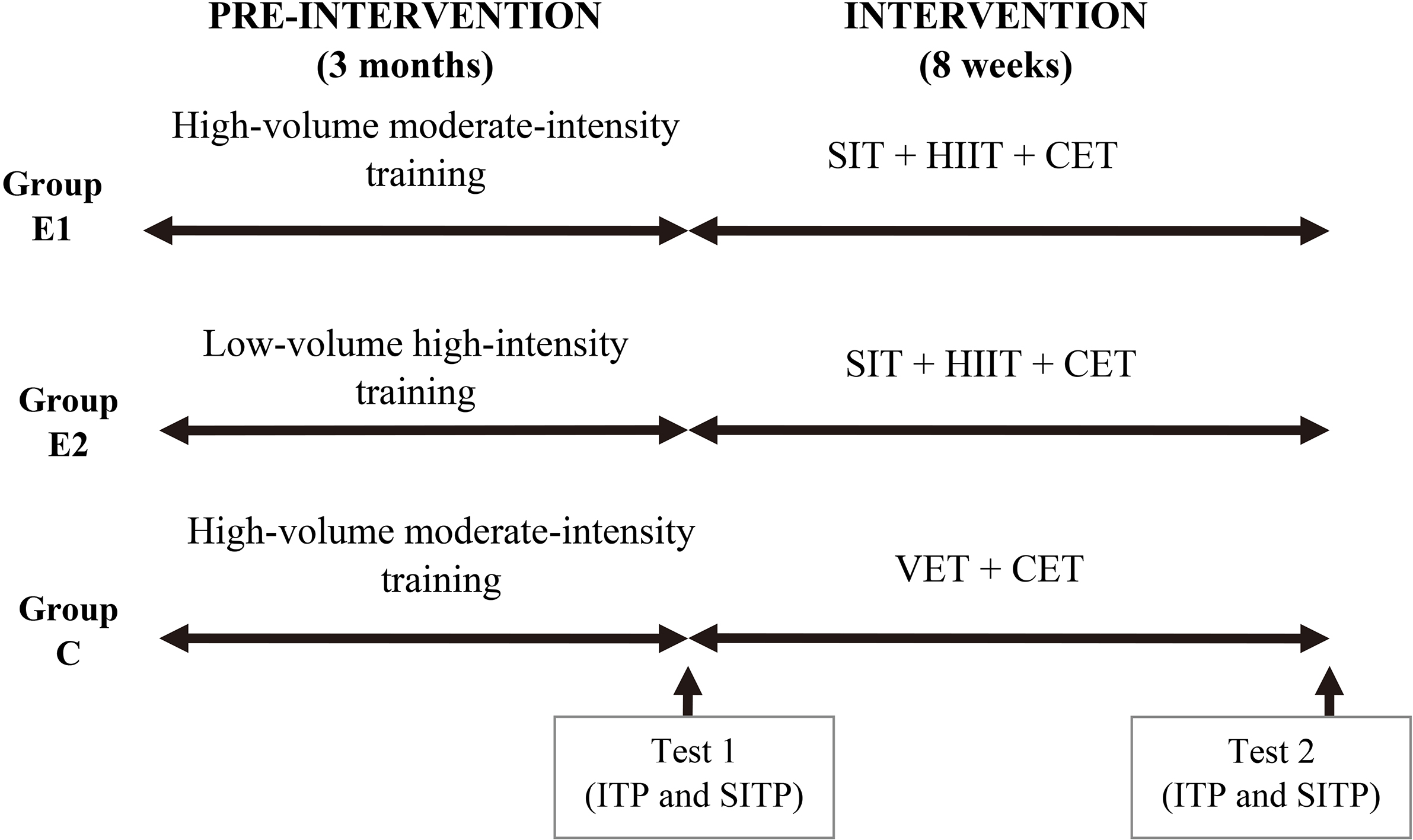
In light of the above, the aim of the study was to determine the effects of a concomitant SIT, HIIT, and continuous endurance training (CET) intervention on maximal aerobic power and VO
Participants
This study design was approved by the institutional ethics committee and all procedures were performed in accordance with the Declaration of Helsinki. Twenty-four male mountain bike (MTB) cyclists were recruited with a minimum of 2 years competitive experience in their respective racing format. Written informed consent was obtained after the procedures were fully explained. Previous training characteristics (heart rate and power output) over a 3-month period prior to study outset were collected from previously saved training records using the Garmin Connect system (Garmin Ltd.,USA). Participant exercise history was then determined and the cyclists were assigned to either one of two experimental groups (E1:
Procedures
The duration of the training intervention was 8 weeks (shown in Fig. 1). HIIT, SIT, and CET were concomitantly executed by E1 and E2. SIT was performed twice a week. Each SIT session involved 12 to 16 repetitions of 30-s maximal intensity cycling with four repetitions constituting one set. Each repetition was interspersed with 90 s of low-intensity cycling not exceeding 30 W. A recovery period was provided between each set in which the first 2 min were performed at an intensity corresponding to 30% maximal aerobic power (determined during an incremental test) followed by 20 min of cycling at 50% maximal aerobic power and then 3 min of cycling at 15% maximal aerobic power. HIIT was performed once a week and involved 5 to 7 cycling bouts of 5 min performed at an intensity 85–95% maximal aerobic power with recovery intervals between each repetition performed at 45–50% maximal aerobic power for 10–15 min. The CET modality was performed twice a week and involved 120–180 min of cycling at an intensity of 70–80% HRmax.
Participants in group C continued their existing training regime based on two endurance training modalities. The first was varied-intensity endurance training (VET) with two sessions held each week. Each session began with several minutes of cycling at an intensity of 65–70% HRmax, followed by cycling again for several minutes at an intensity of 80–85% HRmax, and then several dozen minutes of cycling at 70–80% HRmax. This order was then repeated several times with total session duration 120–180 min. The second involved steady-state CET executed three times a week. In this modality, the controls cycled for 120–180 min at an intensity equivalent to 70–80% HRmax.
In total, participants in all groups (E1, E2, and C) performed five training sessions per week during the intervention. Only one training session was held per day. The remaining two days of the week included: a day of absolute rest and a day of recovery session that involved low-intensity cycling at 60% HRmax, in all participants. Weekly training volume was 11–13 hours for groups E1 and E2 and 14–16 hours for group C (identical to pre-intervention training volume). Every fourth week total training volume was decreased by approximately 50% in each group (to 5.5–8 hours of exercise) to promote recovery without modification to the exercise protocol or intensity. Power output during training was continuously measured using a rear wheel hub-mounted G3 ANT+ and GS ANT+ telemetric system (PowerTap, Wisconson, US). Heart rate was continuously measured and displayed together with power output during training with the Garmin Edge 520 and Edge 810 cycling monitor (Garmin Ltd., Kansas, US).
Testing
Physical fitness parameters and physiological variables were measured pre- and post-intervention by administering two exercise tests based on an incremental testing protocol (ITP) and a sprint interval testing protocol (SITP). The two tests were interspersed by 24 hours of rest during which the participants refrained from any exercise or training stimulus. ITP and SITP were executed in controlled laboratory conditions (temperature and humidity controlled) at the Exercise Laboratory of the University School of Physical Education (PN-EN ISO 9001:2001 certified). Testing began at 09:00 approximately 150 min postprandial.
Incremental testing protocol
The ITP was performed on an Excalibur Sport cycle ergometer calibrated before each test (Lode B.V., The Netherlands). Starting workload was 50 W and increased every 3 min by 50 W until volitional fatigue. If a participant was unable to complete an entire 3 min stage 0.28 W per second missed was subtracted from the work rate at that stage. The highest power output determined in the incremental exercise test was taken to be the measure of maximal aerobic power (Pmax). Respiratory gas exchange was measured on a breath-by-breath basis with a Quark gas analyzer (Cosmed, Italy, Mediolan). The device was calibrated before each trial with a reference gas mixture of carbon dioxide (5%), oxygen (16%), and nitrogen (79%). Tidal air was collected by wearing a face mask and analyzed to determine oxygen uptake (VO
Pre- and post-intervention work done, Pmax, and VO
in the ITP and SITP
Pre- and post-intervention work done, Pmax, and VO
Pre – pre-intervention; Post – post-intervention; W
The SITP was performed on the same Excalibur Sport cycle ergometer as in the ITP and preceded by a warm-up in which the participant cycled for 5 min at 40% Pmax (as determined in the ITP) and then for 15 min at 60% Pmax. An active 5-min cool-down was then performed by cycling at an intensity equivalent to 30 W. The test proper then began and consisted of three sets of sprint interval exercise. Each set was composed of four 30-s maximal bouts with the participant motivated to produce an all-out effort and sustain a high power output for as long as possible. The repetitions were interspersed with 90 s of active recovery in which cycling intensity was reduced to 30 W. Upon completing each set a recovery component was performed that involved pedaling with no external load for the first 2.5 min. Intensity was then increased to 40% Pmax and continued until blood pH decreased to 7.3. Arterialized capillary blood from the fingertip was drawn in order to assay pH with the use of a RapidLab 348 blood gas analyzer (Siemens Healthcare, Germany). This resulted in individualized recovery times that ranged from 25 to 40 min. A subsequent low-intensity effort of 5 min at 30 W was then performed prior to beginning the next set.
Instantaneous and average power were recorded in each sprint repetition and the work done in each set (W
A 10 ml blood sample was drawn from the antecubital forearm vein to determine myoglobin concentration (Mb) and creatine kinase activity (CK) as markers of muscular damage. A baseline measure was obtained 20 min prior to test start and a post-exertion sample was drawn 60 min after the last set was completed. Blood was immediately centrifuged to extract blood plasma. The samples were stored in Eppendorf tubes at
Data analysis
Means and standard deviations were calculated for all variables using the Statistica 13 software package (Statsoft, Poland). The distribution of the data set was screened for normality with the Shapiro-Wilk test. Data comparisons were made with the Friedman test with the Wilcoxon signed-rank test for post-hoc analysis. Pearson’s correlation coefficients (PCC) were calculated to analyze the relationship between changes in pre- and post-intervention Wtot with the changes in
Pre- and post-intervention creatine kinase activity and myoglobin concentration in the sprint interval testing protocol
Pre- and post-intervention creatine kinase activity and myoglobin concentration in the sprint interval testing protocol
Pre – pre-intervention; Post – post-intervention; CK
The assumption of normal distribution was not met for
Analysis of the biochemical markers revealed significant post-exertion increases in CK and Mb (compared with baseline values) among all groups at both the pre- and post-intervention time points (excluding pre-intervention E2). Post-intervention group comparisons showed that the increase in CK and Mb was significantly less in E1 but significantly greater in E2 when compared with pre-intervention measures. This was reflected in the delta change between baseline and post-exertion values, in which post-intervention
Correlation analysis of the changes in
Scatter plot illustrating the linear correlation between pre- and post-intervention changes in 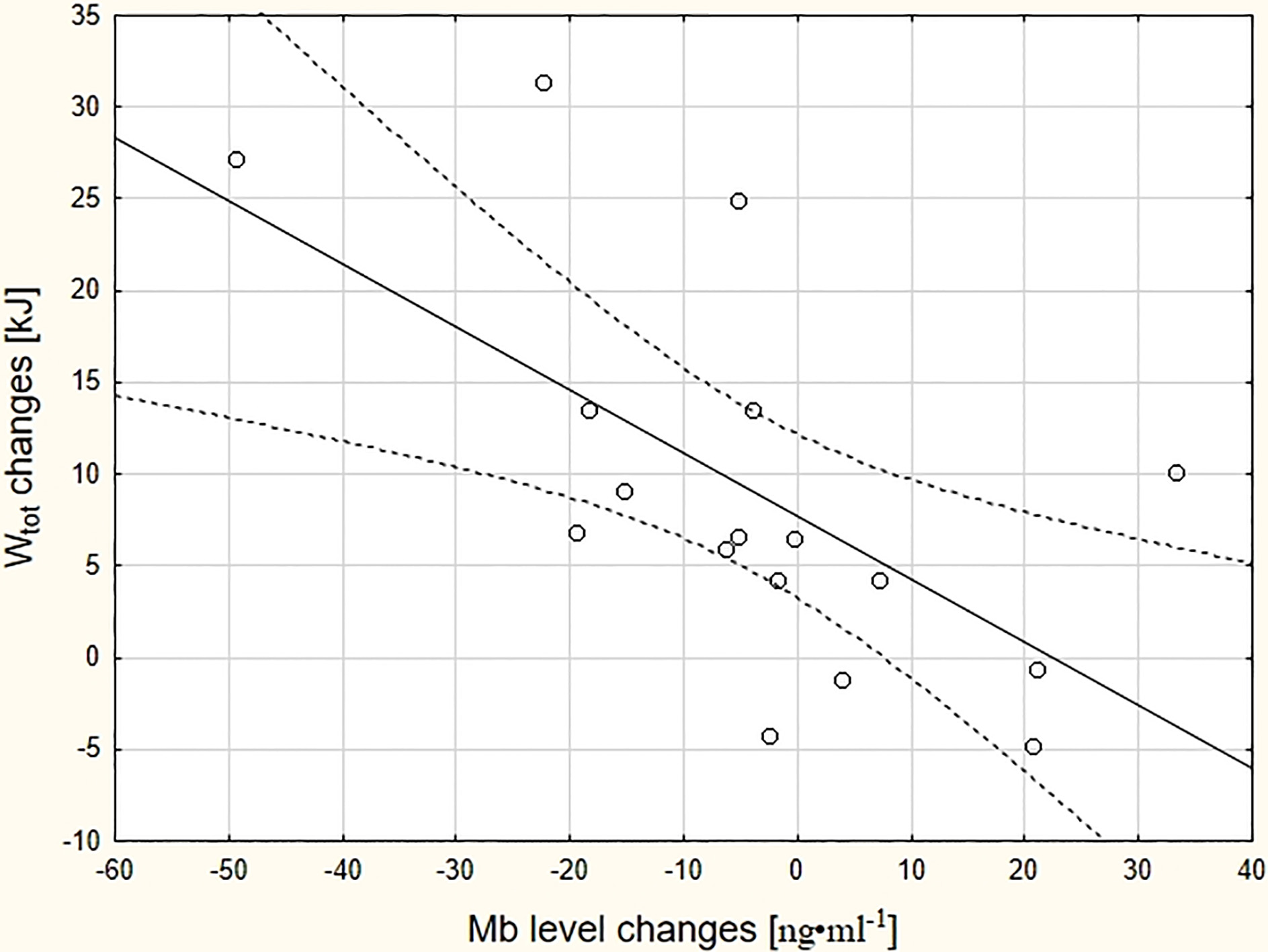
Scatter plot illustrating the linear correlation trend between pre- and post-intervention changes in 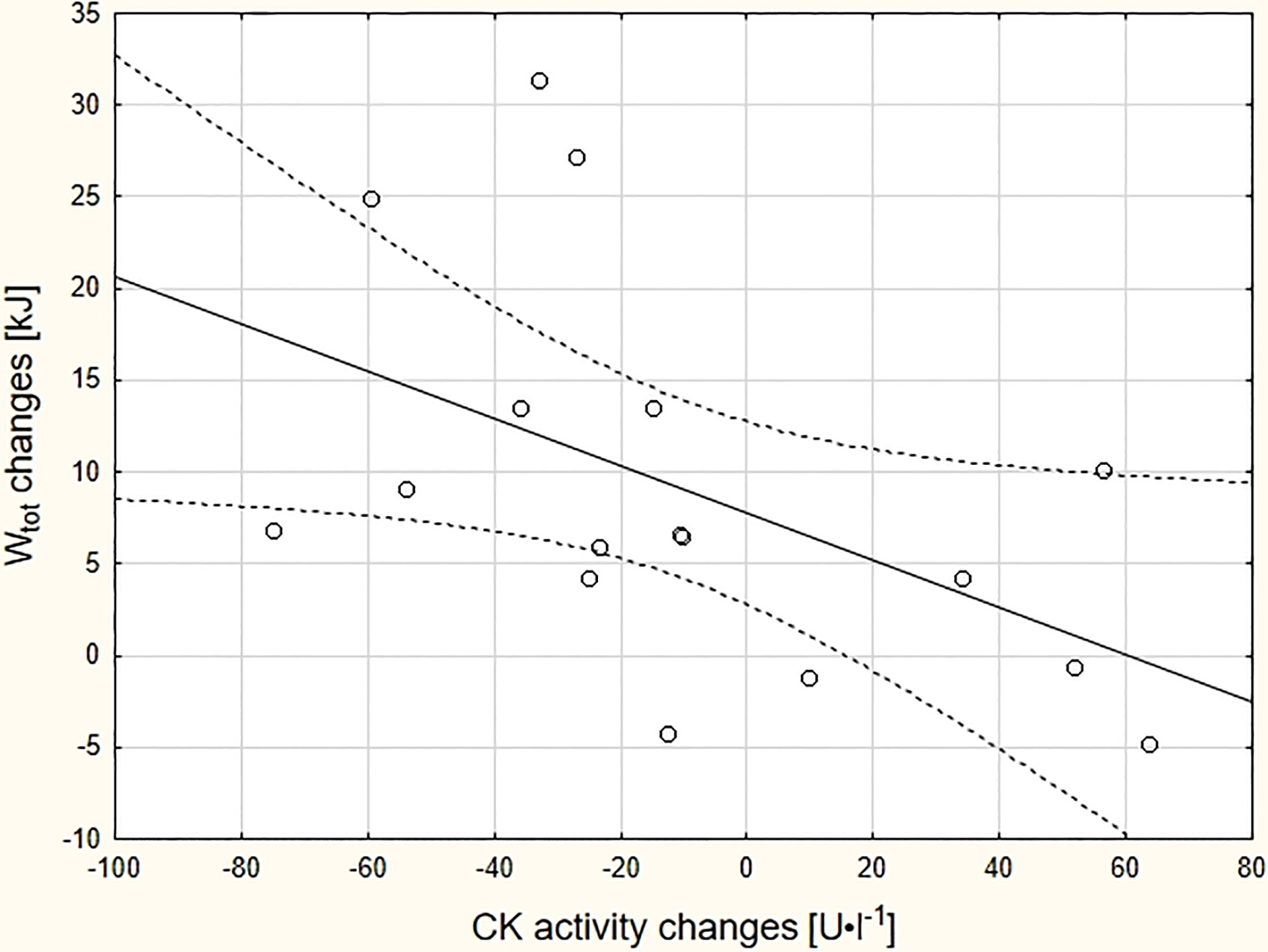
Increased Mb and CK levels were observed after the administration of SITP. Several studies have confirmed that strenuous exercise and the resultant oxidative stress can cause severe muscle damage due to metabolic [21, 25] and mechanical factors associated with excessive muscle tension or stretch [26, 27]. However, the applied exercise tests were all based on pedaling mechanics, an activity dominated by concentric muscle work [28]. While researchers have suggested that even highly intensive concentric exercise does not induce significant changes in CK and Mb [23, 29] or other biochemical markers of acute muscle damage (i.e. calpain or calpastatin) [29, 30, 31], the cited works adopted an exercise testing protocol significantly different from the one used herein. For example, Newham and Jones [23] and Vissing et al. [29] both administered an uphill walking/climbing task. While Murphy et al. [31] did use a cycle ergometer, their exercise protocol involved cycling at 70% VO
Post-intervention group comparisons revealed that the increase in CK and Mb was significantly less in E1 compared with other groups. This was also seen by the significant decrease in post-intervention
It is interesting to note the increase in CK and Mb in group E2 after the intervention was completed. Current evidence suggests that regular training should reduce susceptibility to muscle fatigue [26] and muscle tissue damage [36]. However, the differences between E1 and E2 suggest that the adaptive response to intensive training may be strongly influenced by previous high-volume endurance training background in well-trained cyclists. It may be surmised that if the training stimulus was insufficient, then the resistance to damage and also oxidative potential of muscle to short high-intensity exercise may not improve. Relatedly, the administration of intermittent sprint training to a group of untrained adults (twenty 10-s sprints performed three times per week for 5 weeks) led to enhanced Ca
Conclusions
The concomitant execution of SIT, HIIT, and CET is beneficial in the development of VO
Study limitations
The findings of the study require careful interpretation due to certain intrinsic limitations. The relatively small sample size and underlying distribution of the data required the use of non-parametric methods to compare individual sets and pre- and post-intervention. Non-parametric tests, particularly with small samples, lack the statistical power of their parametric equivalents and limit inference on the magnitude of the studied training effects. However, these limitations are difficult to overcome due to the difficulties in recruiting and retaining high-performance athletes that can execute the training intervention and highly demanding exercise tests.
Footnotes
Conflict of interest
The authors report no conflicts of interest associated with this manuscript.