
Abstract
An 80-year-old patient with diabetes mellitus, chronic bronchitis, and chronic heart failure presented with pain in the right calf after one dose of atorvastatin. Significant increases in creatine kinase, myoglobin, and potassium levels were also observed. Based on the symptoms and laboratory results, the patient was diagnosed with rhabdomyolysis. Older patients with co-morbidities may have a higher risk of statin-associated myopathy. However, there is currently no recommendation for creatine kinase monitoring in this population. This case emphasizes the need to identify high-risk populations and provide early and more frequent creatine kinase measurements to help avoid statin-associated myopathy.
Introduction
Statin therapy plays an important role in the primary and secondary prevention of cardiovascular disease. 1 One of the characteristics of statin therapy is that patients usually need long-term medication, which may cause more safety concerns. Studies have found that statins increase the risk of incident diabetes by 9% and are potentially associated with cognitive dysfunction in some populations during long-term statin treatment.2,3 However, compared to other toxicities, myotoxicity is the most common adverse event during statin therapy. 4 A retrospective study found that the average duration of statin treatment was 6.3 months (range: 0.25–48.0 months) when muscular symptoms were first noticed. 5 Other studies report a much longer time span.6,7 Here, we report a patient who developed sudden rhabdomyolysis after taking one dose of atorvastatin. This case highlights the rapid occurrence of rhabdomyolysis induced by atorvastatin. To the best of our knowledge, this is rare in statin therapy. We believe that early and more frequent creatine kinase (CK) measurements may help avoid statin-associated myopathy (SAM) in high-risk patients.
Case report
An 80-year-old Tibetan man was admitted to our infection center because of chronic bronchitis with a superimposed acute infection. His notable past medical history included chronic bronchitis, emphysema, chronic heart failure (New York Heart Association III; ejection fraction (EF): 23%), chronic atrial fibrillation, and diabetes mellitus type 2. He had 5 years of medication on aspirin (100 mg po qd), metoprolol (12.5 mg po qd), benapril (10 mg po qd), and insulin. Initial medications in our center included cefathiamidine (2 g ivgtt q8h), ambroxol (30 mg ivgtt qd), furosemide (20 mg po qd), spironolactone (40 mg po qd), and digoxin (0.125 mg po qd). After consultation with a cardiologist, warfarin (2.5 mg po qd) and atorvastatin (20 mg po qn) were initiated on the eighth day. One day after the drug adjustment (ninth institution day), the patient developed pain in the right calf. Laboratory test results showed a significant increase in CK, myoglobin, and potassium levels (Table 1). The CK levels increased by 25.8 and 47 above the upper normal limits on the third and fifth days after taking atorvastatin, respectively. Based on the symptoms and laboratory findings, we diagnosed the patient with rhabdomyolysis. Atorvastatin was discontinued, and intravenous fluids were started on the 12th day. Hyperkalemia was controlled until the potassium level was normalized. Although the treatment was not completed and the patient was still in poor general condition, he was discharged on the 14th day per patient’s request. Unfortunately, we had no follow-up data.
Patient laboratory data over time.
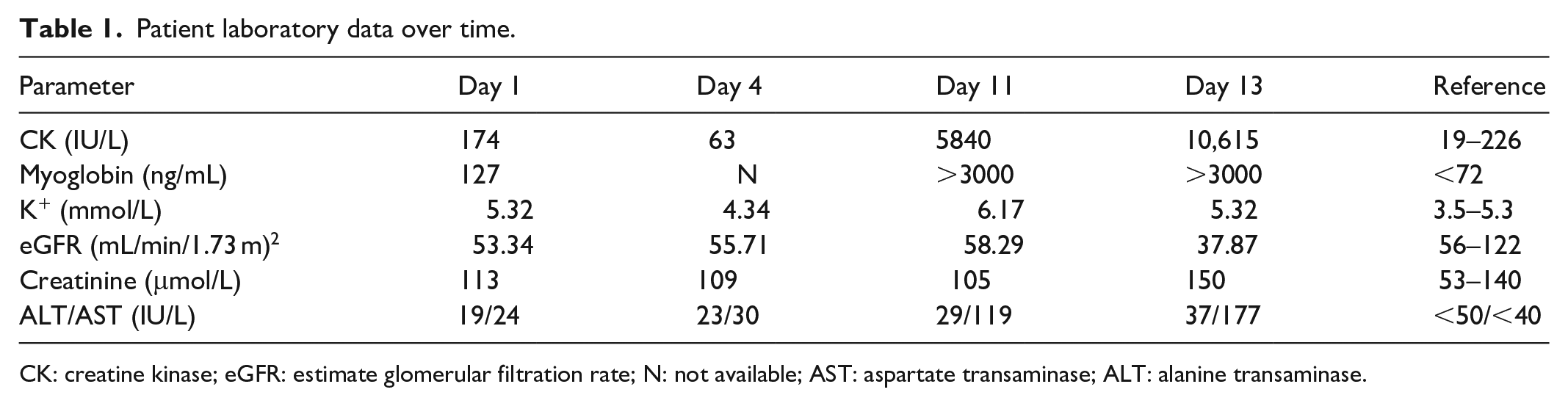
CK: creatine kinase; eGFR: estimate glomerular filtration rate; N: not available; AST: aspartate transaminase; ALT: alanine transaminase.
Discussion
Muscular symptoms usually occur after a few weeks to more than 2 years of statin treatment. 8 However, the rapid occurrence of rhabdomyolysis after taking one dose of statin in this case was rare. SAM can either be a statin-associated self-limited myopathy or a type of statin-associated autoimmune myopathy. 9 The latter is characterized by muscle weakness, high CK levels, lack of improvement after statin discontinuation, and a need for immunosuppressive therapy. 10 It can be distinguished from statin-associated self-limited myopathy based on anti-3-hydroxy-3-methylglutaryl-coenzyme A reductase antibody positivity. 9 Unfortunately, we did not identify which type of rhabdomyolysis the patient had.
The risk factors for SAM vary (Box 1). In a review of our patient’s health condition, there were many risk factors that may have led to rhabdomyolysis, such as advanced age (80 years old), multisystem diseases (diabetes and chronic heart failure), and infection. However, triggers such as liver disease, strenuous exercise, hypokalemia, and aspirin overdose could be ruled out in our patient. Pharmacokinetically, atorvastatin is metabolized by cytochrome P450 3A4 (CYP3A4). In contrast, the other drugs our patient took were neither CYP3A4 substrates, inducers, nor inhibitors. Hence, these had no apparent drug interactions with atorvastatin. Atorvastatin is mostly excreted via bile, while only about 2% is excreted by the kidney. 11 Thus, the plasma concentration of atorvastatin is not influenced by renal dysfunction. However, there were still triggers that we did not identify. First, viruses—especially influenza A H1N1—and bacteria such as Legionella are known to cause rhabdomyolysis. 12 The results of bacterial sputum cultures from our patient were all negative; however, viral testing was not performed. Thus, we could not rule out an infection contributing to his rhabdomyolysis. Second, hypothyroidism is another risk factor for rhabdomyolysis. 13 In combination with other risk factors, hypothyroidism would have supported atorvastatin, resulting in rhabdomyolysis. However, we did not test his thyroid stimulating hormone level. Third, the pharmacogenetics of statins may be also relevant in SAM. 14 The most important gene is SLCO1B1, which associates with a higher statin plasma concentration, elevated CK levels, and SAM. 15 However, gene testing was not common and our patient’s genotype was not known. In summary, these factors might have contributed to the rapid rhabdomyolysis.
Risk factors for SAM.

Source: Adapted from Stroes et al. 16
The incidence of SAM is approximately 5% in clinical trials. 17 However, patients enrolled in clinical trials are typically younger and healthier. 18 The risk of SAM in patients aged over 80 years with co-morbidities has not yet been evaluated. Thus, further studies are needed to determine whether these populations are at a higher SAM risk. 18
This case raised the question of how to prevent and predict SAM in patients at higher risk. To the best of our knowledge, there are no drugs to prevent myotoxicity. However, the biomarker CK could help predict myotoxicity. The American College of Cardiology/American Heart Association/National Heart, Lung, and Blood Institute have recommended baseline CK measurement and a repeat CK measurement when muscular symptoms occur. 17 The Canadian Cardiovascular Society has also recommended CK measurement whenever the initial statin is switched to a higher dose or to a different class, and whenever muscle complaints occur. 19 These comparative values may aid in clinical decision-making. However, these two guidelines only recommend CK measurements before starting statin use and after muscle complaints happen, without contemplating on the different risks of SAM in patients. The European Society of Cardiology did not recommend routine CK monitoring either, citing that CK elevation was rare during statin therapy and other risk factors may lead to muscular symptoms. 16 Thus, there is no consensus on CK monitoring, especially in populations with a higher risk of SAM.
Conclusion
In summary, our case highlights the need to identify high-risk populations and perform early and more frequent CK measurements in these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.