
Abstract
BACKGROUND/OBJECTIVE:
The purpose of this study was to examine muscle damage and EMG responses during recovery period following exhaustive concentric and eccentric contractions.
METHODS:
Fifteen football players participated in this study. In order to evaluate the recovery period after the muscle damage exercise protocol, the expected damage was provoked by concentric and eccentric contractions. The EMG data obtained from Rectus Femoris muscle and levels of CK, LDH, and Myoglobin analysed from plasma were recorded before, immediately after and post 24
RESULTS:
Save a significant change in the maximum EMG value of Rectus Femoris muscle, no difference was found among other variables (
CONCLUSIONS:
As a result, various EMG measures and muscle damage responses were recorded during the recovery period after intensive resistance exercises. However the responses during recovery period did not differ by the contraction type.
Introduction
Exercise-induced muscle damage is one of the most common symptoms after extreme, unusual exercise [1]. However, not every exercise cause muscle damage, the degree of muscle damage may vary according to type and intensity of the performed exercise. The eccentric contraction causes more muscle damage than the concentric contraction. Two theories come forward to explain that why the damage caused by eccentric contraction is more than that of the other kind of contractions. Firstly compared to concentric contraction, the same workload and the amount of active motor unit in kinetic phase during eccentric contraction are reduced by 1/5. Therefore, the increase of the load per fibril during eccentric contraction also brings mechanical tears with it. The second theory is the occurence of the tears caused by extension of muscle under stretch during eccentric contraction. Motor units, which are shorter than normal, may be torn because they are forced to extend more in the eccentric contraction [2].
Two frequent methods are used to detect muscle damage. These are direct methods including visualization techniques such as magnetic resonance spectroscopy, micrography, electron microscopy and indirect methods which includes the determination of intramuscular enzymes rates in plasma. Not only is the direct method costly and difficult to apply to the field, but also biopsy technique used in some types of this method when there is a necessity for conducting a biopsy, can affect the results. But in the indirect method, which is an easier and more practical method to perform, the degree of muscle damage is determined by measuring the amount of intramuscular enzymes and the increased protein in the plasma after exercise [3].
In order to determine muscle damage after exercise, serum creatine kinase (CK), lactate dehydrogenase (LDH), aspartate aminotransferase (AST), alanine aminotransferase (ALT), myoglobin and neutrophil percentage ratios were widely used in the studies [4, 5]. Serum CK activity elevation also observed when muscle damage occurs after exercise, as well as in conditions of muscle injury and usage of proteins as an energy source [2, 6]. CK is the most active substance in skeletal muscle. CK activity in exercise-induced muscle damage is affected by many variables such as gender, age, and type of exercise [2]. The rate of increase in CK activity is higher in males and it is observed that this rate increases more rapidly with aging [7, 8]. The peaking time of increasing CK after exercise changes depending on exercise type, intensity, and duration. It is reported that the highest level of CK is observed in 1–5 days after exercise [2].
Muscle cells create electrical potentials during contraction. Musculoskeletal activity can be determined by recording changes in these electrical potentials using an electromyography (EMG). EMG results do not give the type and resultant force of contraction, but provide information about engaging muscles and motor nerves as a result of the analyses of motor unit action potentials. In addition, EMG is also used to evaluate muscular tension during isometric or dynamic exercises or to determine the degree of fatigue [9].
In the literature, there are many studies evaluating muscle damage caused by eccentric and concentric contractions in the athletes with blood enzyme anal- ysis method. Also, it was observed that studies analyzing the recovery process after eccentric and concentric contraction by Semg were more uncommon. In addition, the effect of muscle damage, occurred after exercise, on muscle activation was not fully understood [10]. From this point of view purpose of this study was to investigate muscle damage and EMG responses during the recovery period following exhaustive exercise composed of concentric and eccentric contractions.
Methods
Subjects
Fifteen voluntary athletes playing football regularly aged between 18 and 25 years, were included in the study. Athletes, who have an acute or chronic disease, had an injury of the lower extremity in the last six months and have unstable cardiovascular status, were not included in the study. The study was completed with 10 athletes, since 5 of the 15 athletes were excluded because they did not follow the exercise protocol. For this study, necessary permission was obtained from the University Ethics Committee for Clinical Researches (2010/53) and the athletes signed a written approval form after being informed about the study.
The average EMG max values of the Rectus Femoris muscle
The average EMG max values of the Rectus Femoris muscle
Base: Pre exercise baseline value, PE: Post exercise.
EMG max. Averages over time obtained from Rectus Femoris muscle in concentric and eccentric contractions.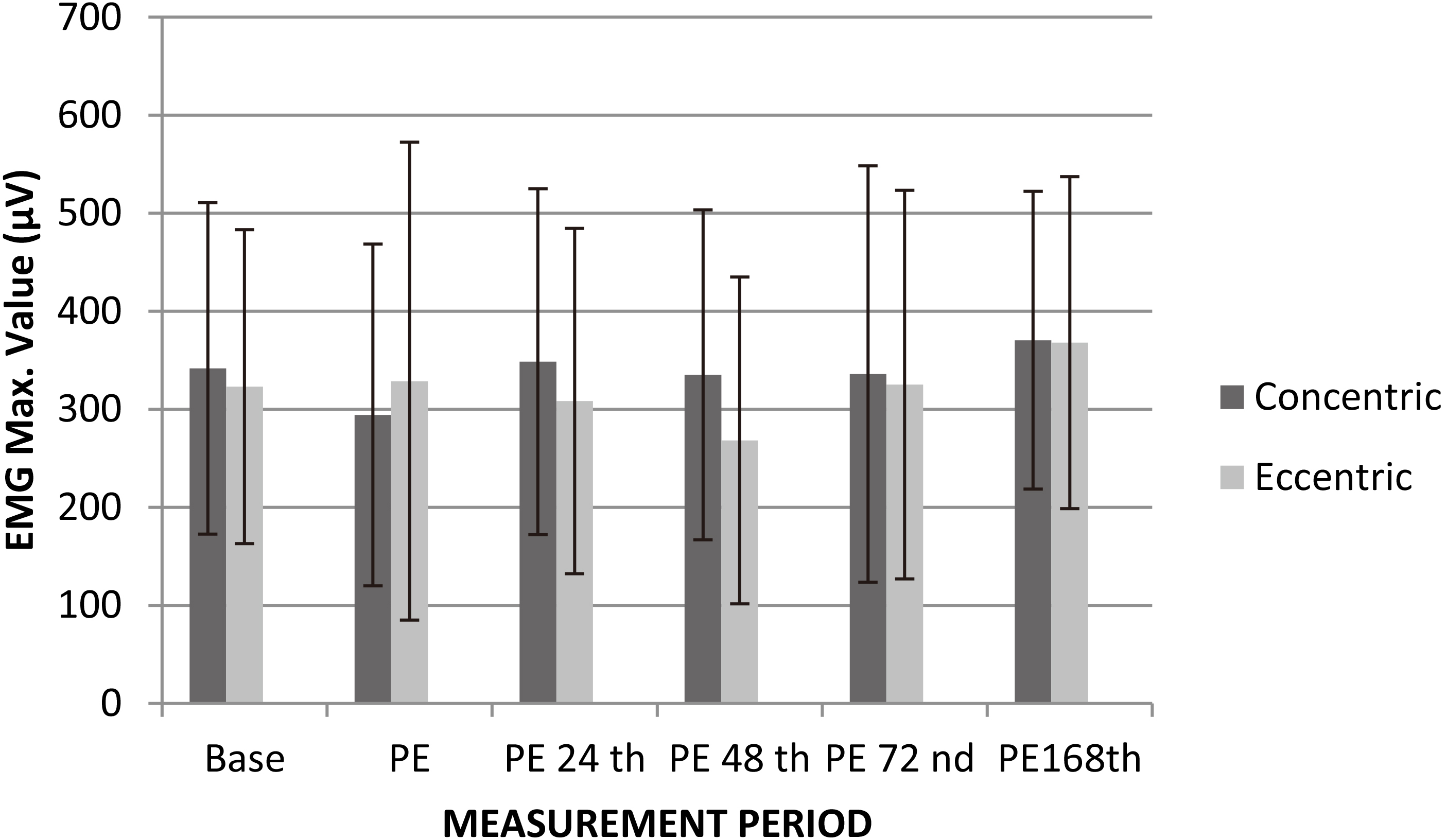
The muscle damage exercise protocol was applied in 2 different ways to the athletes participating in the study. Athletes were involved in a muscle damage protocol with concentric contractions and a protocol with eccentric contraction in a randomized crossover design with one-week interval. The athletes were informed about not doing any physical activity or a heavy work during 48 hours before starting exercise protocol and during 168 hours following the start. The exercise program started with warming up exercises consisted of jogging (5 mins); stretching m. quadriceps femoris (10 repeats), hamstring (10 repeats) and m.triceps surae (10 repeats); marching by pulling knees up (2–3 mins). Pre-study was performed on ten atheletes for the determination of appropriate force loading on twenty five repetition [11, 12] of eccentric and concentric contraction before starting the exercise protocol. As a result of pre-study, it was determined that the concentric and eccentric contraction should be in order by the 70% and 100% of the one maximum repetition. To determine the reference value of the m. rectus femoris measurements were performed by using Myomed 932 surface EMG device and maximum (
Immediately after the exercises finished, the EMG values were measured again and the blood was retaken at the 5
Statistical analysis
Mean and standard deviations of the obtained EMG data and blood analysis results were calculated as descriptive statistics. Two-way analysis of variance with repeated measures (contraction type X time) was performed to determine the difference between contractions. Contrast analysis was performed to test the change over time. The Friedman test, which is the nonparametric counterpart of the variance analysis with repeated measures, was applied to data, not including parametric conditions; Wilcoxon test was used for binary comparisons after the Friedman test. the alpha significance level was accepted as
Results
The age, height and body weight of the ten athletes were 23.1
The average EMG values of the Rectus Femoris muscle of the athletes are given in Table 1.
The results of two way ANOVA with repeated measures regarding the EMG Maximum (Max) values of Rectus Femoris muscle showed significant main effect for time [F (5–90)
When the change over time was examined according to Base by defining contrast after analysis of variance; a significant difference was found only from Base to 1
The averages of blood analysis values of the athletes (CK, LDH, Myoglobin) were shown in Table 2.
The averages of blood analysis (myoglobin, CK, LDH) values of the athletes
The averages of blood analysis (myoglobin, CK, LDH) values of the athletes
Plasma CK level averages over time after concentric and eccentric contractions.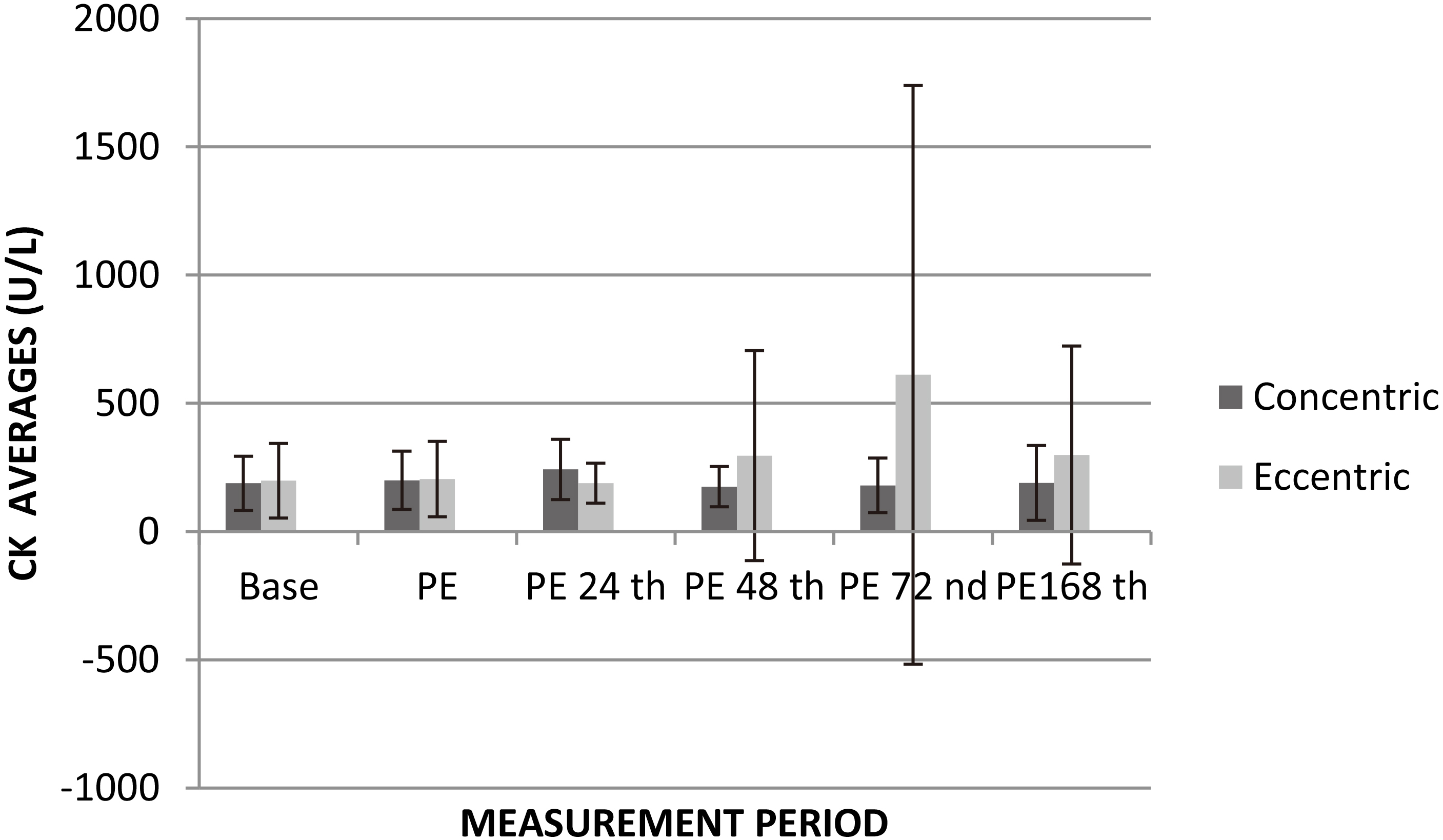
Plasma LDH level over time after concentric and eccentric contractions.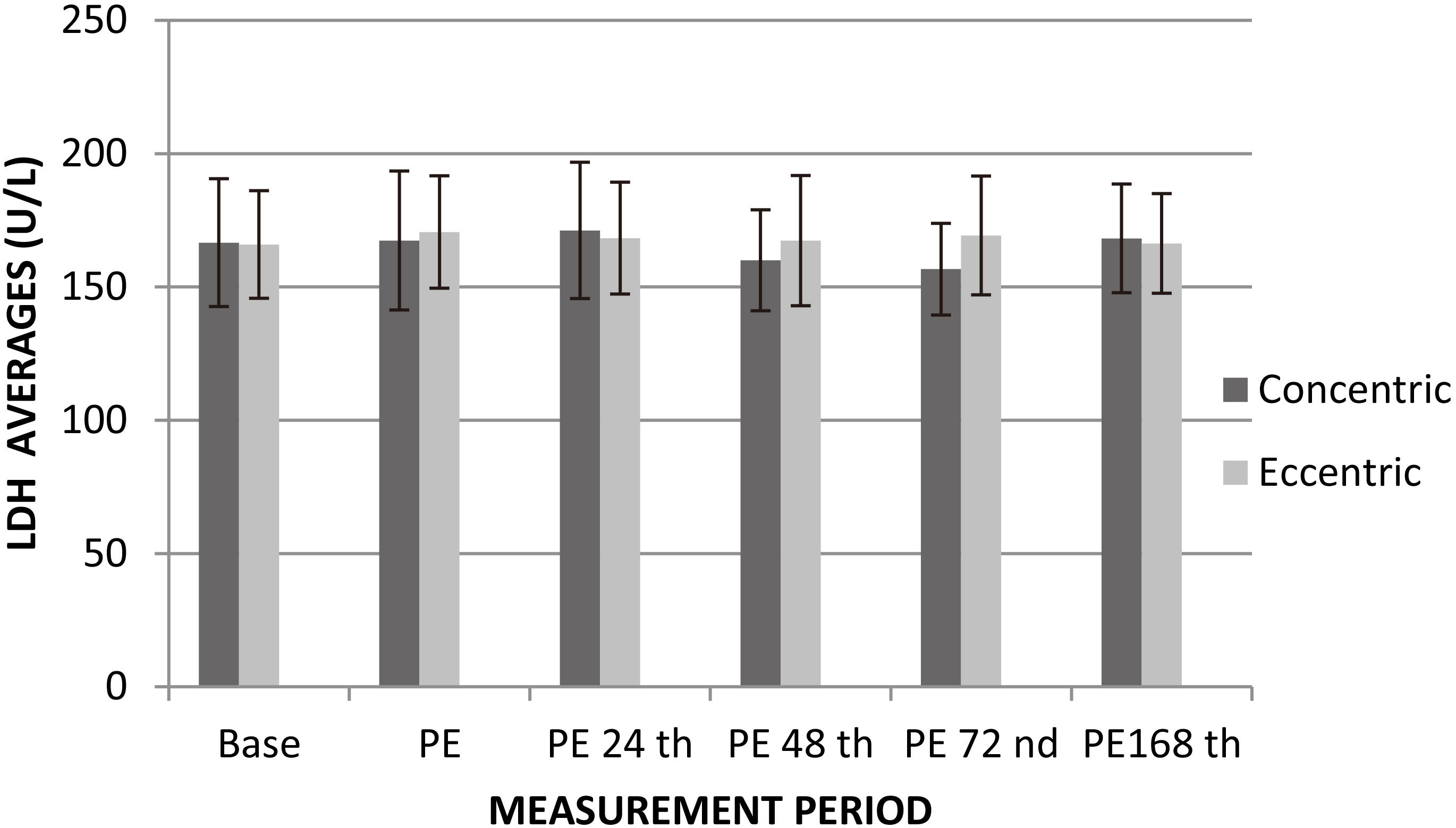
Plasma Myoglobin level over time after concentric and eccentric contractions.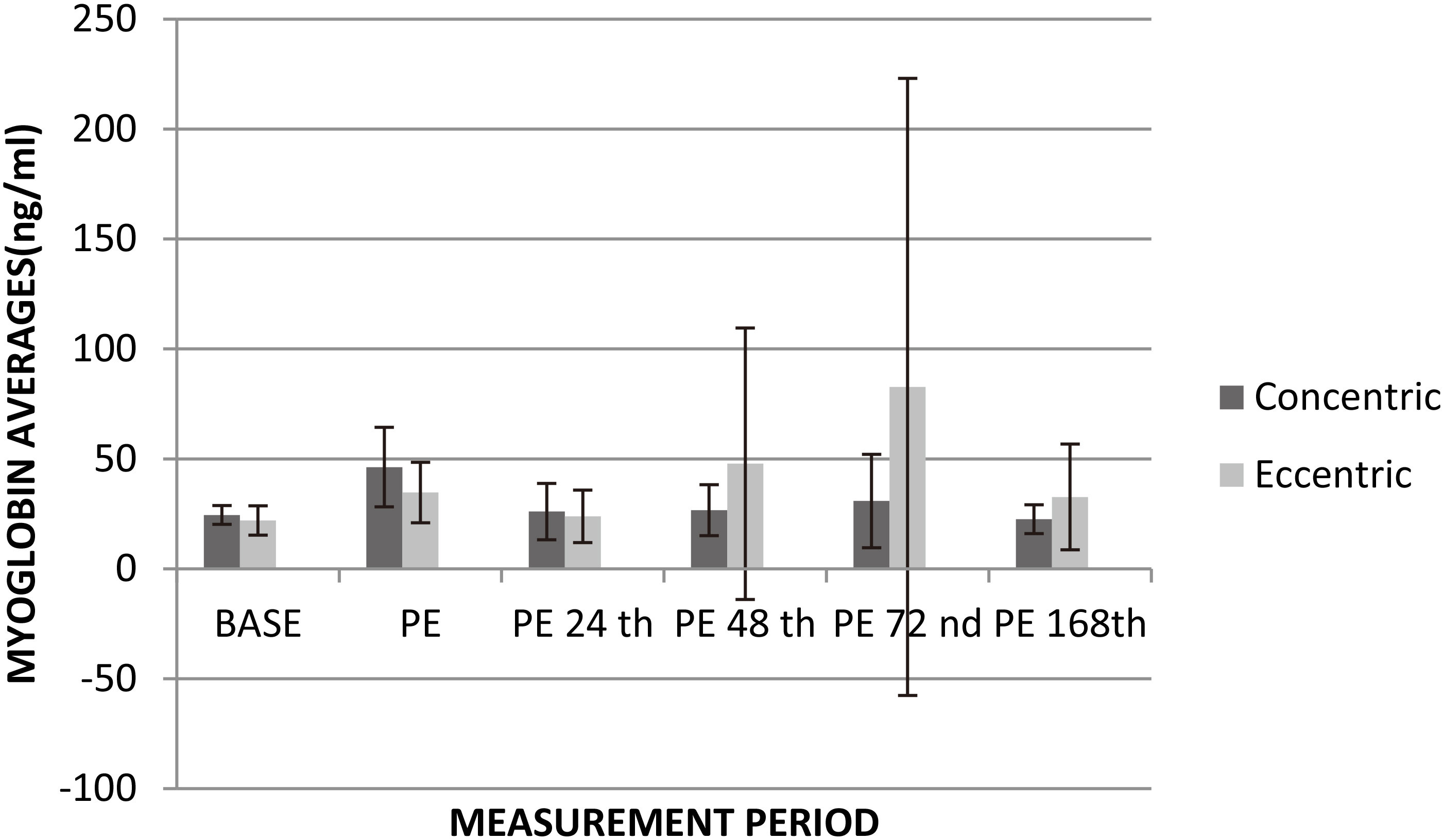
The Friedman test, which is a nonparametric counterpart to variance analysis with repeated measures, was applied to plasma CK levels. According to the Friedman test, difference was detected in the change of CK levels over time in the concentric exercise. However, in binary comparisons, no difference was found between the base and repeated measurements after exercise. Similarly, there was also no significant difference in eccentric contractions. Although the change of CK levels over time, measured with two different contractions and at six different times were similar; it was observed that the CK elevation after eccentric contractions started substantially at the 48
Two way ANOVA with repeated measures applied on plasma LDH levels showed no significant main effect for time [F (5–90)
Two way ANOVA with repeated measures applied on plasma myoglobin levels showed no significant main effect for time [F (5–90)
Recovery period (168-hours) following muscle damage exercise protocol was examined to determine the muscle damage caused by exhaustive concentric and eccentric contractions in the quadriceps muscle groups. As a result of comparison of pre-exercise and one week later assessment, significant difference was found in EMG max value of rectus femoris overtime. Despite no significant difference was found in CK, LDH and myoglobin values overtime, especially peak values were observed at 48 and 72 hours in CK and myoglobin values.
Myoglobin, CK, LDH, AST, CK-MB, sEMG and muscle soreness parameters are noticed to be used in studies examining muscle damage and recovery in the literature [13, 14, 15, 16, 17, 18, 19]. Plasma, CK, LDH and Myoglobin levels and max. values of EMG measured by superficial electrode were used in the present study to examine the recovery period after exhaustive muscle contractions.
In this study, sEMG values were measured during the 1-week period after muscle damage exercise protocol intervention. Maximum EMG values of Rectus Femoris muscle reached and also passed base in 168-hour period after both concentric and eccentric contractions. The EMG max values at the base, post-exercises (PE), PE24
However, in this period of controlling the change over time, it is observed that the difference occurs in the sEMG values, not in the muscle enzymes. This finding demonstrated that sEMG values of one week recovery period are not compatible with the blood enzyme values and also sEMG may not give accurate results about the muscular damage in long-term recovery period follow up. In the literature, there are also similar studies reporting that sEMG is not a suitable method for evaluating the late period of recovery after muscle damage [20].
In a study using the CK level to examine muscle damage concluded that plasma CK upper limit as a practical and alternative method for the early detection of excessive load on the muscles of football players [21]. In another study in which an eccentric exercise program was applied; plasma CK level, muscle pain, and stiffness were measured one day before and after the exercise, and the difference was found in these parameters [22]. In the study of Hazar et al. [23] examining plasma CK level after using exercise equipment for the upper and lower extremities, it was detected that the plasma CK levels began to increase immediately after the training, peaked 24 hours after the training, began to decrease at 48
Whether it is statistically not significant it was observed that the PE plasma CK levels (24
LDH is a muscle enzyme that is often used together with CK to examine the muscle damage in the literature. It is known that LDH is not as sensitive to muscle damage as CK. For instance, in a study significant increase in CK, CK-MB and Myoglobin were observed whereas there is no change in blood AST and LDH after exercise [32]. While the highest change was observed in tripled Myoglobin, AST was multiplied by 1.1 and LDH 1.3 [33]. In the present study no difference was found between plasma LDH levels at Base and PE 24
There is a study reporting that the concentration of myoglobin peaks immediately after muscle damage earlier than CK [34]. Although it is statistically not significant there was difference between plasma Myoglobin level at Base and following exercise especially at 48
Conclusion
In conclusion, it seems that muscular damage caused by concentric and eccentric contractions have similar recovery process. Analysis of recovery process reveals that EMG max values of both contraction types only differentiate in the period of Base and the week following assessment. No significant difference was observed in blood enzyme samples. In this study The number of football players evaluated was inadequate, and this situation can be the possible reason why there is no difference in the majority of the change in blood analysis parameters over time. Application of the exercise just with the dominant leg to create muscle damage was the next limitation of this study. Not using direct methods such as ultrasound, MR and more specific methods for screening the muscle damage in exercised tissue, can also be regarded as another limitation.
Footnotes
Acknowledgments
This work was supported by the Scientific Research Project Unit of University (Project number: 2011.16. 03.429).
Conflict of interest
The authors declare no conflict of interest.