
Abstract
We report the case of a sixteen-year-old high-performance sprinter with an ischial tuberosity avulsion. In these injuries, most of the published literature recommends surgery when the diastasis exceeds 2 cm. Our patient had a 1.9 cm diastasis and was treated conservatively. Various criteria are used to demonstrate recovery after treatment. However, one of our main recovery criteria is functional assessment by isokinetic dynamometry. Whilst the first test showed significant strength imbalance, following rehabilitation hamstring strength underwent substantial normalization despite the absence of radiological healing. The patient resumed competition successfully less than one year after the injury with performance levels which were almost the same as before the injury. This case suggests that functional recovery of the hamstring may be added to radiological assessment as an important rehabilitation criterion and that hamstring strength should be measured accurately and objectively in a preventive approach.
Introduction
Apophyseal avulsion fractures of the pelvis are common among the teenage athletes and ischial tuberosity avulsion (ITA) appears to be the most frequent [1]. Usually, these avulsions are the result of a sudden forceful concentric or eccentric contraction of the muscle attached to the apophysis. Indeed, before ossification, the apophyseal growth cartilage is the weakest point in the musculotendinous unit. With respect to ITA, it is produced, most of the time, by a sudden flexion of the hip with an extended knee. Athletes most commonly affected are gymnasts during floor exercises which impose sudden and excessive lengthening, soccer players when they tackle or shot powerful at goal [1] or water skiers when the ski decelerate and the body maintain its course [2]. The treatment can be conservative or surgical.
Isokinetic strength profile before and after rehabilitation.
Isokinetic strength profile before and after rehabilitation.
A sixteen-years-old high level sprinter (100 m –200 m), while training, felt an acute pain at the ischiatic tuberosity that had compelled him to stop immediately the activity. A few days prior the injury, he had already felt discomfort in this location. Three months after the injury he presented at our physiotherapy departmental clinic. A clinical examination showed moderate elective pain upon ischial palpation and a manual eccentric hamstring testing was moderately painful. He had already had an X-ray which revealed a secondary ossification opposite the ischial tuberosity (Fig. 1a). The patient’s age, the clinic and the X-ray was typical of an ischial avulsion fracture. The maximal diastasis was 1.9 cm. According to most publications [3, 4, 5], surgery is advisable from 2 cm of diastasis; 1.9 cm was within the range of either a surgical or a conservative approach. Three months after the injury, the surgery would have been difficult because of substantial scar tissue formation. Therefore the conservative approach was applied. The patient had already been at rest for three months and he was then allowed to resume low-impact activities.
a. First pelvis X-Ray: ischial avulsion with a 1.9 maximum diastasis. b. Last pelvis X-Ray: persistence of ischial avulsion.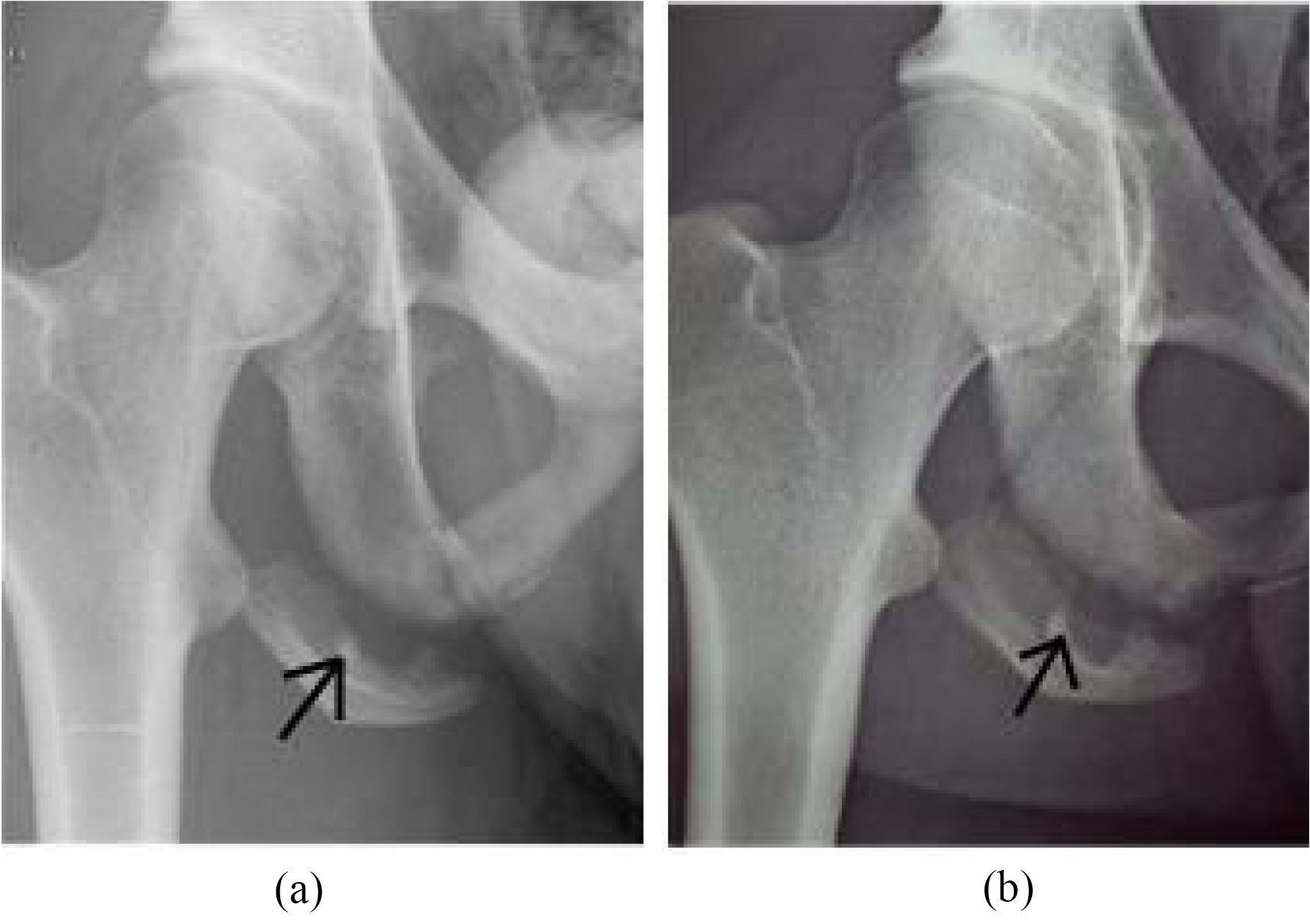
Four months after the first consultation in our department, the patient returned for consultation to check progress. Regarding the radiological findings, we observed no change since the previous X-Ray (Fig. 1b). However, clinically, he was asymptomatic and eccentric contraction was painless. An isokinetic assessment was planned two months later, i.e. 9 months after the initial injury. The isokinetic testing highlighted moderate to severe hamstring strength imbalances due to a bilateral difference of 31% in the concentric and 28% in the eccentric tests. The DCR (Hecc
Six weeks later, the same isokinetic assessment was repeated, showing significant improvement of right hamstring strength, particularly for eccentric contraction (Table 1). The greatest improvement was the DCR which had increased from 0.8 to 1.44. Further specific strengthening was recommended and intensifying training on the field was allowed in order to resume competition.
Four months after the termination of treatment the patient trained four times a week and participated again in competitions. His performance in sporting activities has reached pre-injury level.
ITA is an easily missed diagnosis. Indeed, the clinical picture can be frequently confused with proximal hamstring injury [6] and hence, recognition of the fracture is necessary to determine the most relevant lesion’s management. Ischial pain, with bony tenderness or even a palpable gap, in a teenage or young adult should always lead to an X-Ray [6]. The present clinical picture, with progressive pain followed by an acute pain, may indicate that microtraumatic damages could have been present before the avulsion fracture [7]. At the ischial tuberosity, the osteochondrosis resulting of repeated tractions on the hamstrings is named McMaster and can lead to an avulsion if a stronger trauma occurs [7]. Moreover, one cannot rule out that the ITA occurred on a bone previously weakened by an osteochondrosis.
Several studies discuss the surgical versus conservative approach for treatment of ITA and most advocate surgery when the diastasis exceeds 2 cm [3, 4, 5]. Indeed, apophyseal fractures may lead to prolonged pain, muscle weakness and reduced sport performances if the management of a widely displaced fracture remains conservative [6, 8]. Surgery would be also advisable when the avulsion cause prolonged complains because of pseudarthrosis [4]. However, some other studies advocate conservative treatment regardless of the importance of avulsion [8, 9] while emphasizing that surgery alone is not sufficient for recovery [11]. Our patient, with a 1.9 cm diastasis, was ‘caught in the middle’ between conservative and surgical approach.
Different criteria are used by authors to determine recovery after management of ITA. Most are based on pain relief or ability to perform in sport [6, 9, 11]. No study accurately measured the hamstring strength before and after treatment. However, strength imbalance, especially the DCR, significantly increases the risk of sustaining hamstring injury [12]. In the present case, we believe that the increase in the DCR from 0.8 to 1.44, significantly decreased the risk of recurrence of hamstring injury [12]. However, regarding X-Ray imagery, there was no evidence of healing but the avulsion persistence on the X ray did not seem to impede functional recovery. Remission and ability to return to competition should be based on clinical criteria combined with an objective measurement of muscle performance.
Footnotes
Conflict of interest
None to report.