
Abstract
Various surgical techniques exist to approach an ischial tuberosity avulsion fracture, including open reduction and internal fixation with screws and suture anchors, augmentation with allograft tendon, and excision of the fragment. However, the majority of these techniques approached acute fractures, and nonunions were not addressed nor studied. This case series describes two adolescent patients treated for ischial tuberosity nonunions with a posterior column screw through a subgluteal approach. Both patients demonstrated radiographic healing of their nonunion sites at 6 months’ follow-up. Each patient reported no pain during activity, had symmetric hamstring strength, and were able to return to pre-injury level of activity by final follow-up. In conclusion, the authors utilized a muscle-sparing approach to the ischial tuberosity nonunion site through a cosmetically appealing incision and introduced a novel approach to nonunion fixation without the use of bone graft, resulting in excellent clinical outcomes.
Introduction
Ischial tuberosity avulsion fracture is an uncommon injury with controversial treatment strategies. 1,2 The majority of such injuries have delayed diagnoses, and there is no standardized treatment algorithm. Displaced fractures treated nonoperatively can develop into nonunions or pseudotumors, can be a source of continued pain and immobility for young athletes, and may prevent them from returning to their sport. 3 Due to these, it is important to manage these rare injuries with a reliable treatment.
This case series describes an innovative surgical technique for the treatment of ischial tuberosity avulsion fracture nonunions with a posterior column lag screw utilizing a modified subgluteal approach. This technique minimizes surgical dissection through a muscle-sparing approach and utilizes a large 6.5-mm partially threaded cannulated screw that is placed as a retrograde posterior column screw as described previously. 4 This is placed alongside 3.5-mm cortical screws across the fracture to avoid screw loosening and pullout.
Materials and methods
This study was reviewed by the authors’ hospital’s institutional review board prior to initiation and was granted an exemption. A retrospective review was performed of two adolescent patients who were treated for ischial tuberosity nonunions with a posterior column screw by a single fellowship-trained orthopedic trauma surgeon between January 2015 and January 2017. Each patient was informed that data concerning the case would be submitted for publication, and they verbally agreed to participate. Inclusion criteria included age <18 years, treated with a posterior column screw via a subgluteal approach, and having at least 6-month radiographic and clinical follow-up. Exclusion criteria included age >18 years with insufficient follow-up. Two patients, both under the age of 18, were identified and enrolled in this study.
Each patient had a preoperative computed tomography scan and a radiograph of the pelvis, as well as a clinical exam including hamstring strength testing and visual analog scale (VAS) pain scores. The patients were seen at the 6-week, 3-month, and 6-month time points postoperative. At each of these subsequent visits, pelvis radiographs were obtained, and VAS pain scores, hamstring strength testing, and activity level were documented.
Surgical approach
The patients were placed under general anesthesia and positioned in the prone position. The involved posterolateral thigh was prepped and draped. A 10-cm transverse incision along the gluteal crease was made (Figure 1). The gluteus maximus muscle and fascia were elevated proximally, and the muscular plane between the gluteus maximus and hamstrings tendon was developed. The sciatic nerve was identified just lateral to the ischial tuberosity and protected with a retractor. The ischial nonunion site was identified. The hamstrings tendon was attached to the mobile non-united fragment. The fragment was freed from scar tissue and mobilized; the knee was subsequently flexed, and the hip extended in order to relieve tension off the sciatic nerve and allow appropriate, gentle retraction laterally. A burr was utilized on the nonunion site to expose a bleeding cancellous bed of bone. A point-to-point clamp was placed into the obturator foramen and onto the non-united ischial fragment to obtain bony contact. Following this, the authors percutaneously placed a retrograde posterior column lag screw with the 6.5-mm ASNIS cannulated screw set (Stryker, Warsaw, Indiana, USA) by using a combination of inlet, outlet, and Judet views of the pelvis (Figures 2 and 3). 5,6 This was found via fluoroscopy to be safely located within the posterior column, and the screw provided excellent compression. The authors supplemented this with 3.5-mm cortical screws across the nonunion site under direct visualization. The site was found to be stable. The knee was extended, and the nonunion showed excellent compression. The wound was then closed in layered fashion with a subcuticular monocryl closure to the skin.
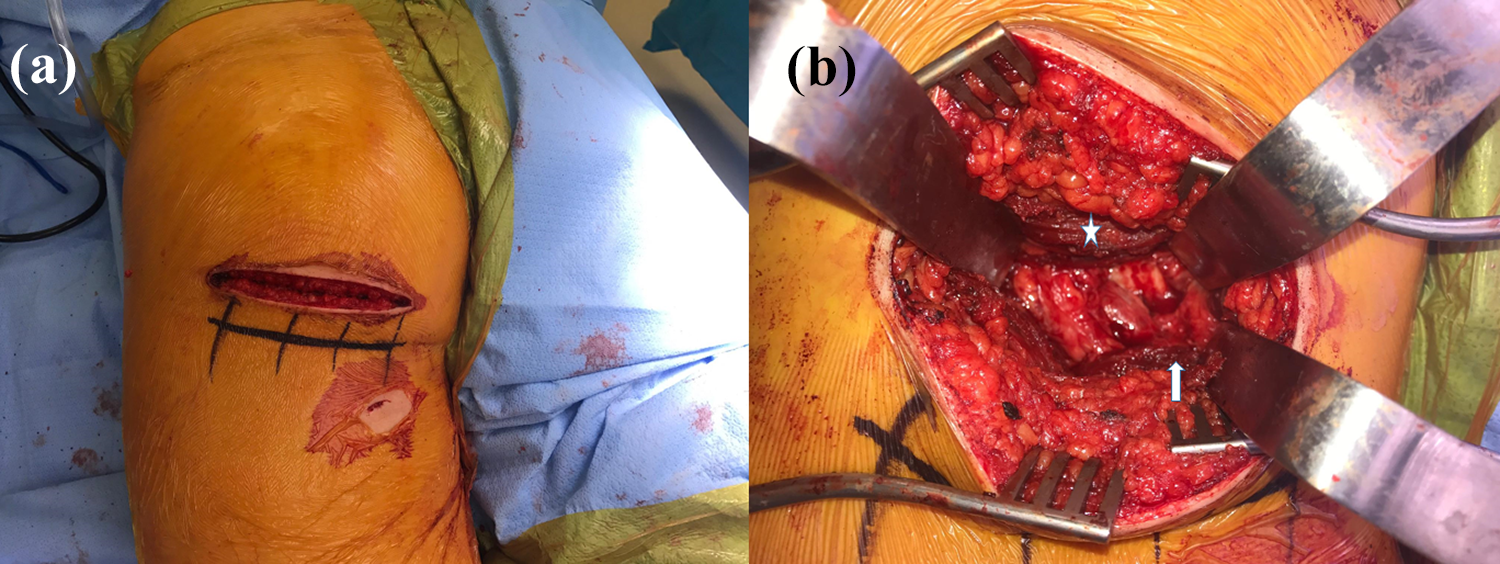
Modified subgluteal approach. (a) A 10-cm transverse incision was made along the gluteal fold. The small 0.5-cm incision for the percutaneously placed 6.5-mm ASNIS screw was also visible distally to the main incision. (b) The muscular interval between the gluteus maximus (star) and hamstrings muscles (arrow) is then developed. The sciatic nerve was identified and gently retracted laterally to gain full visualization of the nonunion site.

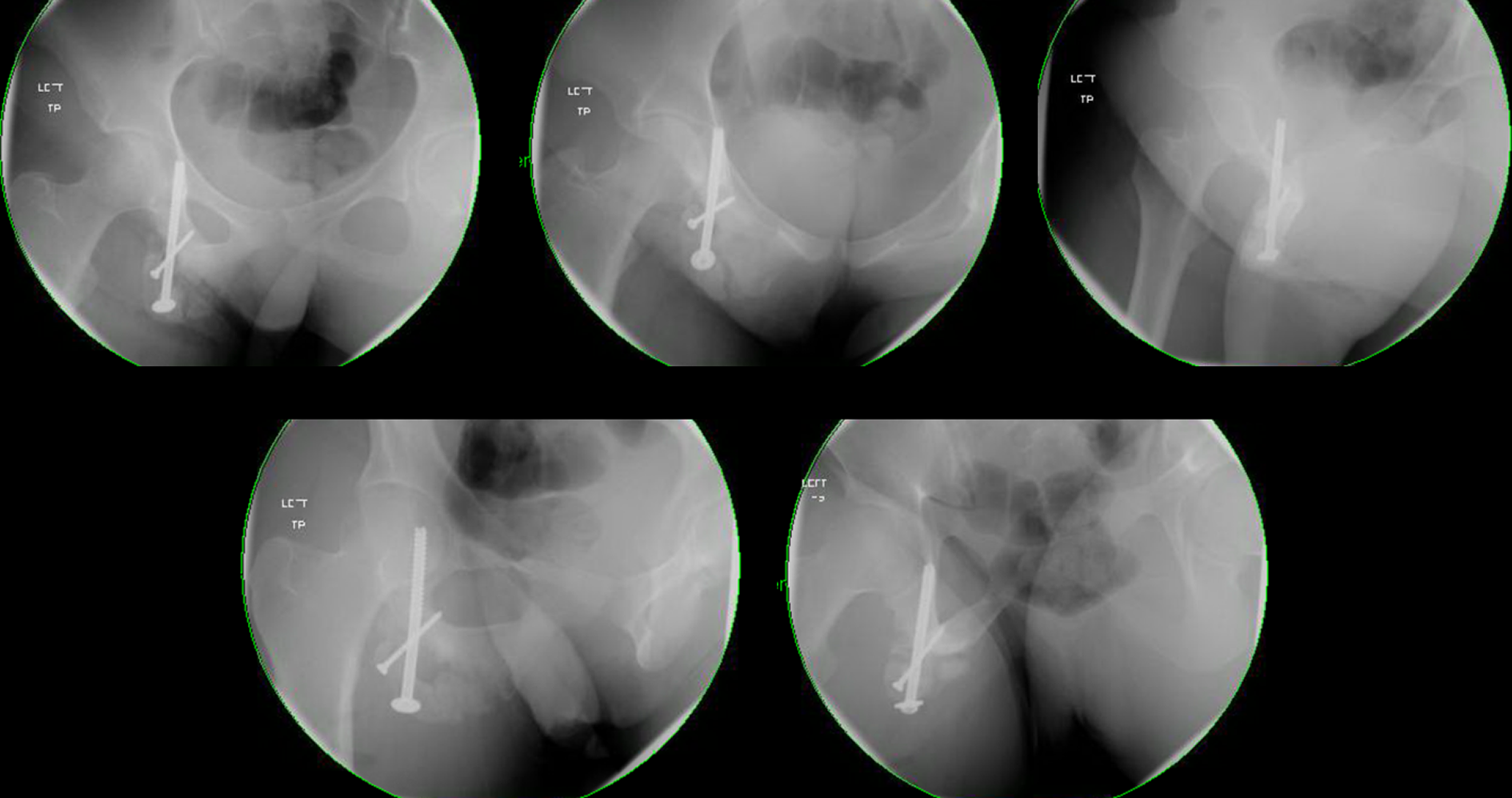
Case 1 intraoperative radiographs. Fluoroscopic images including inlet, outlet, and Judet films of the pelvis after instrumentation. The posterior column screw is safely placed within the bony corridor along with three separate 3.5-mm cortical screws across the nonunion site.
Case 2 intraoperative radiographs. Fluoroscopic images included inlet, outlet, and Judet films of the pelvis after instrumentation. The posterior column screw is safely placed within the bony corridor along with a separate 3.5-mm cortical screw across the nonunion site.
Case reports
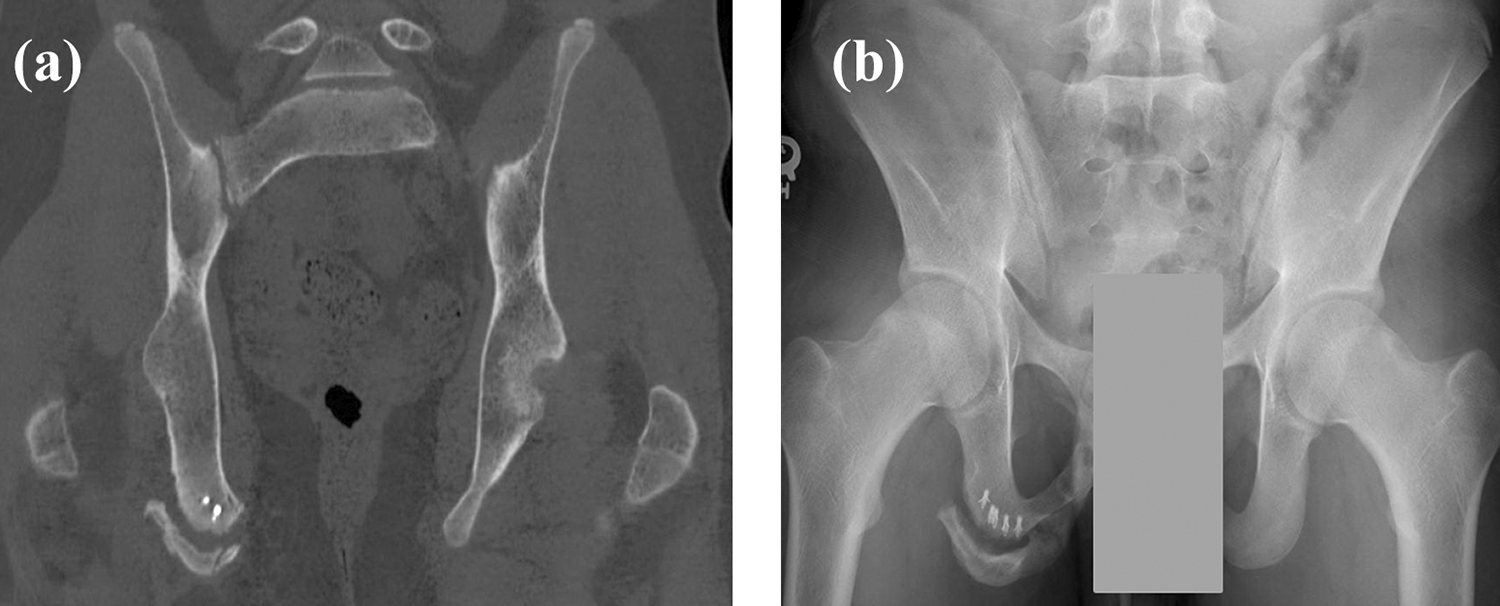
Case 1 preoperative radiographs: (a) and (b) are the preoperative computed tomography scan and anteroposterior radiograph, respectively, of a 16-year-old boy with an ischial tuberosity nonunion. The patient had a history of primary fixation of his proximal hamstrings avulsion fracture with suture anchors, which subsequently failed.
The decision was then made to proceed with operative intervention as described above. The patient was kept overnight for observation and pain control and was then discharged home the following day. The patient was made weight-bearing as tolerated with limited active hamstrings contraction, as well as no running, jogging, or strenuous exercise to the pelvis.
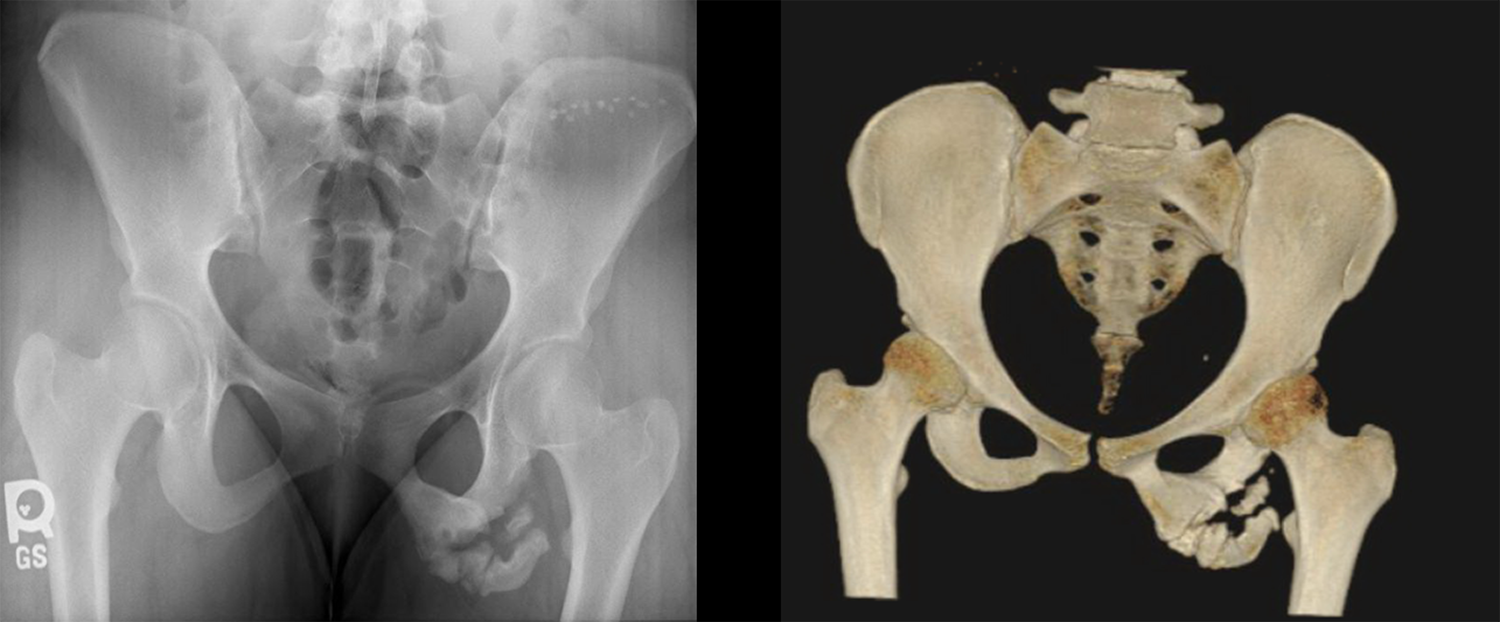
Case 2 preoperative images. Anteroposterior radiograph and three-dimensional reconstruction computed tomography scan of pelvis of a 17-year-old girl demonstrating a left ischial tuberosity nonunion.
The decision was made to proceed with operative intervention as detailed above. She was discharged home the day of surgery and was made toe-touch weight-bearing for 6 weeks with the use of crutches.
Results
Case 1
The 16-year-old boy had an uneventful immediate postoperative course. His wound healed without complications, and he was compliant with his postoperative restrictions. At the 6-week visit, the patient was walking without a limp and had no pain. He had minimal tenderness to palpation along the ischial tuberosity. Radiographs demonstrated stable alignment of the ischial tuberosity with callus formation and healing across the nonunion site (Figure 6). By the 12-week visit, the patient had returned to light jogging and everyday activities without pain. He did demonstrate mild hamstrings weakness as compared with the contralateral extremity. Radiographs showed interval callus formation and stable alignment of the nonunion site. At his 6-month visit, the patient had returned to light jogging and running. On exam, he was able to perform a one-leg hop and full double squat without pain. Radiographs at that time showed a completely healed ischial tuberosity nonunion. The patient returned to the clinic at the 15-month mark complaining of hamstring pain during deep squats that was relieved with anti-inflammatory medications. He had returned to competitive basketball and extensive weight training. On exam, the patient had no weakness or pain with internal/external rotation, abduction, and flexion of the hip. He was mildly tender to palpation along the hamstring tendon, without tenderness at the ischial tuberosity. Overall, he was very happy with his progress and wanted to ensure he did not reinjure his nonunion site. Radiographs demonstrated a healed ischial tuberosity with stable screw fixation (Figure 6).
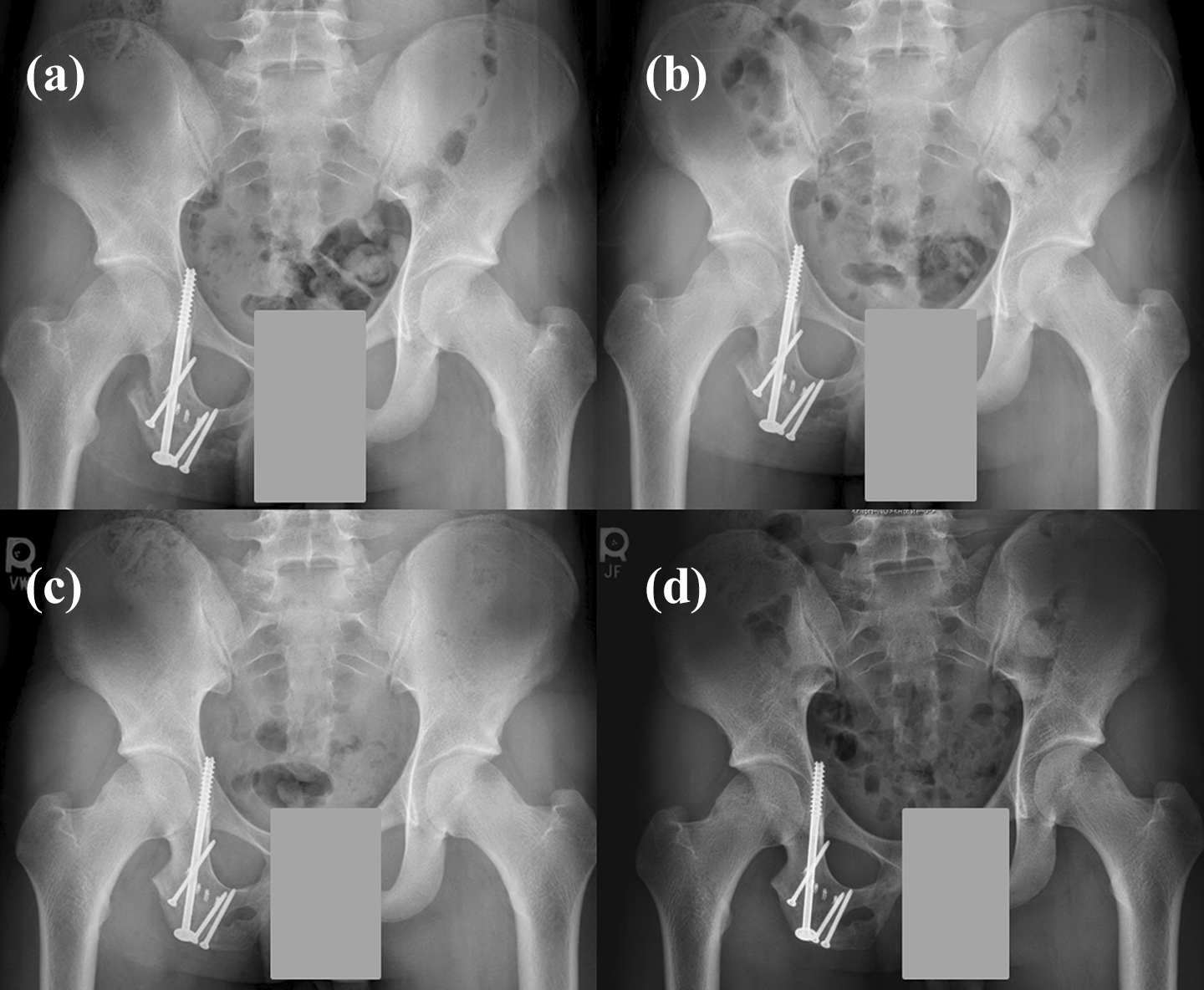
Case 1 follow-up radiographs. Anteroposterior pelvis at (a) 6-week and (b) 3-month follow-up visits demonstrating intact screw fixation with bridging callus formation at the nonunion site. (c) The 6-month and (d) 15-month radiographs demonstrating a healed nonunion site.
Case 2
The 17-year-old girl also had an uneventful postoperative course. Her incision healed without any complications, and she was compliant with her weight-bearing restrictions. At the 6-week visit, the patient reported no pain and had full, painless range of motion of the left lower extremity. She had no pain with resistance to hamstrings activation. Radiographs demonstrated bridging callus formation at the nonunion site. At this visit, she was progressed to weight-bearing as tolerated. She returned again at 12 weeks, at which time radiographs demonstrated interval callus formation at the nonunion site. She continued to have no pain with ambulation or range of motion of the hip. She was then allowed to return to full activities at 3 months. By 6 months, the patient had returned to cheerleading without pain and was pleased with her progress. She had no hamstrings strength deficit as compared with her contralateral side and had full non-tender range of motion about her hip. Radiographs demonstrated a stable nonunion site with continued bridging callus formation medially and laterally at the nonunion site without signs of hardware complications (Figure 7). The patient cancelled her 12-month appointment, as she was having no pain and had returned to everyday and athletic activities. However, since full healing was not appreciated on follow-up radiographs, this nonunion site may become symptomatic in the future.

Case 2 follow-up radiographs. Anteroposterior pelvis at (a) 6-week and (b) 3-month follow-up visits demonstrating intact screw fixation with bridging callus formation at the nonunion site. (c) The 6-month radiograph demonstrating a stable nonunion site.
Discussion
The main finding from this case series was that an innovative approach to ischial tuberosity nonunions via a posterior column screw can provide excellent outcomes and radiographic healing of the nonunion site in the adolescent population without screw pullout or loosening.
There is no consensus within the literature regarding an appropriate surgical technique for ischial tuberosity nonunions. A recent retrospective study reported good functional outcomes in chronic avulsion fractures treated with open fixation with a plate and screws and autogenous bone grafting via a Kocher-Langenbeck approach. Bone grafting was obtained from the greater trochanter or posterior iliac crest for all but one patient. 2 This approach, however, is extensile and can be morbid for young athletes wanting to return to pre-injury sporting levels. One case report detailed fixation of nonunion with three partially cannulated screws across the fracture site, which provided temporary relief. However, by 6 months one screw had loosened, causing the patient discomfort during activity; all three screws were removed after 1 year due to persistent pain. 7
This case series utilized a muscle-sparing approach to the nonunion site through a cosmetically appealing incision and introduced a novel approach to nonunion fixation without the use of bone graft. The large 6.5-mm ASNIS screw placed in the posterior column allowed for adequate compression across the nonunion site, while the 3.5-mm cortical screws provided additional stability to the site with minimal risk of loss of fixation. Both patients returned to pre-injury activity with no reported pain or hamstrings weakness 6 months after surgery. Radiographs demonstrated a healed or stable nonunion site by 6 months without screw loosening or pullout. This approach provides treating surgeons a viable option for treating symptomatic ischial tuberosity nonunions through a muscle-sparing approach with minimal complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.