
Abstract
BACKGROUND:
Relatively little is known about the longitudinal changes in strength and function in the early phase compared to long term outcome following reconstruction of the anterior cruciate ligament (ACL).
OBJECTIVE:
To assess the isokinetic concentric strength of the knee extensors and flexors as well as the distance jumped in the one-legged hop test in patients before and at 3, 6 and 12 months after (6 and 12 months for the hop test) reconstruction of the ACL.
METHOD:
Seventy-three men, aged 18–50 years took part in the study. The primary outcome measures were the International Knee Documentation Committee (IKDC) scores at 3, 6, and 12 months after surgery and one-legged hop test at 6 and 12 months after post-reconstruction.
RESULTS:
There was a consistent increase in muscular strength between 3 and 12 months post-reconstruction. Fair but significant correlations were found between the IKDC score at 12 months and the peak moment of the knee extensors at 3 and 6 months (
CONCLUSION:
Knee extension strengthening in early phase is crucial to restoring sporting performance after ACL reconstruction.
Introduction
Anterior cruciate ligament (ACL) injury, which compromises knee functionality and may trigger knee osteoarthritis (OA) as a long-term complication, has become one of the most common knee injuries in recent years as more subjects engage in sporting activities [1]. The reported OA rates 10–20 years after ACL injury vary from 10% to 90% [2]. Most patients with ACL injuries are younger than 30 years of age; such injuries are thus responsible for early-onset OA (between the ages of 30 and 50 years) associated with pain, functional limitations, and a reduced quality of life [3]. Many patients appear to be minimally impaired but some cannot return to sporting activities after ACL reconstruction. A recent meta-analysis found that, on average, 63% of patients returned to their previous level of sporting activity after ACL reconstruction [4]. Significant correlations between quadriceps and hamstring strengths, and a successful return to functional activities, have been reported [5]. Progressive rehabilitation emphasizing strengthening of the quadriceps and hamstring to levels close to those of the non-operated leg enhances the likelihood that the patient may successfully return to the pre-surgery performance level [5].
Good functional performance after operation is important in terms of patient satisfaction. Many studies have explored patient performance after ACL reconstruction. The International Knee Documentation Committee (IKDC) score, which is a self-reported measure, has good reliability, validity, and patient relevance [6]. The hop test has served as a practical, performance-based outcome measure; equipment requirements are minimal and the test is rapid. The results reflect the extent of integration of neuromuscular control, lower limb strength, and patient confidence in the lower limb [7, 8]. Muscle strength plays an important role in knee joint function and stability. Knee strength is of great interest after knee injury; this measure reflects functional status and predicts whether a patient may return to the previous level of activity [9]. However, potential confounding factors (i.e., gender, age, and/or body mass index) may be in play; these are patient-specific (i.e., not associated with the operated leg). Comparisons of muscle strength within the operated leg (the hamstring-to-quadriceps [H: Q] ratio), and between the operated and non-operated legs (the limb symmetry index [LSI]) can be used to reduce any influence of possible confounders [10]. The LSI is most frequently used to determine if strength and hop performance are normal or abnormal [11].
If ACL rehabilitation is to be successful, it is important to measure changes in functional parameters early after surgery. However, little information is available on longitudinal changes in knee strength, knee score, or dynamic stability from a time soon after reconstruction to 1 year later. Currently, the two most common autograft options are hamstring tendons (the semitendinosus and gracilis) (HTG) and the patellar tendon (bone-patellar tendon-bone) (BPB). Many previous studies that compared these two types of graft found no significant differences in terms of overall outcome, but reported modest differences in in-situ characteristics and donor site morbidity [12, 13, 14, 15]. In particular, it remains unclear whether these characteristics differ in BPB and HTG patients soon after operation.
The aims of this study were therefore to investigate the change in knee strength and function by graft type after ACL reconstruction, using a retrospective cohort sample, and attempt to identify factors predicting the attainment of normal performance.
Methods
Subjects
Patients who underwent arthroscopic ACL reconstruction with autograft (BPB vs HTG) between April 2007 and August 2013 were considered for inclusion. This was a retrospective, cohort observational study, using the clinical rehabilitation pathway applied after arthroscopic ACL reconstruction by the Seoul National University Bundang Hospital. The exclusion criteria were bilateral knee injury, prior knee surgery, infection of the affected knee, any severe medical illness, and/or neuropathy or arthritis of the affected knee. A total of 110 patients underwent rehabilitation. Overall, 26 patients were excluded, 4 refused to submit to testing (1 at 3 months, 3 at 12 months), 1 developed a contralateral leg injury, rehabilitation was delayed in 3 because of knee pain, and 8 were lost to follow-up. Hence, 73 of the 85 patients completed the 1-year follow-up (Fig. 1). The institutional review board (IRB) of Seoul National University Bundang Hospital approved the study (B-1402-238-109). Written informed consent was obtained from all patients and confirmed by the IRB.
Muscle strength
Isokinetic muscle strength was measured using a Biodex System 3 isokinetic dynamometer (Biodex Medical Systems, Shirley, New York, USA). Testing was performed before operation, and at 3, 6, and 12 months after operation and at a velocity of 60
Progress of patients through the study.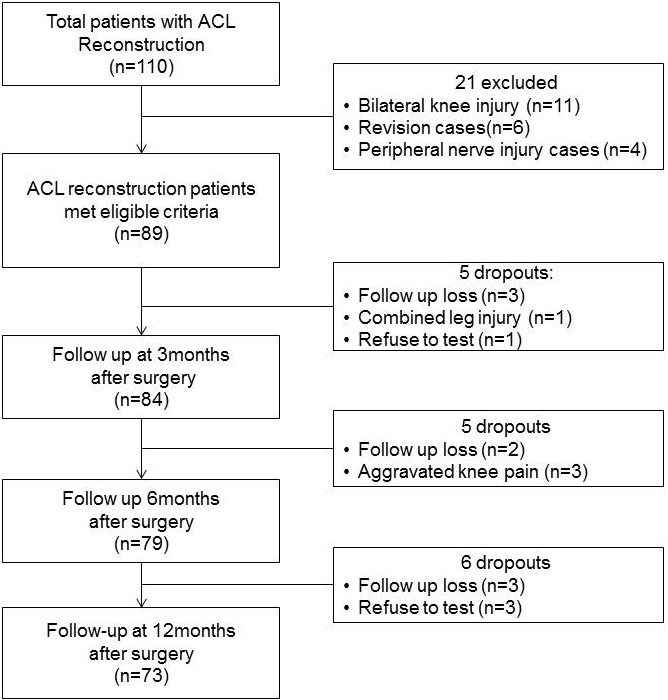
Knee joint function was assessed using the International Knee Documentation Committee (IKDC) scoring system, which is a well-validated instrument used to assess knee ligament injuries [16]. The IKDC form has 18 items (7 on symptoms, 1 on participation in sports, 9 on daily activities, and 1 on current knee function). The response options vary. Item 6 dichotomizes responses into yes/no. Items 1, 4, 5, 7, 8, and 9 employ 5-point Likert scales. Items 2, 3, and 10 use 11-point numerical rating scales [16]. All patients self-rated their performance using an electronic version of the IKDC form available in our medical records system. Primary outcomes were documented using the IKDC scores obtained 3, 6, and 12 months after surgery.
Functional performance was measured using the one-legged hop test, which was performed three times for each leg; the longest hop distance was recorded. The test was performed 6 and 12 months after ACL reconstruction. Each subject was asked to stand on one leg with both hands behind the back, and was instructed to jump as far as possible and land on the same foot. Both hands were to remain behind the back during both jumping and landing. The hop distance was measured from the starting position of the toes to that of the heel after landing [17]. All subjects jumped using the non-injured leg first, followed by the injured leg, during both practice and tests. All tests were supervised by the same physical therapist. Verbal encouragement was given and footwear was standardized. Each subject first performed three to five practice trials, followed by a maximum of three test trials. However, if hop performance increased from hop 1 to hop 3, additional hops were allowed until no further increase was evident.
Post-operative rehabilitation protocol
All subjects underwent four-step clinical rehabilitation; each step features particular exercises and sets goals for range of motion, muscle function, and functional performance. Time intervals for each level were suggested but goal attainment was prioritized. Non-steroidal anti-inflammatory drugs were allowed if needed. In the protection phase (0
Data analysis
The main outcome measure was the isokinetic PM. Limb symmetry index (LSI (%)
Basic characteristics of the study participants (
73)
Basic characteristics of the study participants (
Longitudinal changes in performance
LSI: Limb Symmetry Index, % of non-injured side, H/Q ratio: peak moment of knee flexor/knee extensor, IKDC: The International Knee Documentation Committee.
Predictive value of initial strength parameters of successful outcome in terms of IKDC score and hop distance at 12 months with measurements taken at 3 months after operation, calculated using multiple logistic regression analysis
Data were obtained from male participants after adjusting for age, graft types and the presence of a combined meniscus tear. LSI: Limb Symmetry Index, % of non-injured side, H/Q ratio: peak moment of knee flexor/knee extensor.
Longitudinal changes in the PM of the knee extensor (left) , knee flexor (right).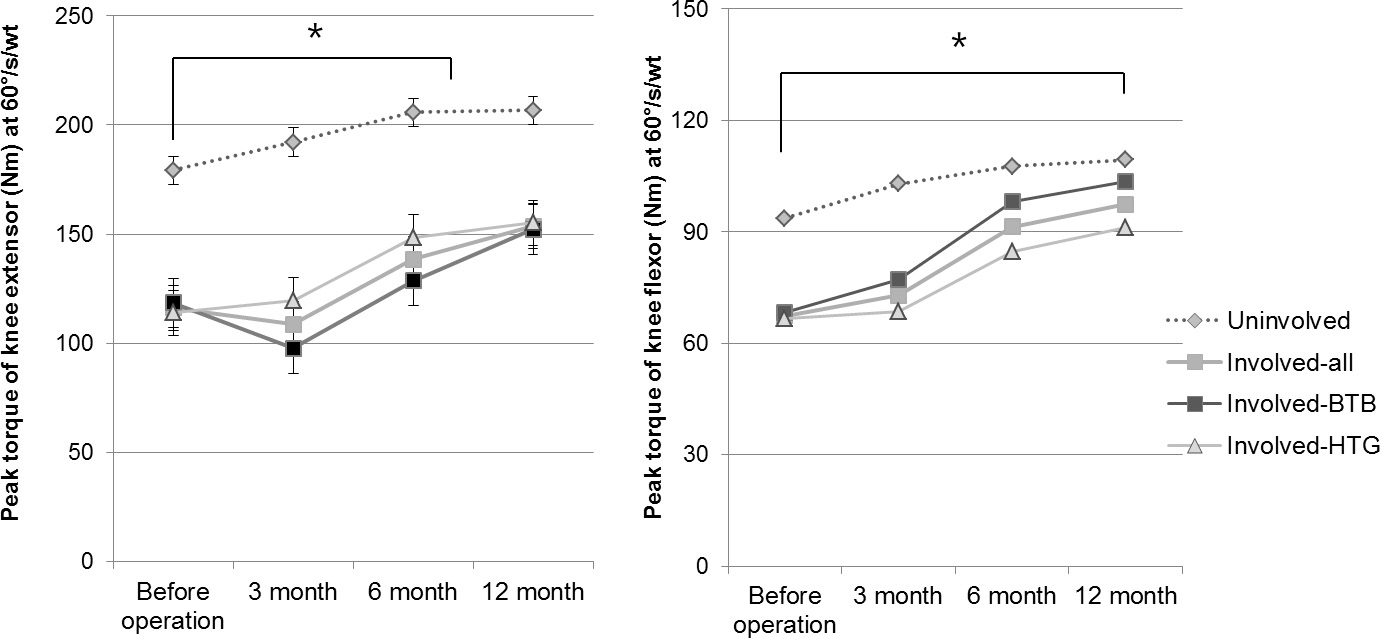
Comparison of the IKDC scores of the patellar and hamstring tendon graft groups. The hamstring tendon graft group scored higher on item 5 (the highest level of activity possible without significant swelling), item 7 (the highest level of activity possible without any significant “giving way”), item 9a (difficulty associated with climbing stairs); item 9g (difficulty associated with running in a straight line), item 9h (difficulty associated with jumping and landing on the operated leg), and item 9i (difficulty in stopping and starting quickly).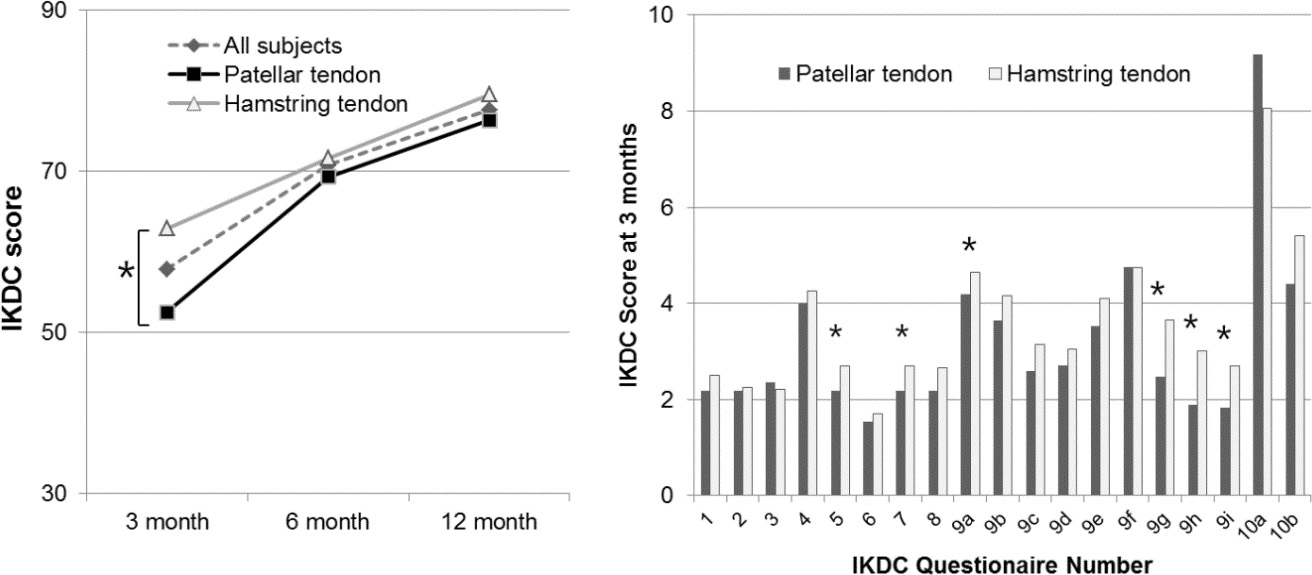
A total of 73 male patients, the average age was 30.7 years and the average height 172.9 cm. Among them, 34 patients received BPBs and 37 received HTGs. Over the half (60.3%) of all patients had additional lesions including medial meniscus (Table 1). Neither age nor BMI differed significantly between the groups. All injured ACLs were reconstructed via arthroscopic surgery.
Knee strength was greater at 12 months than before the operation not only on the involved side but also on the uninvolved side (Fig. 2). Overall, the IKDC score, and hop distance, tended to improve from 3 to 12 months after operation (Table 2). Knee extensor strength was somewhat lower in the BPB group than the other group at both 3 and 6 months, but statistical significance was not attained. Knee flexor strength was somewhat higher in the BPB than the HTG group, but statistical significance was not attained (Fig. 2).
The HTG group had a significantly higher IKDC score than the BPB group at 3 months, but there were no significant differences between the two groups at 6 or 12 months after operation (Fig. 3). We evaluated all individual IKDC items recorded at 3 months to seek an explanation to the differences in IKDC scores. The HTG group scored significantly higher on IKDC items 5, 7, 9a, 9g, 9h, and 9i at 3 months (Fig. 3). The HTG group was able to tolerate a higher level of activity without significant swelling (item 5, 2.7 vs. 2.18, HTG vs. BPB); could undertake a higher level of activity without any significant “giving way” (item 7, 2.7 vs. 2.18 HTG vs. BPB); found it less difficult to climb stairs (item 9a, 4.65 vs. 4.18, HTG vs. BPB); and had less difficulty running in a straight line (item 9g, 3.65 vs. 2.65, HTG vs. BPB), jumping and landing on the involved leg (item 9h, 3.00 vs. 1.88, HTG vs. BPB), and stopping and starting quickly (item 9i, 2.70 vs. 1.82 HTG vs. BPB). There were no significant differences between the groups in terms of the highest level of activity possible without significant knee pain (item 1); the frequency and severity of pain (items 2 and 3); the extent of knee swelling, stiffness, knee locking, or knee catching (items 4 and 6); or the difficulty in going down stairs, kneeling, squatting, sitting with the knee bent, or rising from a chair (items 9b, 9c, 9d, 9e, and 9f).
We found significant correlations between measures of knee strength (knee flexion at 3 months, knee extension at 6 months) and the IKDC score at 12 months. (
Discussion
The main finding of this longitudinal study is at 1 year following ACL reconstruction all parameters including strength, IKDC score, and hop distance improved, compared to the baseline at 3 months post-op. In addition, knee extensor strengths at 3 months post-op was a significant factor for the successful outcome based on the functional performance at 12 months of follow-up adjusting for confounding variables, which indicates that improved knee extensor strength early in rehabilitation significantly influenced the successful outcome of rehabilitation. Lee et al. [20] reported that patients who could return to sporting activities after ACL reconstruction had higher IKDC scores at 5 years. Eitzen et al. [21] found that early exercise (within 3 months after injury) significantly improved knee function. Our results are similar but, to the best of our knowledge, this is a rare trial to longitudinally measure knee strength and performance (including individual IKDC items) from soon after ACLR, and to correlate such data with the extent of operative success.
The goal of ACL reconstruction is to improve patient functionality, allowing a return to an active lifestyle with minimal disability, and to protect the knee from further injury [22]. It is essential to accurately measure knee position and detect joint motion when a knee has become unstable after ligament injury [14]. Restoration of knee strength is also important after ACL injury; this allows a safe return to physical activity and prevents the development of knee OA [10, 23]. Strength deficits are associated with lower Lysholm knee scores and abnormal one-leg hop test results within 1-year of follow-up; these negative findings are predictive of radiographic OA developing over 10 years in patients who undergo ACL reconstruction [24, 25]. In our study, knee extensor strength was positively correlated with hop distance; extensor strength was more important than flexor strength in this context. The mean quadriceps strength was 59% that of the uninjured knee 6 months after operation, improving to 85% at 2 years [26]. Quadriceps atrophy associated with intra-articular knee surgery may also reduce muscle strength, creating a vicious cycle of a reduction in strength, knee pain, and further quadriceps atrophy [27]. These results suggest that knee strength during the early phase of rehabilitation influences not only symptoms and functional status but also the success rate of rehabilitation. Palmieri-Smith and Lepley [28] reported that only
Recovery of knee strength differed among patients receiving different types of graft. The BPB group had a lower level of activity (as reported in the IKDC questionnaire); patients found it more difficult to “give way” and to jump and land on the affected leg during the very early stage of rehabilitation, compared to the HTG group. The BPB group had a lower knee extensor strength than did the HTG group, emphasizing the importance of knee extensor strength. Knee flexor strength was lower in the HTG group than in the other group. In addition, a significant correlation was evident between knee flexor strength 3 months after operation and the IKDC score 12 months after operation, indicating that knee flexor strength was also important in the early phase of rehabilitation, particularly in the HTG group. Thus in early phase of rehabilitation for HTG groups, knee flexion exercise is emphasized either by closed kinetic exercise or other leg assisted exercise in our protocol and other reviews [30].
As for the HQ ratio, it was suggested by Lentz et al. [32] that it was not a significant predictive factor for post-op success. In the current study this ratio proved to be significantly correlated with both the IKDC score and hop distance; a higher ratio was associated with a lower IKDC score and a reduced distance. However, this was not the case for the early phase after adjusting for confounding variables. The HQ ratio was higher among BPB patients compared to their HTG counterparts both at 3 and 6 months post-op. The reason is that the quadriceps was relatively weak in the BPB group and the hamstring was weak in the HTG group. Similar findings have been reported elsewhere; in previous studies, isokinetic knee flexion strength remained weak in HTG groups, and knee extensor strength was poor in BPB groups, at 6–36 months after reconstruction [10, 33]. A patellar graft compromises both knee extension and patellar movement [34]. The hamstring procedure was associated with a strength deficit of the knee flexors, caused by posterior knee pain [35]. The biceps femoris muscle cannot compensate for the deficit in knee flexion strength. Such different effects on functional recovery over time should be considered when rehabilitation strategies are planned soon after ACLR. Thus, rehabilitation focusing on particular strengthening exercises appropriate for each graft type, soon after reconstruction, is important to ensure a successful functional outcome. For example, in case of hamstring graft, CKC based exercise for knee flexors is also emphasized with combined quadriceps strengthening. It could be argued what the best modality is to restore muscle strength following ACL reconstruction surgery. The Elmquivst’s protocol [36] is based on 8 weeks of protection during early post-op period and while suggesting that isokinetic training did not offer any specific advantage in the early muscular rehabilitation of this operation. Other alternatives such as neuromuscular electrical stimulation have been considered when progressive resistance training is difficult to be applied [37].
A limitation of our study was that the work was retrospective and observational in nature; therefore, graft choice was not controlled. In addition, we did not include eccentric strength in the isokinetic test. Originally, this trial was designed with the retrospective cohort study based on clinical pathway from pre-rehabilitation and post-operative rehabilitation after ACL reconstruction. Therefore, we decided to focus only on concentric testing considering the burden on clinical observational procedure. Population bias and confounding factors such as gender, age, and BMI may have been in play. We evaluated the relative values of leg HQ ratios and compared the involved and uninvolved legs (by calculating LSI values). Further prospective studies are needed; such work should evaluate the long-term effects of rehabilitation, focusing on exercises that strengthen the knee joint soon after ACL reconstruction.
Conclusion
Patients in whom knee extensor strength had recovered well 3 months after ACL reconstruction exhibited better dynamic performance at the 1-year follow-up. Therefore, strengthening exercises of knee extensor beginning soon after reconstruction should be prescribed; this is a crucial aspect of rehabilitation to restore normal performance after ACL reconstruction.
Conflict of interest
The authors declare no conflict of interest.