
Abstract
BACKGROUND:
“When will I be able to play again?” is the most frequent question asked by injured athletes. Due to the complex nature of sports injury, deciding when an injured athlete may safely return to training is a critical and difficult decision.
OBJECTIVE:
To study if the Safe Multidimensional Algorithm for Return to Training (SMART) scores, applied before the release to full return to training after injury differs between football players who suffer a subsequent re-injury and football players who do not.
METHOD:
Seventy one male professional football players were prospectively monitored for injuries during two seasons. The SMART tool was applied in injured players with an absence
RESULTS:
Fifty-five injuries with absence
CONCLUSIONS:
A multidimensional approach of Return to Training that includes objective measures may indicate potential deficiencies in the recovery of injured players.
Introduction
Injuries are particularly common in high-impact pivoting and contact sports such as professional football [1]. In addition there is evidence to show the close relationship between injury and decreased team performance [2, 3].
Once an injury occurs the most frequent question which the athlete and the coach ask is “When will I/he/she be able to play again?”. Due to the complex nature of sports injury [4], this question is usually very difficult to answer in the early setting. Moreover, causes of injury and re-injury are multi-factorial in their nature [5] and there is therefore a clear consensus about the need to address the recovery process of an injured athlete in an individualised manner [6, 7]. However, deciding when an injured athlete may safely return to training is a critical and difficult decision [7, 8], for which the guidelines still have not been clearly specified [9, 10].
A multidimensional approach to return to training was proposed for acute hamstring injuries already in 2010 [11]. More recently, an expert group pointed out the importance of including several measurements on the injured athlete before return to training after hamstring injury [12]. Five main criteria domains were highlighted: functional performance, strength, flexibility, pain and player’s confidence. Moreover, in order to determine how and when to advance an injured athlete through rehabilitation, the approach should include reliable, objective and quantifiable (clinical and functional) criteria [11].
The Safe Multidimensional Algorithm for Return to Training (SMART) is a tool which observes the athlete in an individualised way and permits the parties responsible for the rehabilitation process to objectively assess the progression during rehabilitation from injury. This tool assesses the anatomical, functional and psychological predisposition of the player to return to team training sessions [10, 13, 14]. At the same time, it is intended to increase the athlete’s motivation and involvement through clear and concise specification of the objectives to be achieved in each recovery phase [15].
The objective of this pilot study was to evaluate if the SMART scores differ between football players who suffer a subsequent re-injury and those who do not. The hypothesis was that players who sustained a re-injury, would present worse results before the clearance to return to training compared with those who did not.
Method
Participants
A total of 71 male football players, members of the Albacete FC, Spain took part in this study which was carried out during the 2012/13 and 2013/14 seasons. The first team (
Definitions
An injury was defined according to the consensus statement for football injury surveillance as any complaint sustained by a player that results from a football match or training, irrespective of the time loss from football activities [16]. An early recurrence was defined as an injury of the same type and at the same site as the index injury within 2 months of a player’s return to full participation.
Safe Multidimensional Algorithm for Return to Training
SMART is an assessment tool composed of a series of progressive steps which the injured athlete must pass without pain, defined as lower than 2/10 during activity rated on a visual analogue scale (VAS), prior to being released to return to training with the team. Based on the overall decision model [7, 17] and also inspired by other preliminary approaches [10, 11, 18], the SMART tool consists of 17 different measurements of a medical, psychological, functional and sports-specific modality, distributed by the complexity level into three “steps” to complete. We based the selection of the test to be included on 4 criteria psychometric properties of the test, expert opinion, recommendations from the literature and the adaptability to a context with minimal financial resources. Using the Delphi technique, a total of 16 experts (competence coefficient acceptable-high: 0.84 K) chose the test that best fit the needs of a football player in recovery process [19, 20].
Levels of achievement for SMART measurements
Levels of achievement for SMART measurements
POMS, Profile of Mood States; SMART, Safe Multidimensional Algorithm for Return to Training.
The different steps in the Safe Multidimensional Algorithm for Return to Training (SMART).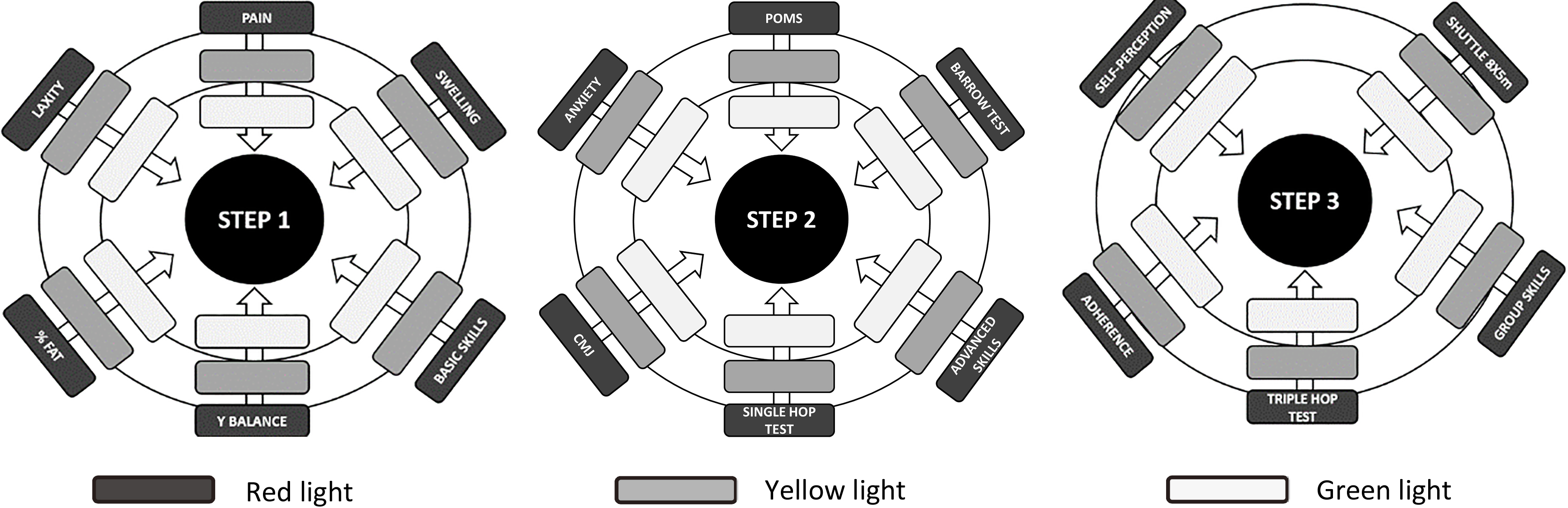
The injured football player must pass all the tests included in each step to be able to move on to the next step. Once Step 3 is completed, the player can fully return to training without restrictions (Fig. 1). Due to the time required to carry out all the included tests (5–7 days) the SMART tool was only applied in players who suffered injuries with an absence period
For each test, a three level traffic light system (green light
Between-group comparisons in anthropometry, absence and prior experience
The tests or assessments selected for
The tests or assessments selected for
The tests or assessments selected for
Procedure
With the objective to obtain functional reference values for each individual in a non-injured state, all the injury-free players carried out the functional tests included in the SMART tool at three different times of the season as a matter of routine (August, December and June). When an injured player was in his expected final days of recovery, he had to carry out all of the tests included in the SMART tool once again.
The persons responsible for the application, control and recording of the tests were a physician, a physiotherapist and two PhD candidates in sports sciences, all of whom worked with the first team of the Albacete FC with extensive knowledge about the tests to be performed. Except for the measurements with a more clinical nature such as laxity, swelling and adherence which were under the responsibility of the medical staff, the rest of the tests were supervised by the team’s physical trainer or injury rehabilitation therapist. In the absence of a sports psychologist in the club’s structure, the questionnaires which assessed dimensions such as anxiety, mood state, self-perception and adherence were also applied by the team’s physical trainer.
Data analysis
The IBM SPSS Statistics v.22 software was used for all analyses. Data on anthropometry and length of absence was reported as mean with corresponding standard deviation (SD). We used the Kolmogorov-Smirnov test to determine if data were normally distributed. We applied Student’s t-test in the variables with a normal distribution and the Mann-Whitney U test in those with non-normal distribution. We calculated effect sizes (ES) to determine the magnitude of the differences [33], and classified as follows: trivial (
Results
A total of 165 injuries were recorded in 62 players during the study period; 55 injuries in 29 players had an absence period of
Between-group comparisons of average variables in the SMART tool
Between-group comparisons of average variables in the SMART tool
CMJ, Counter Movement Jump; POMS, Profile of Mood States; SMART, Safe Multidimensional Algorithm for Return to Training.
Between-group comparisons of binary categorised variables in the SMART tool
CMJ, Counter Movement Jump; POMS, Profile of Mood States; SMART, Safe Multidimensional Algorithm for Return to Training.
The group of players with re-injury presented worse values for: fat percentage, basic skills and pain variables in Step 1. Barrow test, advanced skills, anxiety state, POMS stress and POMS depression in Step 2 and shuttle 8
SMART cut-off scores and re-injury risk
Players who had an anxiety greater than 17 points (RR 8.63, 95% CI 2.0 to 36.2), presented a POMS tension greater than 4 (RR 9.5, 95% CI 1.8 to 49.1) or POMS depression greater than 2 (RR 10.3, 95% CI 2.0 to 36.2) had a significantly higher re-injury rate. Similarly, players with worse values on the Barrow test (RR 21.0, 95% CI 2.0 to 213.2), shuttle run 8
Discussion
The main aim of this pilot study was to find out if the Safe Multidimensional Algorithm for Return to Training (SMART) scores differed between football players who suffered a subsequent re-injury and those who did not. The key finding show that players who sustained a re-injury, presented worse SMART scores (pain, agility, sport specific skills, anxiety, depression, and self-perception) before the clearance to return to training compared with those who did not.
Considering the multiple and complex variables which influence the return to play decision, multidimensional approaches are needed to objectify and facilitate the progression of the injured player. In 2007, the Biopsychosocial Model [35] appeared as one of the first multidimensional approach for the injuries recovery. This proposal, as SMART intends, integrates biological, psychological and social assessments. Subsequently, in the year 2015, the StaRRT Model [17] appears as an updated version of the Global Decision-Based Model of Creighton et al. [7]. The main innovation that includes this three-step multidimensional approach (StaRRT) is that it helps estimate the risk of different short-term and long-term outcomes associated with RTT (Return to Training). Since each moment of recovery presents functional, physical and psychological particularities, this idea has also been included in the SMART algorithm.
In this way, following the recommendations identified at the First World Congress in Sports Physical Therapy [8], SMART tries to quantify the progress and predisposition of an injured player through a multidimensional approach. The effectiveness of these multidimensional approaches versus more traditional and simplistic approaches has recently been tested in other contexts. In a recent study [36], football players with acute hamstring strain injury who underwent an individualized multidimensional and criteria-based algorithm from the early stages of the process markedly decreased the risk or re-injury compared to a general protocol where lengthening strength training exercises were prioritized. This multidimensional approach, based on our results, should focus on variables related to pain, agility, sport specific skills, anxiety, depression and self-perception since these were the variables that showed the strongest association with risk of re-injury.
Pain at RTT increase re-injury risk
In this study, the results obtained corroborate the importance some variables may have in avoiding re-injury after RTT. For example, some authors had pointed out that perceived pain could condition the occurrence of a re-injury after ACL injury [37]. Although focused on all types of injuries and not only ACL, this would be supported by our data since those players with a perceived pain greater than 2 (out of 10) presented an increased risk of re-injury.
Agility and sport-specific skills associate with re-injury risk at RTT
In relation to the importance of properly recovering the skills for cutting manoeuvers and fast accelerations, in the same line as other studies [38], we found that a worsening of more than 10% in the execution time of the Shuttle 8
Psychological factors matter in RTT
In reference to the psychological variables as part of the player’s well-being and their importance in the RTT [8, 14], we found that the anxiety state, POMS-depression and self-perception readiness were the most sensitive manifestations for differentiating between football players with and without recurrent injury. These results are in accordance with another previous study showing that psychological readiness is a dynamic and psychological process that seems to be composed of three dimensions: confidence, realistic expectations and motivation [39].
Other
With regard to other tested parameters and in spite of the existence of studies with satisfactory results in relation to the % fat [40], POMS [41], posture control [42], adherence [43], and the vertical jumps (bipodal and unipodal) [44], we did not detect differences for these variables in the presence or absence of re-injury.
Improving SMART
In the case of relying on a professional environment with greater resources, as is the case of the large European football clubs which compete in the UEFA Champions League, several measurements of interest could be considered too, such as: tensiomyography for muscle stiffness, isokinetic test for strength, global position system (GPS) for profile efforts, etc. Although most of these techniques have not yet demonstrated their usefulness to ensure optimum RTT, we believe that they could provide very interesting objective and complementary information.
The analysis of the association between the tests included in SMART and the risk of re-injury, will allow us to propose improved versions of this algorithm in the future. For example, if we know that there are certain tests that are more related to an optimal RTT than others, we may improve versions of this algorithm including only these tests. The data obtained when comparing the risk of re-injury must be considered as relevant starting points on which major emphasis can be placed when making a decision about a RTT and hence in future research, construct improved versions of the algorithm presented here.
We hope that this study may encourage critical evaluation of the algorithm, and lead to the development of more objective, reliable and quantitative measures including a multi-factorial approach to rehabilitating football injuries.
Study limitations
Due to the sample limitations which this research presented and SMART has not yet been validated, the data also cannot be generalized. More studies in this line of research are required with larger samples, using a similar multidimensional methodology in several teams at the same time and thus increase the external validity. Another limitation in our study is that the achievement ranges for each of the tests were established in a generic way, without taking into account the type or the severity of the injury. We suggest that this be adjusted according to these two variables in future versions of SMART. Finally, as Creighton et al. [7] suggest, it would be interesting to test the effect of the pressure from the environment (coach, fans, family or the competition calendar) on the return to the training sessions of the injured player. This question has been vaguely taken into account in our proposal since only 1 of 10 questions in the self-perception questionnaire was related to the pressure of the environment. We are aware of the difficulty of assessing this issue but, due to its contextual importance, researchers are encouraged to consider these factors in future studies.
Conclusions
The SMART algorithm is presented as a feasible tool when making a decision regarding RTT for an injured football player but further validation is necessary, preferably a multidimensional approach to rehabilitation. Preliminary findings from this study show that players who sustained a re-injury presented worse SMART scores (pain, agility, sport specific skills, anxiety, depression, and self-perception) before the clearance to return to training compared with those who did not sustain a re-injury. A next step would be to evaluate whether the use of SMART with strict adherence to progression criteria could be applicable in guiding a successful RTT with a reduced risk or re-injury.
Footnotes
Acknowledgments
The authors would like to thanks to Albacete football Club and all their players for their willingness and essential collaboration in this project.
Conflict of interest
None declared.