
Abstract
Background:
The first case series to report on return to play (RTP) in National Football League (NFL) players after primary anterior cruciate ligament (ACL) reconstruction (ACLR) published an RTP rate of 63%. Other studies that have attempted to estimate RTP after ACLR in these elite athletes have been largely based on secondary sources. This study is the second to report the authors’ own results in treating ACL injuries in NFL players spanning a study period of 25+ years.
Purpose:
To report the senior authors’ experience treating ACL injuries in NFL players as well as revisit the concept of RTP as it is currently used to measure successful surgical outcomes in professional athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 47 NFL players were treated at our institution for knee injuries that included a complete tear of the ACL; of these, 41 were primary ACLR and 6 were revision ACLR. Of the primary ACLRs, 6 were classified as ACL plus additional ligament and 3 were classified as multiligament. Return to game play (RTGP) was defined as returning to play in a regular-season game. Successful return to previous participation (RTPP) was defined as return to a level of participation equal to the level the player had reached before injury. Multivariate analysis was used to assess predictors of successful RTPP.
Results:
Using the RTGP criteria proposed by prior authors, the RTGP after primary ACLR was 73%. Using our proposed RTPP criteria, 87.8% of players successfully returned to the same level of participation after primary ACLR. RTGP percentage for all NFL players after ACLR (including multiligament injuries) was 67.6%, and the overall RTPP for those patients was 87.8%. In multivariate analysis, age ≤25 years was predictive of successful RTPP. High draft picks and offensive players played more seasons after primary ACLR. ACL graft rupture occurred in 4.3% of this cohort. Contralateral ACL tear occurred in 8.5%.
Conclusion:
Regardless of which definition is used to measure a successful outcome after ACLR surgery, the findings of this study suggest that successful return after primary ACLR in NFL athletes is higher than previously reported. While concomitant reconstruction of a single collateral ligament did not affect RTPP, revision ACLR or bicruciate plus collateral ligament reconstruction was associated with a lower RTPP rate. Age ≤25 years predicted successful RTPP. The risk of a future ACL tear of either knee after index reconstruction was approximately 13%.
Return to football after anterior cruciate ligament (ACL) reconstruction (ACLR) has been estimated to be between 63% and 69% for high school and college athletes, respectively. 5 Several studies 1,3,6 –8 have reported on return to play (RTP) after ACLR in the National Football League (NFL). For all of these studies, the outcome of RTP was used as a measure of a successful outcome after ACLR surgery. The first study 8 to report RTP in the NFL after ACLR did so on a consecutive series of 49 NFL athletes who underwent primary ACLR with a single surgeon at a single institution. In that study, successful RTP was specifically defined as participation in an NFL game subsequent to reconstruction and was achieved by 63% of athletes in their cohort. Since that publication, other studies 1,3,6 –8 have used the concept of RTP as a measure of successful ACLR in the NFL.
Since the initial publication by Shah et al, 8 which reported results from NFL players treated at their institution, all subsequent studies 1 –3,6,7 that have published on RTP after ACLR in NFL athletes have mined public online databases to identify players who had undergone ACLR and evaluate successful RTP. The authors of those studies did not include the surgeon of record for the players they reported in their studies. There was no unified surgical technique or rehabilitation protocol. Additionally, the authors of those studies did not communicate with the athletic trainers, physicians, therapists, and strength and conditioning coaches who were responsible for determining a player’s ability to return to NFL-level football. Reporting on RTP without communication between the authors and NFL organizational staff potentially introduces a strong risk of bias, as at the professional level, surgical recovery may not be the sole factor that goes into the decision to return a player to a roster.
The current study is unique in that it reported on a consecutive series of a large number of ACLRs by 2 surgeons (R.D.V. and D.E.C.) in NFL players using a consistent technique, graft selection, and rehabilitation protocol at a single center for over a quarter of a century. Further, we reported the results of all NFL players treated at our practice, regardless of team affiliation.
In addition, we suggest a new concept of return to previous participation (RTPP), which we believe is a more accurate measure of a professional athlete’s successful outcome after ACLR. We propose that professional athletes’ recovery should be considered a success if they are able to return to the same level that they previously participated at, regardless of participation in actual game play. There are many elite-level athletes who have recovered from ACLR and who may be part of an active professional roster, but some of them do not see actual game time. Their successful return to that level of sport should not be discounted. In order to encompass all NFL players that we believe made a successful return to sport, the term RTPP has been used in this study. In contrast, the previously established standard of measuring RTP by an athlete’s return to actual game play is referred to as return to game play (RTGP).
We hypothesized that our new definition of RTPP would result in a higher reported successful return rate compared with the similarly designed study by Shah et al. 8
Methods
Over the course of 27 years, 55 NFL roster players (who were subject to the NFL Injury Surveillance Program) had ACLR surgery performed by 1 of 2 surgeons at our institution. The current study is an institutional review board– and NFL/National Football League Players Association--approved retrospective evaluation of prospectively collected data over this period. Characteristic data, including date of injury, classification of injury, date of surgery, surgical findings, and surgical procedures, as well as the athletes’ recovery and RTPP or RTGP, were acquired from operative reports, clinical notes, the NFL Injury Surveillance System, publicly available information on the internet, and data acquired from the records of the team’s athletic trainers. All patients completed a minimum of 6 months of rehabilitation, but the exact follow-up duration of each patient was not recorded in this study. Descriptive statistics were calculated for all variables. Inclusion criteria were that the player (1) be a roster member of an NFL team; (2) have had an ACL injury that was treated with reconstruction; (3) had fully completed rehabilitation after the reconstruction; (4) was cleared by the surgeon to return to full activity with his NFL team; and (5) passed a preparticipation physical examination as per the terms of the NFL Collective Bargaining Agreement.
A total of 55 NFL players met the inclusion criteria. Of these, 8 were excluded for having had surgery too recently to allow for adequate follow-up at the time of manuscript preparation. The 47 NFL players who met inclusion and exclusion criteria were included in this study.
All players included in this study were treated by 1 of 2 surgeons at a single center. In all but 1 case, an arthroscopic transtibial single-bundle ACLR technique was performed with bone--patellar tendon--bone autograft and interference screw fixation. Meniscal and chondral injuries and their treatment were recorded, but review of these data were not part of the methods of this study. After surgery, all players underwent the same rehabilitation protocol (Table 1). The protocol consisted of a minimum of 6 months of standardized ACL rehabilitation therapy followed by a comprehensive dynamic functional movement program, with cord resistance and a progressive deceleration cutting program over 6 weeks before the athlete was cleared for participation.
Postoperation Rehabilitation Protocol a

a ROM, range of motion; RTGP, return to game play; RTPP, return to previous participation.
b Progression through this rehabilitation program is only partly dependent on postoperation time frame. We believe that it is important for the player to achieve good functional performance based on the volume of work at each level, before he is allowed to advance to the next level. A foundation is established, and then you build on it with each phase of exercise.
Supplemental data regarding a player’s draft status, position, or level of play if he was traded to another team were obtained from publicly available sources (www.nfl.com), interviews with team trainers, and NFL franchise records.
For the purposes of this study, RTPP was defined with 4 specific criteria (Table 2). In addition to using RTPP, we also calculated successful RTGP using previously published methodology, 8 by which a player is considered to have had a successful surgical outcome if he has played in at least 1 regular-season NFL football game after primary ACLR.
Criteria for RTPP a

a CBA, Collective Bargaining Agreement; NFL, National Football League; RTPP, return to previous participation.
Both RTGP and RTPP were determined for the group as a whole and for variables thought to predict RTGP and RTPP. Only 43 players were counted in the analysis using RTGP because players who had 2 ACLRs on the same knee were only counted for their first ACLR, as this is more consistent with the previously published RTGP definition where players with revision ACLRs are excluded. Risk factor analysis was performed using both RTGP and RTPP as well as seasons played after surgery. Given the low incidence of graft ruptures and contralateral tears in this small cohort, risk factor analysis was not performed for these variables.
Statistical Analysis
Descriptive statistics were generated for all data. Independent analyses were performed for each of 3 outcomes: RTPP, RTGP, and seasons played after primary ACLR. Univariate analysis was used to screen 6 potential predictor variables: surgeon, primary versus revision, round drafted, position, age, and number of ligaments reconstructed. Each predictor variable was dichotomized (surgeon 1 vs surgeon 2, primary vs revision, first 4 rounds of draft vs later than fourth round, offense vs defense, age ≤25 vs >25 years, and isolated ACLR vs multiligament reconstruction), and groups were compared using unpaired Student t tests (seasons played) and contingency analysis with a 2-tailed Fisher exact test (RTP). Only univariate predictors with P ≤ .2 were deemed significant and included in subsequent multivariate analysis.
Multivariate analysis was then performed using nominal logistic regression for dichotomous outcomes (RTP) and standard least squares linear regression for continuous outcomes (seasons played after ACLR). Risk factors were considered significant if P < .05 in multivariate analysis. Statistical analysis was performed using JMP 12 (SAS).
Results
Overall, 47 ACLR procedures in 43 players met the inclusion criteria for this study. There were 41 primary ACLR and 6 revision ACLR procedures. Of the 41 primary ACLR procedures, 9 had ≥1 ligaments repaired or reconstructed in addition to the ACL. Six were classified as ACL plus 1 additional ligament (medial collateral ligament [MCL] or lateral collateral ligament [LCL]) and 3 were classified as multiligament (ACL and posterior cruciate ligament [PCL] + MCL or LCL). Also, of the 41 primary ACLR procedures, 4 were contralateral isolated ACL tears in players who had already undergone isolated primary ACLR in their other knee. All of the 6 revision ACLR procedures were isolated ACL graft ruptures, and none of those players had contralateral ACL tears. The time to reinjury or contralateral ACL tear was not recorded.
Using previously published inclusion criteria and definition of RTGP, 8 total RTGP percentage in this cohort was found to be 67.6%. Using our inclusion criteria and proposed definition of RTPP, the overall RTPP for all NFL players sustaining isolated or combined ACL injuries requiring surgical reconstruction was 87.8%. For the players having 2 ACLRs (4 players total), RTPP was determined twice. The results of the univariate analyses are shown in Tables 3 and 4. Using the current study’s definition of RTPP, the average number of seasons participated in after surgery, for the entire cohort, was 2.6. For only those players who did RTPP, the average number of seasons played after surgery was 4.1 ± 2.82.
Univariate Analysis for RTPP After ACLR a
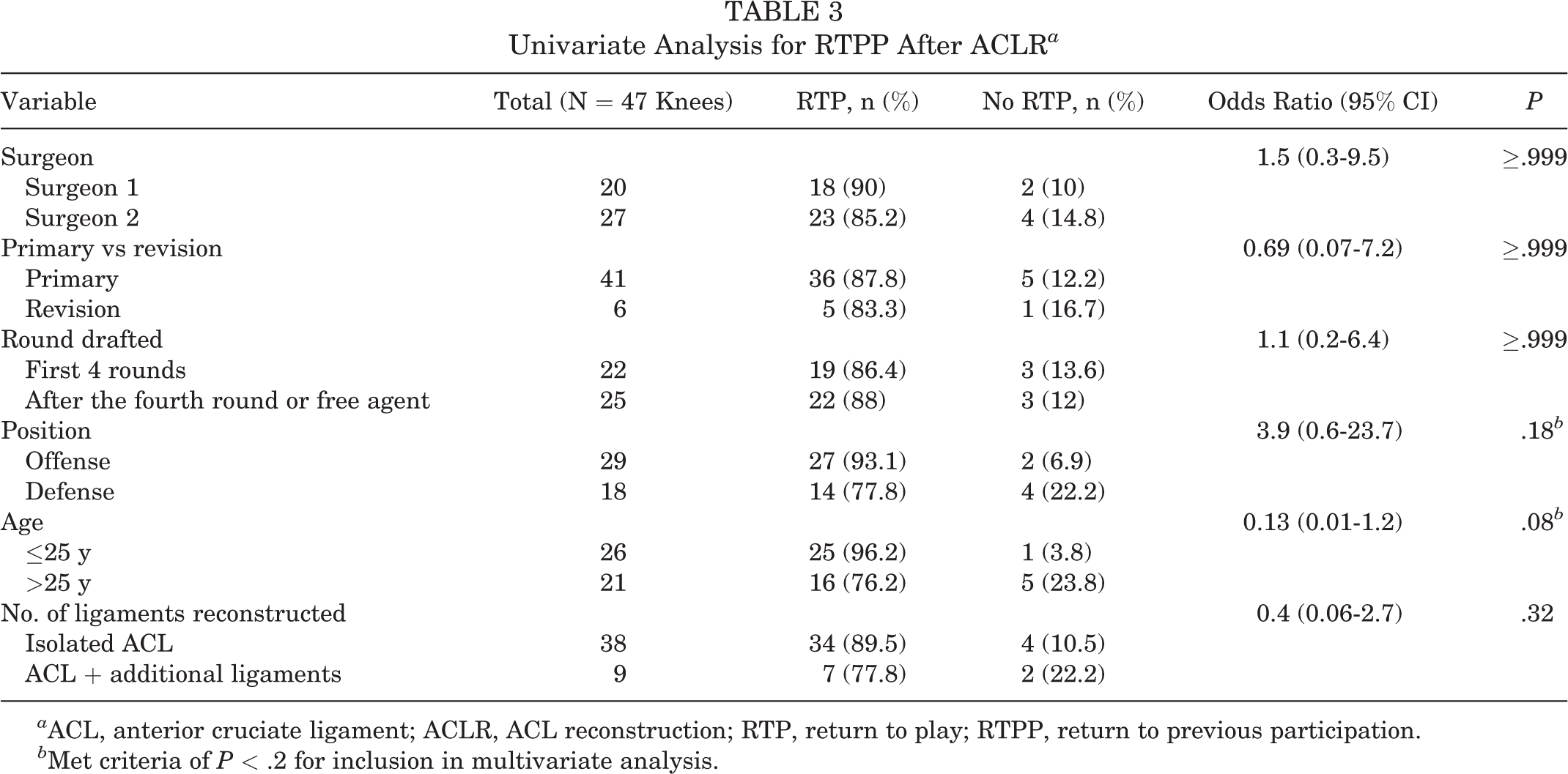
a ACL, anterior cruciate ligament; ACLR, ACL reconstruction; RTP, return to play; RTPP, return to previous participation.
b Met criteria of P < .2 for inclusion in multivariate analysis.
Univariate Analysis for RTGP a

a ACL, anterior cruciate ligament; RTGP, return to game play; RTP, return to play.
ACL graft rupture occurred in 4.3% (2/47). Contralateral ACL tears occurred in 8.5% (4/47). Thus, the subsequent occurrence of an ACL tear in either knee was 12.8%. Of the 2 ACL graft ruptures, 1 was an isolated graft rupture of a previous isolated primary ACLR and 1 was an isolated graft rupture of a previous isolated revision ACLR. All 4 contralateral ACL tears were isolated injuries that occurred in players who had previous isolated primary ACLRs.
In multivariate analysis with our proposed criteria (Table 5), age ≤25 years was an independent predictor of successful RTPP (OR, 10.8; 95% CI, 1.4-233; P = .02). In our cohort, 96.2% of players who were ≤25 years of age met the definition of RTPP compared with 76.2% of players >25 years. RTPP percentages under our definition were not significantly different for primary versus revision ACLR (P ≥ .999), however they were significant using the prior RTGP definition. High draft picks (rounds 1-4) and offensive players played more seasons after return (3.7 ± 3.3 vs 1.6 ± 2.4; P = .016) (Table 6). In multivariate analysis, offensive players played 1.18 more seasons after ACLR compared with defensive players (P = .009), and players drafted in the first 4 rounds played 1.48 more seasons compared with those drafted after the first 4 rounds or not drafted (P = .008) (Table 7).
Multivariate Analysis for RTPP a
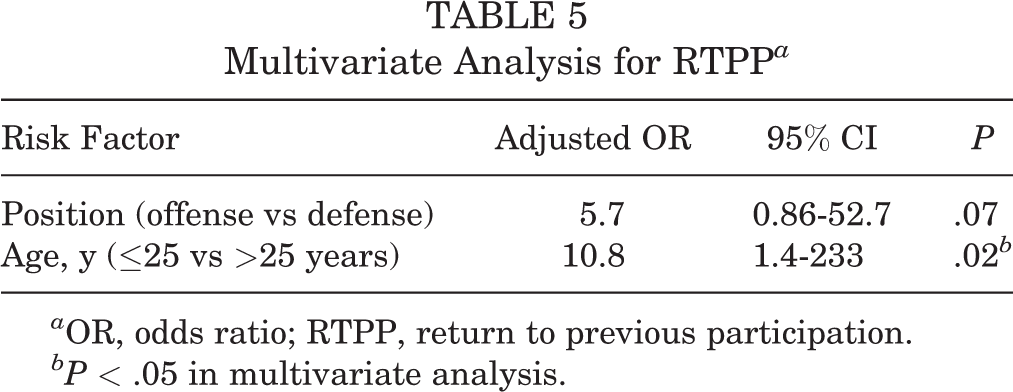
a OR, odds ratio; RTPP, return to previous participation.
bP < .05 in multivariate analysis.
Univariate Analysis for Number of Seasons of Participation After ACLR a

a ACL, anterior cruciate ligament; ACLR, ACL reconstruction.
b Met criteria of P ≤ .2 for inclusion in multivariate analysis.
Multivariate Analysis for Number of Seasons of Participation After ACLR a

a ACLR, anterior cruciate ligament reconstruction.
bP < .05 in multivariate analysis.
Discussion
This study reports the experience of 2 surgeons treating NFL players with ACL tears at the same center. A total of 43 NFL players had 47 ACLRs over a time period of >25 years using very similar surgical approaches and rehabilitation protocols. Further, the senior authors (R.D.V. and D.E.C.) performed all surgery, supervised rehabilitation, and made RTP decisions for all of these players. There is only 1 other similar study 8 on such a series of NFL players, but there are differences between the 2 reports. Notably, we introduced a new RTPP criteria that we believe to be more relevant than the prior RTGP criteria, and we reported on RTPP for revision ACLR.
Analysis of this cohort using the new RTPP criteria provides important information that can help predict which athletes might have a more successful RTP in the NFL. Younger age and playing an offensive position predicted a higher rate of successful RTPP with our new criteria. However, when using the RTGP criteria, younger age and position played were not significant predictors of successful return. Conversely, RTPP rates were no different between primary versus revision ACLR, but there was a significantly higher RTGP rate with primary ACLR compared with revision ACLR.
Our analysis also suggests that additional medial or lateral ligament repair did not significantly affect RTPP. However, we believe that any conclusion regarding multiligament knee injuries is limited given the small number of these injuries present in this cohort. NFL players who were high draft picks (rounds 1-4) or who were offensive players played, on average, more seasons after ACLR than other NFL players (Table 7). We speculate that higher draft picks played more seasons because of better overall talent, and it is not surprising that both our study and Shah et al 8 found that to be true after ACLR. The discussion of why offensive players play longer versus defensive players does not have explanation in the current literature. However, it is the opinion of the senior author (D.E.C.) that NFL teams favor using younger players on defense regardless of injury history, and offensive linemen tend to have longer careers than their counterparts on the defensive line. The factors that affect those variables include nonorthopaedic issues such as salary cap management.
Shah et al 8 studied RTGP (reported as RTP in their study) in 49 NFL athletes who underwent primary ACLR with or without additional procedures. Of those 49 athletes, 13 were isolated primary ACLRs. The authors did not report on revision ACLR. A total of 5 of 49 knees required open MCL repair, 2 required posterolateral corner repairs and 1 required a concomitant PCL reconstruction. The overall RTGP was calculated as 63%, where RTGP was defined as actually playing in an NFL game. 8 It is important to recognize that their report, similar to ours, included knees with additional injuries beyond an isolated ACL tear. In fact, only a minority of players in their study had isolated ACL tears. That factor can skew the data and results.
Read et al 7 published a study examining RTGP in NFL defensive players by comparing NFL players who underwent ACLR with a matched cohort of defensive players who had not undergone ACLR. They found that 74% of defensive players undergoing ACLR met a successful RTGP definition by returning to at least 1 NFL game. They also found that defensive players who started more games and had more solo tackles per game also had a higher probability of successful RTGP. In our study, using our new RTPP criteria, defensive players had a similar RTPP rate (78%) but were less likely to RTPP as compared with offensive players (78% vs 93%).
Okoroha et al 6 reported on RTGP in NFL players after revision ACLR between 2007 and 2014, hypothesizing that older and more experienced players would have a significantly increased RTGP percentages. They found that 79% (19/24) of those who underwent revision ACLR met RTGP criteria of returning to NFL regular-season play. Players who were drafted in the first 4 rounds were more likely to successfully return than those drafted in later rounds. These findings correlate with those of our study that high draft picks participated in more seasons after ACLR.
A previous study 4 has attempted to quantify NFL athletes’ performance after ACLR. Mai et al 4 reported that NFL players perform the worst after ACLR compared with other professional athletes, with the shortest postoperative career length, lowest survival rate, and largest decrease in performance. The overall RTGP in NFL athletes in their study was 82.4%. Prior estimates of the risk of contralateral ACL tear and ACL graft rupture in NFL athletes who had undergone ACLR were reported as 7.3% and 12.3%, respectively. In our series, contralateral ACL tear occurred 2 times more frequently than graft rupture; 8.5% and 4.3%, respectively.
Carey et al 1 reviewed the outcomes of ACLR in NFL running backs and wide receivers. They found the overall successful RTGP to be approximately 79% but that player performance, as measured by power rating, fell by one-third.
In addition to publishing the results of ACLR in this cohort, we proposed a new concept of RTP in a professional athlete: RTPP, which we believe more accurately captures what should be considered “successful” surgery and RTP in the professional athlete. We believe that prior definitions lower the perception of successful return by missing players who would otherwise be considered to have an excellent outcome. Examples of this oversight would be (1) players who return to their previous level of participation but who only play on the practice squad and (2) players who practice and make the active roster, but who do not play in a game (eg, backup quarterback).
Our experience suggests that regardless of RTP definition, the ACLR techniques and rehabilitation principles used during the study period led to a higher successful return percentage in the NFL than previous studies have reported. Depending on how it is defined, RTPP or RTGP, it is a stricter gauge of success than other standard measures of postoperative outcome and should not be compared with other scores. It is best to always interpret RTP rate in the context of the inclusion criteria and definition.
This study does have limitations. First, all patients were treated at a single center by 1 of 2 orthopaedic surgeons. RTPP rates may differ significantly at other institutions or with other surgeons. As part of the inclusion criteria, the 2 treating surgeons were responsible for clearing the players to return to full activity with their NFL team, and we acknowledge that this might introduce a selection bias to the cohort. Additionally, we acknowledge that this cohort represents a highly select patient population, and although there is interest in RTPP in professional athletes, these results may not accurately reflect RTPP rates in athletes at other levels of competition. Finally, the patients with revision ACLR and multiligament knee injury in this cohort were a very small group, and it is difficult to make any strong conclusion regarding our revision ACLR and multiligamentous injury findings.
Conclusion
Using our proposed criteria of RTPP, successful RTP after primary ACLR in NFL athletes was higher than previously reported RTP using RTGP measures. Additionally, our proposed RTPP criteria showed differences with the old RTGP criteria with regard to variables predictive of successful return. Younger age predicted successful RTPP, and higher draft round and offensive position predicted longer participation after ACLR. Concomitant reconstruction of a single collateral ligament did not affect RTPP or RTGP. There was no difference in RTPP rates when considering primary versus revision ACLR. Bicruciate plus collateral ligament reconstruction was associated with a lower RTPP rate but with small reported numbers.
Footnotes
Final revision submitted April 10, 2020; accepted April 27, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.R. has received educational support from Smith & Nephew and has received hospitality payments from Smith & Nephew and Stryker. D.E.C. has received consulting fees from Arthrex and Stryker and receives royalties from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Baylor Scott & White Research Institute (ref. No. 110649).