
Abstract
BACKGROUND:
Obesity and physical inactivity increase the risk for cardiovascular disease, Type 2 diabetes mellitus, hypertension, dyslipidemia and certain cancers. Exercise training and increased fitness promote positive changes in body composition and improve insulin sensitivity.
OBJECTIVE:
To investigate the effect of sequence order of combined strength and endurance training on new adiposity indices: visceral adiposity index (VAI), body adiposity index (BAI) and waist to hip ratio (WHtR) in overweight elderly women.
METHODS:
Forty overweight elderly women (age range: 60.34
RESULTS:
The results showed that the amount of weight, BMI, body fat percentage, BAI and WHtR have significantly decreased in E
CONCLUSION:
Sequence does not seem to play a role in the positive effect on current adiposity indices of the investigated training programs.
Introduction
Increasing prevalence of obesity and its relationship with chronic diseases such as diabetes, cardiovascular diseases, cancer and mortality put this disorder still on the top of health problems [1]. The first step to health programming is screening for and identification of obesity with easy and precise methods. Obesity which is said to the excess body fat can be identified precisely and reliably using imaging techniques such as magnetic resonance imaging (MRI), CT scan and dual-energy X-ray absorptiometry (DEXA), but in addition to be costly and time consuming, these techniques require skill in measuring and cannot be used for a large population. In contrast, anthropometric measures including waist circumference (WC), body mass index (BMI), and waist-to-hip ratio (WHR) are the most commonly used means to identify general and abdominal obesity [2].
BMI has been recommended as an international reference and standard for defining overweight and obesity [3]. Although a large number of health professionals are familiar with BMI index and use it in health care centers, BMI has some limitations: BMI is the index of total body fat but it gives no information about abdominal fat which is localized and has more to do with metabolic diseases. The other problem is that BMI does not differentiate between muscle body mass and body fat mass. Therefore, it is essential to replace BMI with accurate indexes which have fewer limitations [4].
Recently, it has been reported that these new indices including visceral adiposity index (VAI) and body adiposity index (BAI) make a reliable prediction of systemic diseases such as cardiovascular and metabolic disorder [5, 6].
VAI has been known as the fat distribution index showing metabolic risks indirectly. Moreover, VAI has been known as a useful tool for early detection of cardiac risk factors before metabolic syndrome develops. VAI is a simple mathematical relation based on gender-specific anthropometric models (WC, BMI) and functional parameters (triglyceride and HDL cholesterol) which shows body fat distribution and its function [7].
In an analysis conducted on 1518 Peruvian adults using a variety of actions to investigate obesity, VAI, WC and WHtR were the best predictors for metabolic syndrome. Especially, VAI has a good prediction power to show the risk of visceral obesity and high blood pressure [8].
In a large study, high VAI was associated with increased risk of coronary heart disease in Chinese men and women [9], however, there are also some conflicting results. A Canadian study showed non-superiority of VAI in predicting adipose tissue changes in postmenopausal women with low calorie diet in comparison to BMI and WC. These contradictory results have increased the need to prospective studies on VAI compared to other simple anthropometric ones [10]. Furthermore, research has shown that BAI can be used to show the body fat of adults, men, women and different ethnic groups without numerical modification. In another study, body fat was estimated using X-ray (DXA) and it was reported that hip circumference and height were highly correlated with body fat.
On the other hand, aging process leads to many adverse changes in body composition, muscular strength, aerobic capacity, health status and finally the practical capacity of persons [11]. Several studies have shown that endurance activity can reduce fat mass and increase muscles resistance to fatigue and increase in the maximum oxygen uptake (VO
Concurrent endurance-strength training in regular training program is called combined training. Various adaptation during combined strength and endurance training has been reported in the classic research conducted by Hickson and studies following that [16]. Due to the specificity of training effects, the combination of both endurance and strength training has been recommended for optimal physical performance and health in the elderly people [15]. We propose that combining strength and endurance training in elderly people to improve physical fitness, body composition and metabolic status is more effective than each of the training methods alone. Kitamura et al. after 12 weeks of combined endurance and strength training in 14 elderly men aged 65–73, observed an improvement in insulin function and a significant reduction in body fat percentage in both strength and combined groups [17]. In contrast, after 14 weeks of combined training in 12 middle-aged women, Fleck et al. found no significant changes in the total body fat tissue and all regional measures of fat tissue and body fat percentage [19].
The sequence order of training, that is, the sequence of performing strength and endurance training may affect training induced adaptations as well. However, about improvement in adiposity indices, only a few studies have reported on whether strength training should be done before or after endurance training in a training session [20]. Following 10 weeks of combined endurance-resistance training in sedentary postmenopausal women, Taleghani et al. observed a significant change in all anthropometric indices including body mass, abdominal circumference, waist circumference, waist – hip ratio (WHR), BMI, and body fat percentage [21]. Also, Tibana et al. investigated the effect of eight weeks of resistance training in overweight women. They found no significant changes in WHtR and BAI [22]. To the best of our knowledge, no comprehensive research has yet been conducted on the effect of combined strength and endurance training on new adiposity indices. Therefore, considering the importance of new adiposity indices in metabolic syndrome and some chronic disease, the current research aimed to investigating the effect of sequence order of combined strength and endurance training on new adiposity indices (VAI, BAI, and WHtR) in overweight elderly women.
Method
Subjects
Forty elderly healthy women (age: 60.34
Group assignment
After baseline assessments the participants were randomly assigned into 4 groups of 12 people. After the beginning of the experimental period, eight participants withdrew from the study due to personal reasons. At the end of the training period, the participants decreased to control group (N
Anthropometric measures
Fat percentage
Body fat percentage was calculated using 3-site skin fold test (triceps, thigh and suprailiac) value, measured with a Lafayette Skinfold Caliper II. The suprailiac, thigh, and triceps sites were selected, since they are included in the 3-Site model for women developed by Pollock et al. [24]. Sites were measured on a rotation basis. Each site was measured three times and the mean of these three measurements was calculated. The three measures were at a distance of 2 mm from each other.
Density: 1.0994921
Fat percentage
x
y
BMI
Weight
WHtR
Waist
In order to estimate VAI, the following women specific formula was used:
VAI
WC: waist circumference in cm;
TG: Triglycerides in millimoles per liter (mmol/L);
HDL: High-density lipoprotein in millimoles per liter (mmol/L);
BAI was estimated using the following formula [25]:
BAI
HC
Biochemical indices measurement
After 12 hours of overnight fasting, subjects attended the specialized laboratory at 9:00 AM and the initial 5 ml blood sample was drawn by laboratory expert from their antecubital vein. Then centrifuged blood sample and its serum sample were separated and stored frozen at
Complete strength and endurance training periodization
Complete strength and endurance training periodization
Modified Bruce protocol treadmill test was used to estimate maximal oxygen consumption of subjects. In this test, the subjects ran with a speed of 1.7 mph and a gradient of 0%. At three minute intervals the incline of the treadmill and the speed. The test continued until exhaustion. Testing time was measured and recorded. Estimated VO
VO
Muscle strength
Prior to the beginning of the muscle strength assessment, two familiarization sessions were performed with the following exercises: bench press, leg press, bent over lateral pull down, and bilateral biceps curl and bilateral triceps push down. During these two sessions, volunteers were expected to perform two series of ten sub-maximal repetitions, with 60 seconds of interval between series and exercises. Muscle strength was measured with the maximum repetition test (1-RM). The 1-RM leg press test used to measure the lower limb strength capabilities and upper limb strength was measured using 1-RM bench press test [27].
Maximal strength was calculated by using Berezicki equation [28]:
One Repetition Maximum (1RM)
In order to use this equation and evaluate the maximal strength, replacement of weight was repeated to maximal amount in leg press and bench press until getting fatigued and then, it was evaluated through placing amount of weight and number of repeats in Berezicki equation. It must be mentioned that Berezicki equation is used for repeats under maximal amount that would be less than 10. Previous studies have examined the validity of these tests and have shown a high reliability for older people [28].
Concurrent training protocols
After the preliminary tests, the exercise intervention consisted of eight weeks of combined (strength plus endurance) training. Experimental groups performed three training sessions per week. Each session consisted of 10 minutes for general warm up and 50 minutes exercise training, and 10 minutes for the cooling-down processes. All participants performed a familiarization session for becoming familiar with training procedures, intensity and equipment. The training program for strength-endurance (S
Experimental training protocols. E 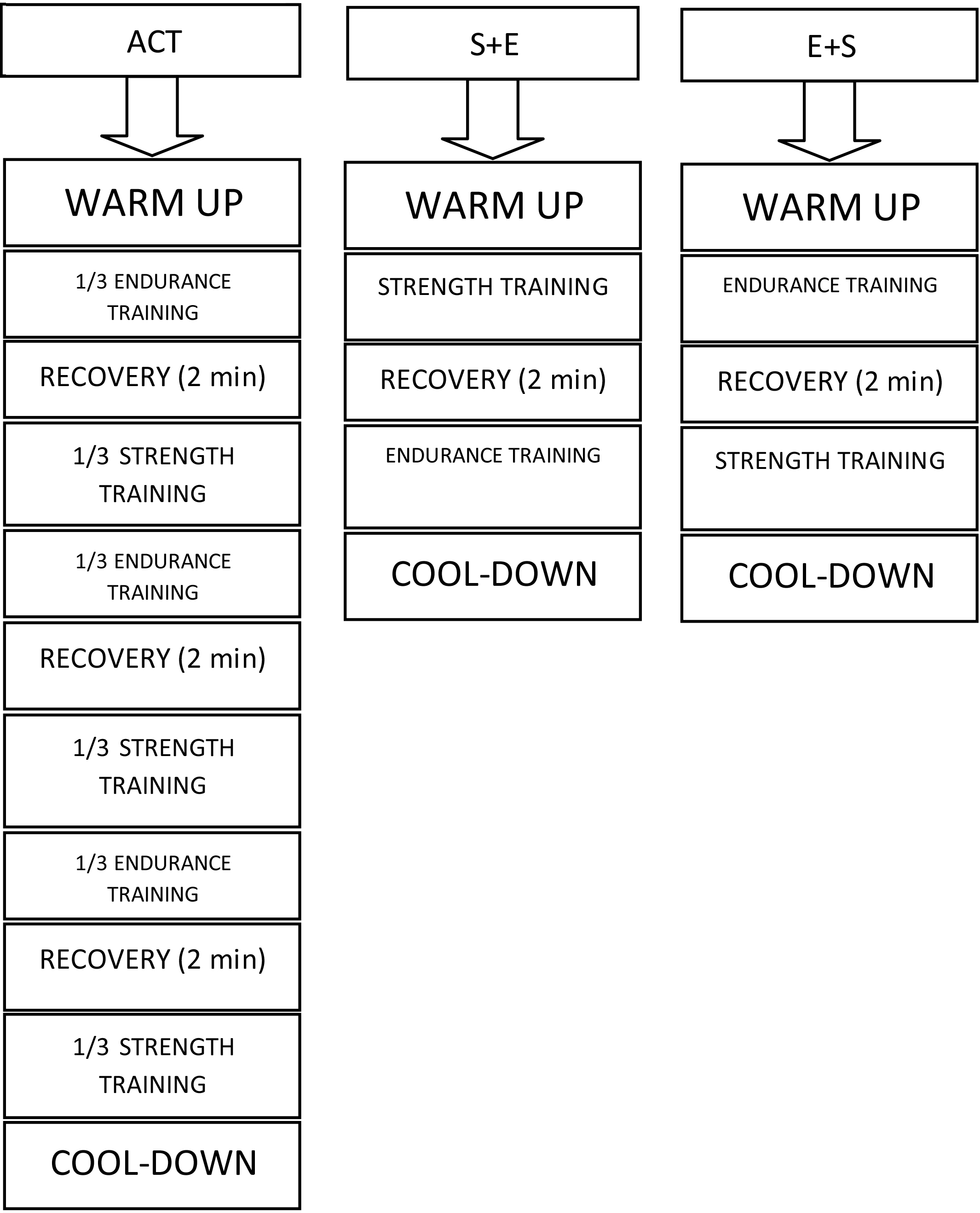
Changes in outcome variables within groups and between groups
Significance level at
Figure 1 shows the experimental training protocols.
This intervention was registered in Iranian Registry of Clinical Trials (IRCT) coded as IRCT2014123019995N3 and approved in the Research Deputy of Shahrekord University coded as 311254 3114 on May 25, 2014.
The SPSS statistical software package was used to analyze all data. Results are reported as mean
Results
The obtained results by the research showed a significant decrease in the weight, BMI, body fat percentage, and WHtR in experimental groups E
Discussion
The results of the current research indicated a significant decrease in BMI, body fat percentage, BAI, and WHtR among all 3 training groups, and no difference was observed between training sequence orders in reducing mentioned variables. Endurance training and strength training help with improvement of body composition by decreasing and increasing body fat mass, respectively. Training volume is a key factor in changing body composition. As training volume in combined training group is approximately 2 times of strength and endurance training volume alone, probably subjects enjoy the positive benefits of both types of training. Glowacki et al. observed the significant reduction of body fat percentage only in combined training groups [29]. Several studies demonstrated that performing combined training in a session leads to increased consumption of body fat. In this vein, Hu et al. investigated the effect of 12 weeks of aerobic, strength and combined trainings on risk of cardiovascular disease among overweight adult men and women. They found that combined training caused a significant reduction in BMI, weight and fat mass of subjects in comparison to other training methods. They ascribed this to the interactive effects of two training methods. Therefore, combined training can effectively influence persons’ body composition compared to other training methods alone [2]. Tan et al. reported that performing six months of combined training (aerobic and resistance) improved body composition and significantly reduced BMI and waist-to-hip ratio in elderly persons [30]. In addition, the results of the current research are in line with the results obtained by researchers who observed improvement of body composition indices after performing combined training in sedentary people [31].
Therefore, we suggest that combined training is an effective and efficient method for reducing body fat percentage and improving body composition, and the sequence order of training may have no effect on reducing the body fat percentage. Cadore et al. investigated the effect of sequence order of combined training in elderly men. The body fat percentage reduced in their research without any difference in sequence order of training [32]. Moreover, Alves et al. stated that the sequence order of training did not interfere with energy expenditure during combined training [33].
Glowacki et al., Cadore et al. and Shaw et al. observed a slight increase or no significant change in the body mass after combined training [29, 34, 35]. The result obtained by them is in contrast with the current research results. As the aim of resistance training program used in this research was not to create maximum hypertrophy, the intensities used in the current research may cause very little muscle hypertrophy or no hypertrophy in elderly persons. In the other studies a greater increase in muscle mass was observed by resistance and endurance combined training in a session [36, 37]. The increase of body mass may be due to different methods designed to change body composition. However, the results of the current research are the same as those obtained by Nindl et al., Gergley et al. and Dolezal et al. indicating the significant reduction of body mass after combined training [38, 39, 40].
When combined training is performed in a session, fat mass reduction and a slight increase or no change in fat-free mass causes body composition to change and eventually body mass to reduce. In this regard, it has been shown that in comparison to aerobic training, combined training enhances more the continuous growth of muscle mass and therefore, can help reduce fat mass by increasing the basal metabolic rate. In a recently conducted meta-analysis, Marzolini et al. reported that combined training is more effective than aerobic training alone in improving lean body mass, body fat percentage, and body fat mass in individuals with coronary artery disease [41].
In another study, following 10 weeks of combined resistance endurance training, Taleghani et al. observed a significant change in all anthropometric indices such as body mass, abdominal circumference, waist circumference, WHR, BMI, and body fat percentage [21]. These were in agreement with changes observed in our research exprimental groups. In addition, the results of several other studies are consistent with those of our research i.e. training leads to significant reduction in body mass and body fat percentage [34, 42]. But some of the studies did not show the efficiency of combined training [43]. The results of the current research are inconsistent with those obtained by Campos et al. [44]. They observed that combined training yielded no significant effects on body composition of elderly women. These inconsistencies may be due to the subjects’ age, gender and physical condition, the severity and duration of training, and methods of measuring variables in research.
The results of the current research indicate a significant reduction in BAI and WHtR in all 3 training methods. Considering the significant reduction of waist circumference in all 3 training methods, the reason for WHtR reduction can be attributed to the reduction of waist circumference. Moreover, the significant reduction of BAI is logical with regard to the significant reduction of hip circumference following combined training. In addition to VAI, the amount of triglyceride and HDL underwent no significant change after sequence order of E
As for the possible limitations of the present study, we concede the lack of sizeable enough strength and endurance training groups. This resulted from difficulty in recruitment of a sufficient number of participants that met with the inclusion criteria. Another limitation refers to the age of the subjects which e.g. under N. American or West European, and certainly Japanese, standards may not be considered as representative of elderly population. However, in terms of the local populace, they are but some care should be taken when extrapolating the findings into other parallel cohorts.
Conclusions
The current research indicate no significant differences among sequences of strength and endurance training for adiposity indices; all three training types seem to have the same efficiency in reducing new and old adiposity indices of elderly women. Consequently all protocols may be effective in promoting health of overweight elderly women.
Footnotes
Conflict of interest
None to report.