
Abstract
BACKGROUND:
Blood flow restriction (BFR) resistance exercise often elicits additive response of muscle activation. It is not clear whether local vibration (LV)-induced involuntary muscle contraction plus BFR would elicit an additive response of muscle activation.
OBJECTIVE:
To investigate the effects of LV exercise with and without BFR on muscle activation.
METHODS:
Eight physically inactive males were randomly assigned to a sequence of LV (0.45 mm amplitude, 35 Hz sinusoid, lasting 1 min) treatments on unilateral antagonistic muscle groups, including the upper arm (biceps and triceps), the calf (gastrocnemius, GAS; tibialis anterior, TA) and the thigh (rectus femoris, RF; biceps femoris, BF), in a repeated-measures counterbalanced design, with a 5-min interval separating the treatments. The LV treatments on each of the limbs included one bout of LV and one bout of LV
RESULTS:
Only the RF and biceps in the measured muscles showed greater electromyography (EMG) values during LV
CONCLUSIONS:
LV
Introduction
Performing regular resistance exercise has been demonstrated to elicit multiple health benefits [1]. However, for some populations, engaging in resistance exercise can be difficult. Hence, using portable devices that invoke involuntary muscle contraction as an alternative training modality might be of great significance. Recent studies have reported that individuals exposed to local vibration (LV) regularly can improve their leg extension strength [2, 3], suggesting that LV induces a somewhat similar response as that induced by resistance exercise and may thus be easily used as a training modality. LV is one form of the vibration, also known as direct vibration, in which a vibrator is often placed on the belly or the tendon of a specific muscle. Vibration can contract the users’ muscles involuntarily. This muscle contraction process is termed as tonic vibration reflex, where the muscle spindles work through the stretch reflex, which facilitates the activation of Ia-motoneurons, leading to involuntary muscle contraction [4]. Recent studies have reported that muscle activation was enhanced immediately following either LV with resistance exercise [5] or LV exposure alone [6].
Schematic timeline of the experimental procedure. LV 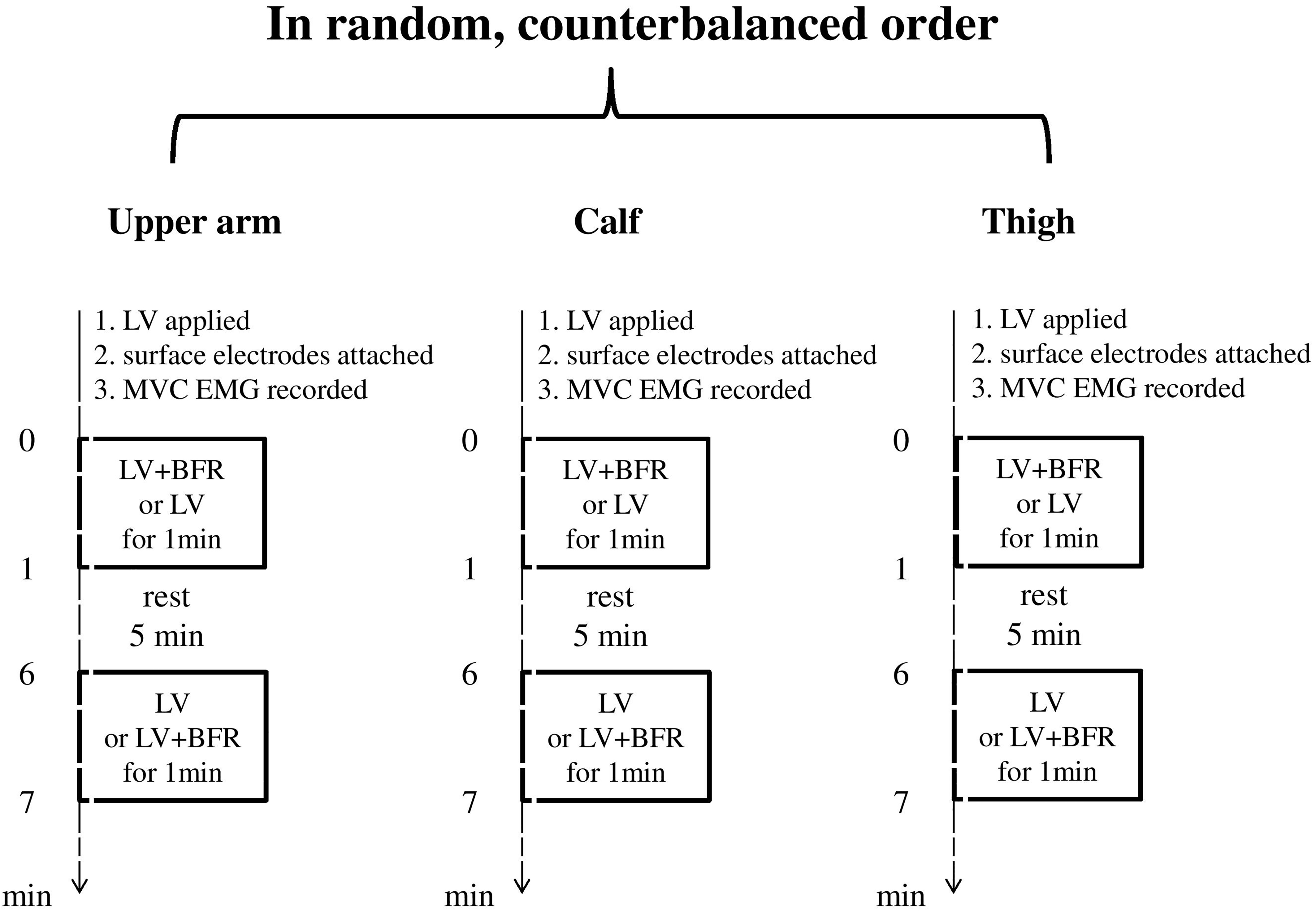
Moreover, research conducted in the last few deca-des has indicated that 20%–30% of the one-repetition maximal (1 RM) of low-intensity resistance exercise combined with blood flow restriction (BFR) results in muscle hypertrophy and strength gain in adaptations similar to those of traditional high-intensity resistance training [7, 8, 9], which has been proposed as an alternative to heavy resistance training [8, 9]. This emerging strength training method, in which the proximal portion of the exercising muscles is typically compressed by wrapping an inflated cuff or wraps, is termed as occlusion training or BFR resistance exercise [8]. During BFR resistance exercise, the venous return of blood flow from the muscles is reduced, and even the arterial inflow into the muscles is reduced depending on the cuff pressure applied [10], which might result in an ischaemic/hypoxic environment, subsequently leading to increased metabolites [11, 12]. The increased metabolites due to BFR may increase the perceived effort and muscle activation, showing a greater electromyography (EMG) value during BFR resistance exercise than that during resistance exercise alone [8, 13]. Although the mechanism underlying BFR resistance training induced-muscle adaptation is not completely understood, it has been speculated to be related, in part, to an increase in muscle activation [14, 15].
Root mean square (RMS) electromyography (EMG) values (mean
Given that an additive effect of BFR resistance exercise is often observed under low-intensity resistance exercise [8, 10, 11, 12, 13], and EMG analysis indicated that the magnitude of muscle activation immediately following LV leads to low intensities of muscle contraction (range: 3.54%–11.55% of maximal voluntary contractions, MVCs) [5, 6], the spurring hypothesis is that even adding BFR during this involuntary muscle contraction process can further increase the muscle activation.
Therefore, the aims of this study were to investigate the effects of LV
Subjects
A total of eight healthy males (mean
Study design
Prior to the experiment, the participants were familiarised with the experimental procedures and devices. In the experimental session, the participants were randomly assigned to a sequence of LV treatments on unilateral antagonistic muscle groups, including the upper arm (biceps and triceps), the calf (gastrocnemius, GAS; tibialis anterior; TA) and the thigh (rectus femoris, RF; biceps femoris, BF) in a repeated-measures design. The treatments were proceeded by two vibrators respectively strapped onto the skin over the belly of the specific antagonistic muscle groups, and then the antagonistic muscles were exposed to LV for 1 min simultaneously. Each of the three limbs was subjected to one bout of LV and another bout of BFR applied on LV in a counterbalanced order, with a 5-min interval separating treatments (Fig. 1). To emphasise the character of passive exercise, during each treatment, the participants were requested to maintain a comfortable and relaxed seated posture, with the knee angle at 90
LV devices and protocol applied
Briefly, the custom-designed electromechanical vibration device consists of one control unit, two vibrators (0.45 mm amplitude, 35 Hz sinusoid) connected to the control unit and a medically approved power supplier, which results in a peak acceleration of 2.2 g as calculated using the Lorenzen formula [18]. The acceleration is within the range to stimulate the increase in muscle strength when using regularly [3]. Each vibrator has an encoder. The rotating element inside the vibrators is a cylindrical brass component with a length of 30 mm, a diameter of 24 mm and a thickness of 18 mm (weighing about 38.5 g) (Fig. 2). The vibrators were properly fixed to the skin with an elastic belt to prevent from swinging and to avoid movement artefact.
The local vibrators.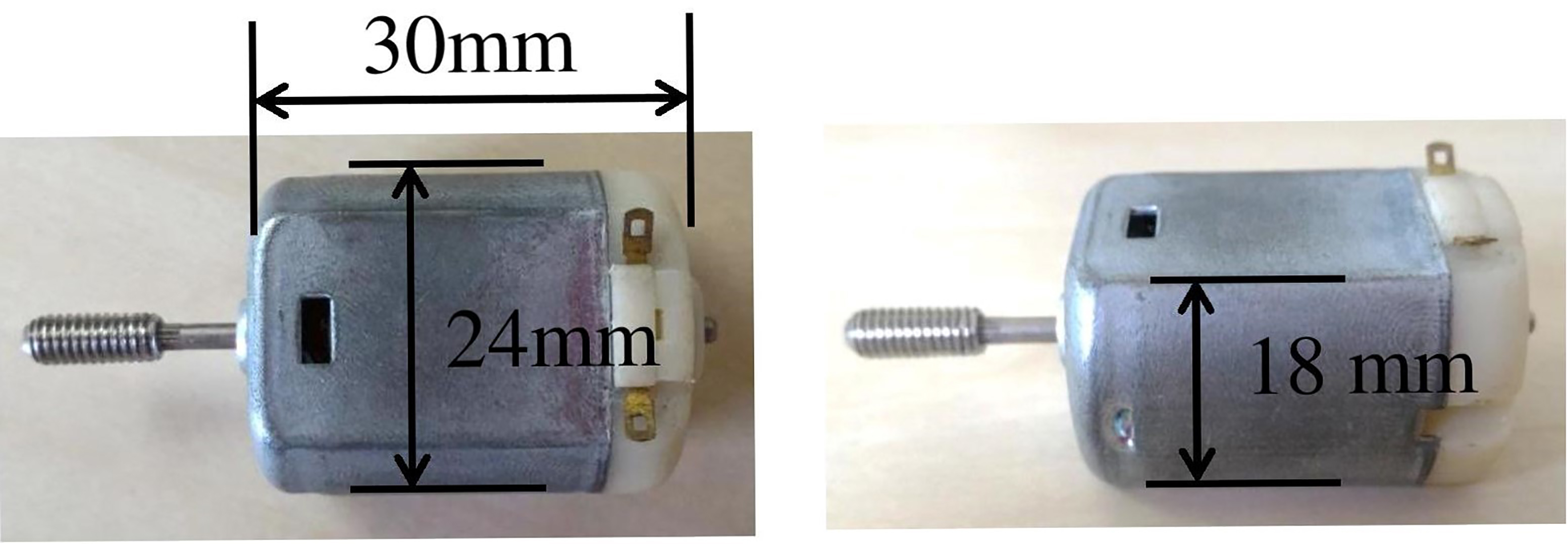
In the LV
EMG signal analyses
Each participant’s skin was shaved, abraded and cleaned with alcohol to minimise impedance, after which bipolar surface electrodes (Ag/AgCl, 3M Health Care, St. Paul, MN) were applied on the RF, BF, GS, TA, biceps and triceps right below the vibrators, and the ground electrode was placed over the epicondyle of the tibia. The EMG signals were collected using the Noraxon Telemyo DTS EMG system (Noraxon Inc, USA) and were amplified (
Statistical analyses
Data are expressed as the mean
Results
The paired
Discussion
To our knowledge, this is the first study to examine the effects of a passive LV exercise with BFR on the muscle activation of both the upper and lower limbs. The primary finding of this study was that the external compression applied on the limbs during LV exposure-magnified muscle activation is muscle-specific, which is only pronounced in the RF and biceps, with no further effect on BF, GAS, TA and triceps.
Recent research has indicated that low-intensity resistance exercise combined with BFR enhanced the muscle activation of both the upper and lower limbs, as demonstrated by EMG analysis [13, 20]. A review article on BFR exercise indicated that lower body restrictive cuff pressures ranging from 160 to 240 mmHg are effective in increasing metabolic stress, due to partial but not complete arterial flow restricted to the muscle [19]. It has been reported that the larger circumference of the limb requires a higher cuff pressure to elicit sufficient occlusion effect during BFR exercise [21]. To let the venous outflow of the arm and calf muscles (smaller than the thigh in circumference) were apt to occlude, the cuff pressure on the thigh in the current study was also applied on the upper arm and calf muscles during LV
The recommended cuff pressure for the lower limb while applying for the upper arm may make individuals feel tight and theoretically elicit greater levels of BFR than those applied on the lower limb due to a smaller circumference, which may be easier to magnify the muscle activation response when BFR is applied during LV. In general, as expected, greater EMG amplitude was found in the biceps, the part of the upper arm where BFR was applied with LV. Biceps are the antagonist muscles to the triceps; when the elbow flexes, the biceps shorten or contract and the flexion is the opposite action of a triceps extension. In the current study, the participants were required to maintain a sitting posture that approaches the natural resting position, with the elbows bent to 90
When the calf muscle was exposed to LV with or without BFR sessions, the participants maintained an anatomically natural sitting posture, with the knee bent to 90
With regard to the thigh muscles, during the LV
Regarding the results obtained in the present study, some limiting factors become relevant and warrant emphasis. First, to facilitate the comparison among different limbs, we utilised uniform cuff width and pressure for all limbs, which might have led to a disproportionate increase in BFR levels even when the participants were physically inactive. Second, since the vibrators were applied on the mid part of the target muscles, the EMG electrodes attached on the belly of the RF approaching the vibrators may not fully reflect the maximal muscle activity when exposed to LV, despite normalisation of the data. In spite of these limitations, the findings provide information on the target muscle activation with LV
In conclusion, this study provided some evidence that the combination of LV and BFR promotes an increase in muscle activation, with obviously higher values in the RF for the lower limb and in the biceps for the upper limb. The greater muscle activation of the RF and the biceps during LV
Footnotes
Acknowledgments
This work was partially supported by the Ministry of Science and Technology, ROC (MOST 103-2511-S-110-010-MY3). The authors greatly appreciate Chang-Ju Li, Hao-Ting Chen, Po-Chou Shih, and Jih-Wei Chung for experimental assistance.
Conflict of interest
All the authors declare no conflict of interest.