
Abstract
BACKGROUND:
The palmaris longus (PLM) is a fusiform-shaped muscle that appears in the superficial flexor compartment of the forearm. It has been suggested that PLM is a phylogenetically degenerate metacarpophalangeal joint flexor.
OBJECTIVE:
The aim of this study was to compare the strength of wrist flexion and extension in healthy volunteers with and without the PLM.
METHODS:
Sixty-four healthy subjects, 30 men and 34 women, 18–22 years old were enrolled in this study. The database consisted of 128 wrist tests. The inclusion criteria were as follows: sedentary lifestyle, unknown musculoskeletal disorders and right-handedness. Musculoskeletal ultrasound imaging was used for assessing the presence of PLM. A hand-held digital dynamometer was used to assess the peak force of wrist extension and flexion. Data were analyzed separately for women and men
RESULTS:
The existence of right-sided PLM was 73.3% in male subjects and 55.9% in female subjects. For men, the strength of wrist flexion was 36.03
CONCLUSIONS:
The existence or absence of PLM plays no role in the strength of either the flexors or extensors of the wrist.
Introduction
Palmaris longus muscle (PLM) is a fusiform shaped muscle which is arranged in superficial flexor compartment of the forearm [1, 3]. It springs from the medial epicondyle and converges on a long tendon which broadens out to become a flat sheet and become adjoined into the palmar aponeurosis. It has been suggested that PLM is a phylogenetically degenerate metacarpophalangeal joint flexor [3, 10]. PLM has significant anatomical variance, and the complete absence of the muscle is the most common variation [10, 13]. The absence of PLM differs according to race, ethnicity, sex and the handedness [14, 18]. There are variable reports in the literature about the prevalence of the agenesis of PLM ranging from 3.4% to 63.9% [12, 18]. Because PLM is easily palpated and very superficial in the forearm, it is easy to harvest, so it is the most common source of an autologous tendon graft in different reconstructive surgeries [2]. The elbow does not lose their functions after tendon harvesting operations [2, 7]. Recent studies focused on the effect of the absence of PLM on the forearm and hand strengths and functions. The associations with grip, pinch and thumb abduction strength in the absence of PLM or its effect on fatigue resistance and proprioception of the hand were studied before [6, 8, 15, 17]. Although PLM is located in the flexor compartment of the forearm, to the best of our knowledge, no trials have investigated the contribution of the PLM to the strength of wrist flexion and extension.
Therefore, the aim of this study was to compare the strength of wrist flexion and extension in healthy volunteers, with and without PLM.
Methods
Subjects
Seventy healthy subjects between the ages of 18 and 22 years, have volunteered to take part in this trial. This study was conducted in the Department of Physical Medicine and Rehabilitation at the Training and Research Hospital of Konya/Turkey between September and November 2016. Informed consent was obtained from all individual participants included in the study. The protocol of the study was approved by the Ethic Committee of the University of Necmettin Erbakan No: 2016/645. The inclusion criteria were as follows: 18–22 years of age, sedentary lifestyle (no or irregular physical activity), non-smoking, body mass index of 22–25 kg/m
Instrumentation and procedures
Musculoskeletal Ultrasound (MUS) imaging was used to assess the presence of the PLM. The examination was performed by an experienced physiatrist and a radiologist. One hundred and twenty-eight forearms were evaluated with a linear array probe (8–15 MHz). Subjects were seated on a high swivel chair to provide easy examination of semi-flexed elbow. Scanning began on transverse axis from the attachment point of the PLM (medial epicondyle of humerus) and followed distally. A transverse sonogram was obtained from muscle bely at proximal to distal over the tendon. A Long axis confirmation was also performed.
Wrist flexion and extension strength was measured by an independent physician who was blinded to the MUS results. A calibrated computer-assisted hand-held dynamometer was used (MicroFet2 TM Hoggan Health Industries, West 130 Jordan, UT, USA) to assess the peak force during wrist extension and flexion. A 5-minute warm-up exercise for the upper extremities was performed before the evaluation. The dynamometer and the forearm were fixed and wrist movement was conducted by exerting maximum effort for flexion or extension movement for three seconds (Fig 1a–b). Care was taken to ensure that the subjects’ forearm did not lose contact with the surface during the measurement. Three tests were performed alternatively for each side. The average of the three tests was recorded and the average flexor/average extensor strength was calculated to determine the agonist/antagonist ratio.
The set up for the dynamometric measurements. 1a – wrist flexion 1b – wrist extension.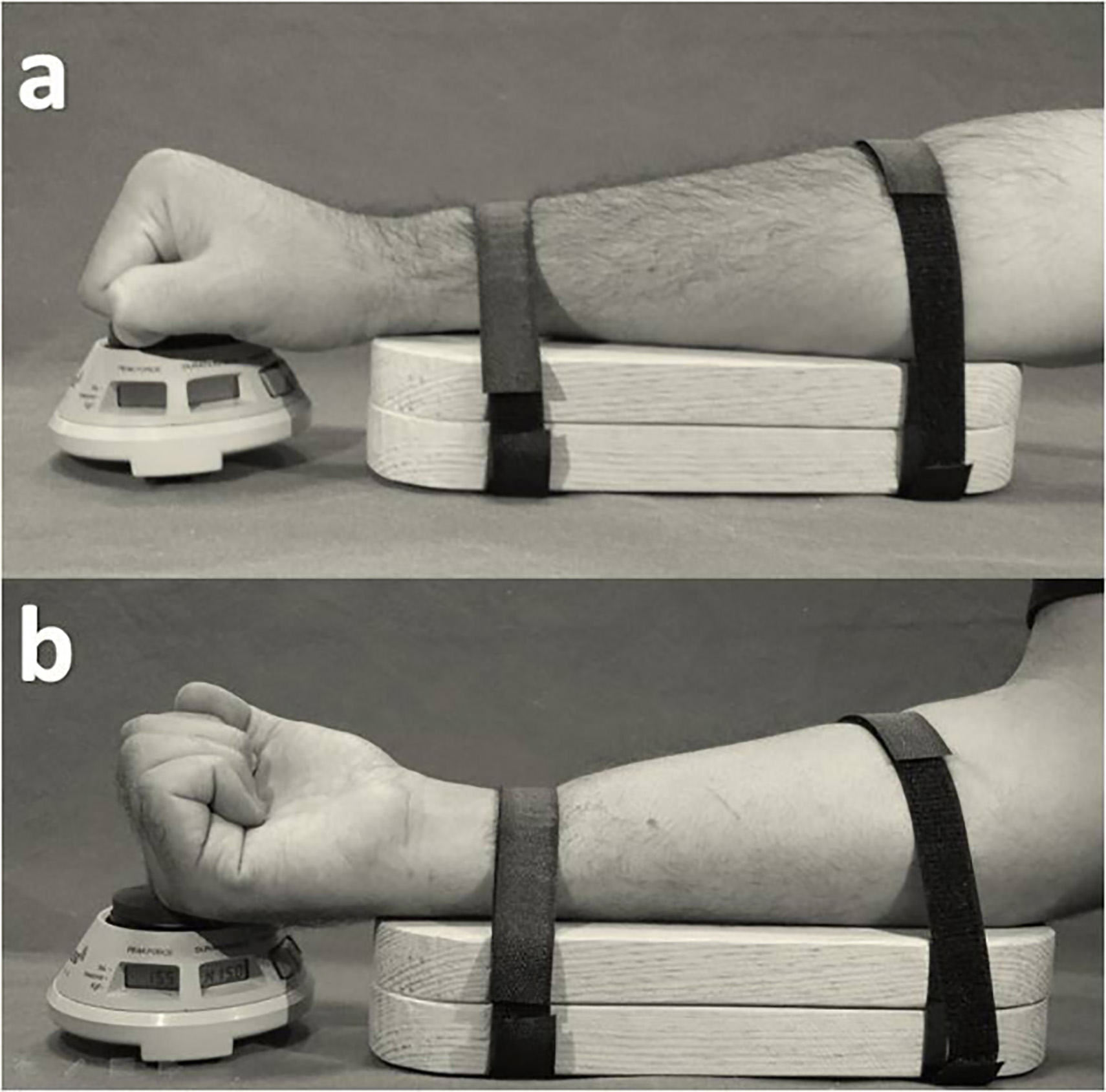
The SPSS for Windows 11.0 software package was used for the statistical evaluation of the data. All data were analyzed separately for women and men. Descriptive statistics were analyzed and reported as mean (with standard deviation), or as percentiles as appropriate. The Kolmogorov-Smirnov test was used to test the normality of the distribution of the data within the groups. For the comparisons between the groups, non-parametric Wilcoxon Signed Ranks Test was used; a p-value (two-tailed) of less than 0.05 was taken as significant.
Results
Of the 70 individuals who were initially recruited, 3 had carpal tunnel syndrome, 2 had history of fracture and one subject had a surgery history for Kienbock’s Disease. Thus the final N was 64, 34 women and 30 men, totaling 128 wrists. The demographic variables of participants and the presence of the PLM according to gender and lateralization is summarized in Table 1. The strength scores are outlined for men in Table 2 and for women in Table 3. In both gender, there was no significant statistical difference between PLM present (
Demographic variables of the participants
Demographic variables of the participants
Comparison of muscle strength in men
Comparison of muscle strength in women
This is the first clinical study which aimed to evaluate the effect of PLM on wrist flexion and extension strength in healthy subjects. The main finding of this study is that the PLM plays no role in effecting these movements in young normal individuals.
Muscle strength depends on certain variables, including age, sex, body mass index, and level of physical activity [9, 11]. The influence of sex, age, and hand dominance on muscle strength was assessed in previous studies which evaluated the contribution of PLM to various activities [6, 8, 17]. In this study, we chose to test young right-handed subjects with a BMI of 22–25 kg/m
Unlike conventional methods such as the “traditional test”, “Gangata test” or “adducted five-finger test” which are performed for validating the presence of PLM [6, 8, 15, 17] in this study we used for probably the first time USG imagining in order to detect the belly of the muscle and follow the tendon trough distally. This process enabled the exclusion of PLM variations which may affect the results.
In previous explorations of the relationship between the presence of PLM and muscle strength Cetin et al. [6] and Sebastin et al. [15] studied the effect of the PLM on grip and pinched strength in healthy subjects. While Sebastin et al.’s was based on adults without any age limitation Cetin et al.’s tested children 6–11 year old. During forceful grip the hand flexors generate the force while the extensors stabilize the wrist and maintain optimal length-tension relationships [1]. All of the muscles which are associated with carpometacarpal, intermetacarpal, metacarpophalangeal and interphalangeal joints are involved in this compound movement. Also, muscles such as flexor digitorum profundus and flexor pollicis longus which contribute to both wrist flexion and gripping having a role [1, 9]. Because the absence of the PLM might be easily tolerated by the other structures, it is difficult to demonstrate the effect of this muscle on grip strength. Thus Cetin et al. [6] and Sebastin et al. [15] reported that the absence of the PLM was not associated with either grip or pinch strength. Gangata et. al. [8] compared thumb abduction strength between hands in those subjects who had unilateral presence of PLM. Thumb abduction strength was significantly stronger on the hand with a PLM than the one without it in participants with the unilateral presence of the PLM. According to Boatright et al. [4] and Liu et al. [13]thumb abduction and wrist flexion strength could be used as an indirect indicator of PLM function. In variance with this view, our findings do not support a role for PLM in wrist flexion.
Vercruyssen et al. [17] elaborated that the absence of PLM was not related to fatigue resistance proprioception of the hand and grip strength in athletes [17]. Grip strength and fatigue resistance were measured with a hand dynamometer in this study. The time during which grip strength dropped to half of its maximum was noted as fatigue resistance.
We also studied extensor muscle strength of the hand to calculate agonist/antagonist ratio for the wrist. Our results reveal the presence or absence of the PLM is not associated with the agonist/antagonist ratio of the wrist. Extreme differences between the prime movers and the antagonist muscle strength in any joint have been reported to be associated with the rate of joint stability, fatigue, and rate of injury [5]. According to our results, the presence of PLM does not have a substantial effect on the agonist/antagonist ratio of the wrist. Our results will, therefore, be more meaningful in clinical practice and may especially help decisions regarding PLM harvesting operations.
Tendon grafts are frequently used in reconstructive surgery for various purposes such as management of facial paralysis, ptosis correction, lip augmentation, or tendon reconstruction in the limb [2]. Most authors agree that the PLM is the choice as a tendon donor since it is easily available on the surface of forearm and also fulfils the requirements of length and diameter. Also, there is unlikely to be any functional loss of the hand following the harvest of the PLM [2, 3]. Authors divide patients who require PLM as a graft into two groups [8, 15]. One group have a normal upper limb and the PLM is harvested for reconstructive surgery of other parts of the body whereas in the other group the muscle is harvesting for upper limb surgery. The second group can be further subdivided into two groups where the first is intended for PLM harvesting serving any reconstruction in which the wrist flexors are not involved. In the second subgroup, the wrist flexors or thumb abductor muscles on the ipsilateral side need a reconstruction with this autologous tendon graft. Except this second subgroup, functional influence of the PLM in the harvested side is unexpected [8, 15]. Our study results confirm this observation.
There are some limitations to our study that need to be acknowledged. Isokinetic testing is the gold standard test for muscle strength testing. However, the high reliability of hand-held dynamometer used for the present study convinced us to apply it for the specific topic we explored. In addition, isokinetic dynamometry is a very expensive device which is not available very widely. Second, we would have preferred to use a sample of patients who will be operated for PLM harvesting. In such case a comparative before-after harvesting paradigm could give us more functional results regarding contribution of the PLM to hand functions.
Conclusion
Based on the results of this study, although PLM is a fusiform-shaped muscle arranged in superficial flexor compartment of the forearm, it has no significant effect on wrist flexion or extension strength or on the agonist/antagonist ratio. These points should be considered for methodological as well as surgical objectives.
Conflict of interest
The authors declare no conflict of interest.
Funding
The authors received no financial support for the research.