
Abstract
Purpose:
We aimed to compare the clinical results and the complications between the minimally invasive modified Camitz opponensplasty and the conventional Camitz opponensplasty for severe carpal tunnel syndrome (CTS), and to evaluate the efficacy of the modified technique for CTS.
Methods:
Twenty-eight hands in 24 patients with severe CTS who had disorder of the thumb opposition with thenar muscle atrophy (group 1) were treated by minimally invasive modified Camitz opponensplasty, passing the transferred palmaris longus (PL) tendon under the abductor pollicis brevis (APB) fascia using only palm and thumb incision, and no incision to either wrist crease or forearm. Ten hands in 10 patients (group 2) were treated by the conventional Camitz opponensplasty. Clinical evaluation was made by comparing the results before and after surgery for the angle of the thumb palmar abduction, pinch power, and grip strength.
Results:
All clinical findings significantly improved after surgery compared with before surgery in all patients. In group 1, there were no complications including transferred tendon bowstring, painful wrist scar, or injury to the palmar cutaneous branch of the median nerve in all hands. Conversely, patients in group 2 had four painful wrist scars and nine bowstrings of the transferred tendon.
Conclusions:
Several complications have been considered to attribute to the long incision and an extensive dissection crossing the wrist crease from the palm to the wrist in the conventional Camitz procedure. The current modified Camitz opponensplasty by minimally invasive incision without straddling the wrist crease is a simple and effective procedure that can decrease the risk of painful scar around the wrist crease in severe CTS patients with disorder of thumb opposition. Additionally, this technique, by passing the transferred PL tendon under the APB fascia, is useful in restoring the thumb opposition immediately, and in preventing the bowstringing of the transferred tendon.
Introduction
Thenar muscle atrophy, especially abductor pollicis brevis (APB) atrophy, is frequently observed in patients with long-standing severe carpal tunnel syndrome (CTS). 1 –12 Moreover, most advanced CTS patients with thenar muscle atrophy have severe disorder of thumb opposition and difficulty with activities of daily living. 1 –12 Thumb opposition is essential in providing motion and strength for both pinch and grasp, and, therefore, it is important to restore it for these CTS patients. 1 –12
Opponensplasty is a standard and effective procedure that improves thumb opposition to achieve fine finger movement. 1 –12 Presently, various methods of opponespalsty have been reported. 13 –18 Especially, the Camitz opponensplasty using the palmaris longus (PL) is the most commonly employed tendon transfer for severe CTS patients with distinct significant thenar muscle atrophy and loss of thumb opposition. 2 –12,15 Currently, the Camitz opponensplasty combined with carpal tunnel release is a standard procedure using the PL transfer continued with a strip of palmar aponeurosis to the insertion of the APB. 2 –12 Foucher et al. reported that the Camitz opponensplasty combined with carpal tunnel release provided 90.7% good long-term results. 2
However, several complications have been reported with the conventional Camitz procedure. This procedure requires a long incision and an extensive dissection crossing the wrist crease from the palm to the wrist, to harvest a strip of palmaris aponeurosis and to lengthen the PL tendon. 2 –4,6 –12 The appearance of a painful scar on the wrist has been considered to be due to the extended skin incision straddling the wrist crease. 1,3,10,11,19 Additionally, the extensive soft tissue dissection may increase the risk of iatrogenic injury to the palmar cutaneous branch of the median nerve around the wrist, poor wound healing, and infection, especially in elderly patients. 1,3,10,11,19 Moreover, the prominent bowstringing of the transferred tendon has been widely reported as one of the main shortcomings in the conventional Camitz opponensplasty. 1 –3,5,10,19 We assumed that this weakness occurred because the transferred tendon straddled over the wrist crease runs too radially under the skin. Therefore, we considered that bowstring of the transferred tendon may be overcome by passing the tendon under the APB fascia using a small palm incision without straddling the wrist crease. However, there have been no reports concerning modified Camitz opponensplasty using only minimally invasive palm and thumb incision, and by passing the transferred tendon under the APB fascia with no incision to either the wrist crease or forearm for severe CTS.
The purpose of this study was to compare the clinical results and the complications between the minimally invasive modified Camitz opponensplasty and the conventional Camitz opponensplasty for severe CTS patients with thenar muscle atrophy, and to evaluate the efficacy of the modified technique. It was considered that this modified procedure may be useful and effective not only to immediately restore thumb opposition, but also to prevent bowstringing of the transferred tendon and painful scarring on the wrist.
Materials and methods
We recruited 34 patients (38 hands, 9 men, 25 women, mean age 65.6 years with a range of 52–83 years) who were clinically diagnosed and confirmed by electrophysiological studies with severe idiopathic CTS. The affected hands were the right in 14 patients, the left in 16 patients, and bilateral in 4 patients. The duration of follow-up ranged from 12 months to 38 months (mean 19.1 months). Patients were excluded if they reported a history of systemic disease associated with a higher incidence of CTS, such as rheumatoid arthritis, thyroid disease, hemodialysis, amyloidosis, osteoarthritis of the thumb carpometacarpal joint, or traumatic injuries to the upper extremities. All treatments and examinations proceeded after signed consent was obtained from all patients in this study. All patients had severe thenar muscle atrophy and subjective symptom with disorder of thumb opposition causing inability to pinch and grip adequately during activities of daily living. All electrophysiological examinations were performed according to the American Association of Electrodiagnostic Medicine guidelines 20 by one examiner (MN) using a Neuropack X1 MEB 2312 (Nihon Kohden Corporation, Tokyo, Japan) before surgery in all hands. The electrophysiological examinations before surgery demonstrated that both the compound muscle action potential of the APB and the sensory nerve action potential of the index finger were unrecordable by stimulating the median nerve on the wrist in all hands. Namely, all cases were categorized to the “extreme” grade by the Padua classification. 21
Patients were organized into two groups: those who underwent the minimally invasive modified Camitz opponesplasty (group 1), and those patients who underwent the conventional Camitz opponesplasty in which the incision continued proximal to the wrist proximal crease (group 2; Table 1). In all hands, the opponensplasty was performed concurrently with open carpal tunnel release.
Patient demographics.
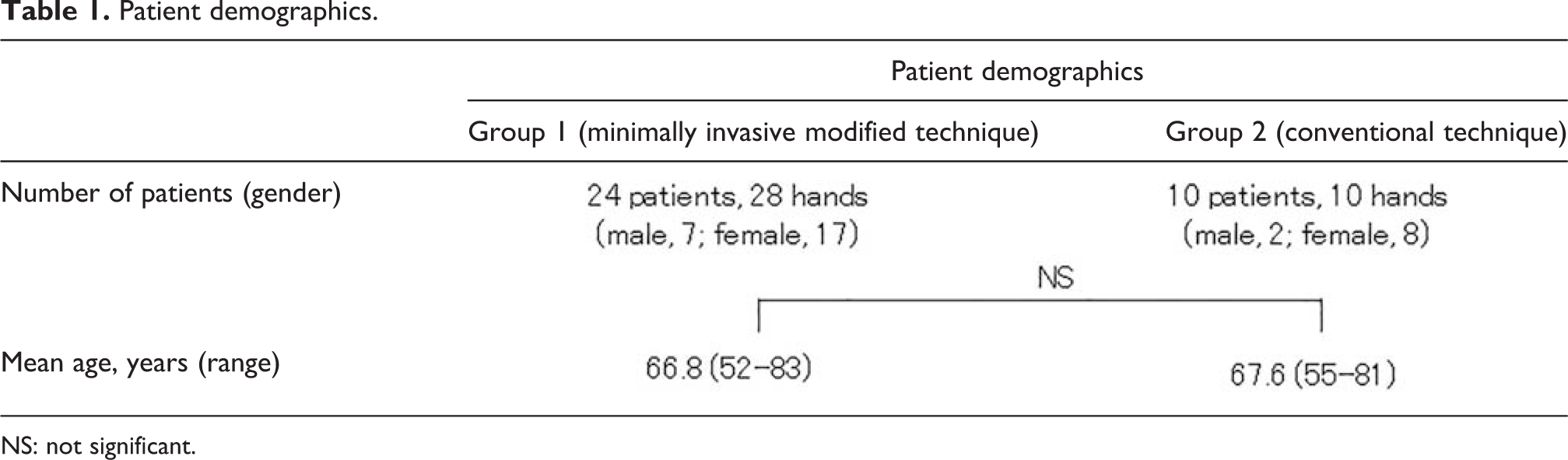
NS: not significant.
This procedure is not recommended for patients with osteoarthritis of the thumb carpometacarpal joint because it may worsen the symptoms. They are also contraindicated for patients performed suspensionplasty using the palmar approach, because the overlying skin is usually scarred.
Surgical technique
Before surgery, the presence of the PL tendon is confirmed by the active maneuver of opposing the thumb to the little finger with the wrist slightly flexed.
All surgeries were performed under general anesthesia. Patients in group 1 underwent the minimally invasive modified Camitz opponesplasty. A 5 cm curved skin incision (2.5 cm both distally and proximally extending from Kaplan’s cardinal line) along the proximal palmar crease is made without crossing the distal wrist crease (Figure 1). A 2 cm strip of the palmar aponeurosis together with the PL tendon is dissected and harvested to maintain the maximal length to allow transfer (Figure 2(a) and (b)). Care is taken to preserve the palmar cutaneous branch of the median nerve, which situates radial to the PL tendon. An adequate length of palmar aponeurosis must be harvested so that the transferred tendon reaches the insertion point of the APB. The transverse carpal ligament is continuously released to decompress the median nerve in the carpal tunnel. No pulley is made on the transverse carpal ligament. A second small longitudinal incision is then made on the radial side of the thumb at the level of the metacarpophalangeal (MP) joint to expose the tendinous insertion of the APB. Lastly, the PL tendon strip is passed under the fascia of the APB to prevent the bowstringing of tendon and sutured to the insertion of the APB with the thumb in full opposition during maximum tension in maximal palmar abduction of the thumb (Figure 3(a) and (b)).
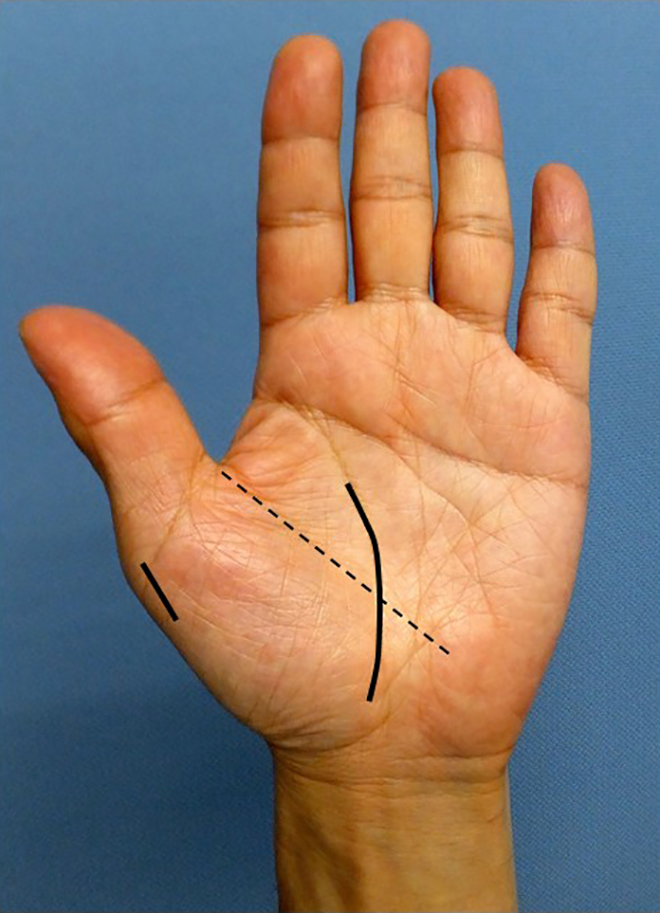
Surgical skin incision length of the minimally invasive modified Camitz opponensplasty (group 1). Long solid line: palmar incision, short solid line: thumb incision, dotted line: Kaplan’s line.
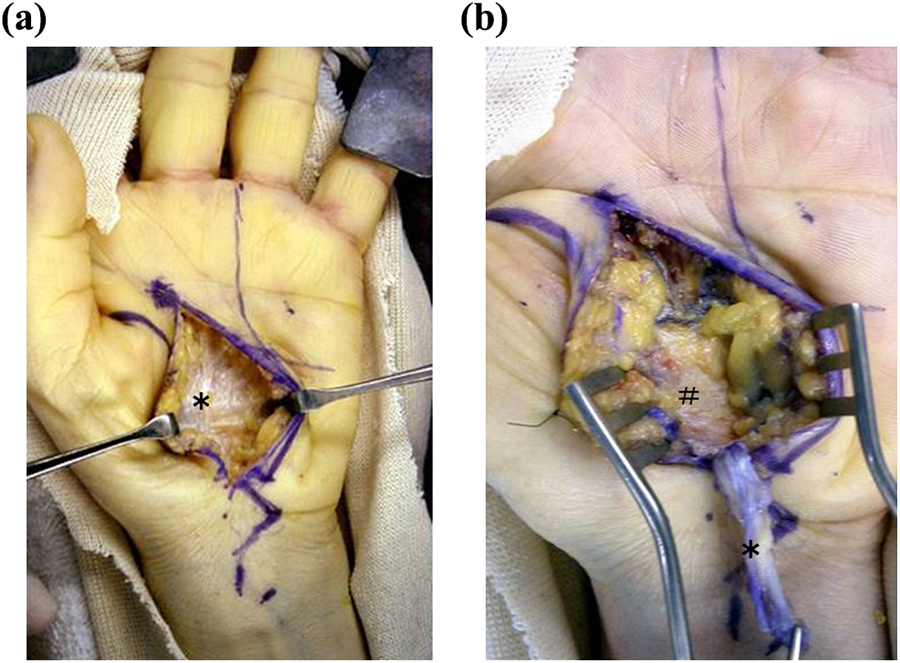
Intraoperative photograph of the minimally invasive modified Camitz opponensplasty (group 1). (a) Dissection of the subcutaneous soft tissue after a palm skin incision and (b) harvest of a strip of palmar aponeurosis continued with the PL tendon. *: palmar aponeurosis, #: transverse carpal ligament.

Surgical procedure of the minimally invasive modified Camitz opponensplasty (group 1). (a) Passing the PL strip under the fascia of the APB as prevention for tendon bowstringing after decompression of the median nerve in the carpal tunnel and (b) Suture the PL strip to the insertion of the APB with the thumb. PL: palmaris longus; APB: abductor pollicis brevis.
Conversely, patients in group 2 underwent the conventional Camitz opponesplasty. A skin incision continued from proximal to distal palm crease to approximately 2–4 cm proximal to the wrist proximal crease along the proximal palmar crease is made with crossing the distal wrist crease (Figure 4). A 2 cm strip of the palmar aponeurosis together with the PL tendon is dissected and harvested to maintain the maximal length to allow transfer. The transverse carpal ligament is continuously released to decompress the median nerve in the carpal tunnel. No pulley is made on the transverse carpal ligament. A second small longitudinal incision is then made on the radial side of the thumb at the level of the MP joint to expose the tendinous insertion of the APB. Lastly, the PL tendon strip is transferred under the skin, without passing under the fascia of the APB and sutured to the insertion of the APB with the thumb in full opposition during maximum tension in maximal palmar abduction of the thumb.

Surgical skin incision length of the conventional Camitz opponensplasty (group 2). Long solid line: palmar and wrist incisions, short solid line: thumb incision, dotted line: Kaplan’s line.
In all patients, a short arm thumb spica splint is then applied to immobilize the thumb in maximum palmar and radial abductions with the wrist in neutral position for 3 weeks after surgery. After the splint is removed, the thumb range of motion exercise is started.
We retrospectively evaluated the clinical results before and after surgery as follows.
The clinical results obtained before surgery and more than 12 months after surgery were evaluated and classified into four categories according to the relief of symptoms in accordance with Kelly et al. 22 Excellent was complete relief of symptoms, good meant persistence of occasional minor symptoms, fair meant some constant or annoying symptoms, and poor meant symptoms unchanged or worse.
Moreover, the angle of the thumb palmar abduction and the pinch power were examined before surgery and more than 12 months after surgery using a pinch meter. Additionally, the Kapandji score 23 was used to measure the degree of active thumb opposition. It was charted from 0 to 10 by asking the patient to oppose the thumb tip to the distal, middle, and proximal phalanx of other fingers. Furthermore, the clinical results obtained before surgery and more than 12 months after surgery were evaluated according to Foucher’s evaluation. 2 Foucher et al. evaluated the clinical results as good when the distance between the thumb tip and the palm in the thumb palmar abduction, the angle of the thumb palmar abduction, and the Kapandji score were all over 80% of the unaffected side. 2
All analyses were performed with the software program IBM SPSS Statistics 21.0 J (IBM Japan Ltd., Tokyo, Japan). The angle of the thumb palmar abduction, the pinch power, and grip strength were statistically analyzed before and after surgery using the Student’s paired t test. Moreover, they were compared between group 1 and 2 using the unpaired Student’s t test. A p value of less than 0.05 was considered statistically significant.
Results
According to Visser’s classification of clinical severity of CTS, 24 before surgery, all hands had severe lesions with sensory loss and severe muscle weakness (less than grade 4 on the Medical Research Council scale) or atrophy of the APB or opponens pollicis. In group 1, after surgery, 4 hands were normal with no sensory disorders, 24 hands had mild lesions with only sensory disorders, no hands had moderate lesions with sensory loss and weakness of APB or opponens pollicis, and no hands had severe lesions. In group 2, after surgery, two hands were normal, eight hands had mild lesions, and no hands had moderate or severe lesions.
The clinical results obtained after surgery were evaluated and classified into four categories according to the relief of symptoms in accordance with Kelly et al. 22 Excellent was complete relief of symptoms, good meant persistence of occasional minor symptoms, fair meant some constant or annoying symptoms, and poor meant symptoms unchanged or worse. In group 1, the clinical results were excellent in 4 hands (14.3%), good in 21 hands (75.0%), fair in 3 hands (10.7%), and poor in no hands after surgery. The clinical results in group 2 were excellent in one hand (10.0%), good in seven hands (70.0%), fair in two hands (20.0%), and poor in no hands after surgery.
Moreover, the angle of the thumb palmar abduction, pinch power, and grasp strength markedly improved from 30.2°, 3.41 kg, and 10.4 kg to 57.4°, 5.82 kg, and 15.2 kg, respectively, after surgery compared with before surgery in group 1 (Tables 2 to 4). There were statistically significant differences in the angle of the thumb palmar abduction, the pinch power, and grasp strength between before and after surgery, respectively, (p < 0.01; Tables 2 to 4). The Kapandji score 23 also significantly improved from 2.6 to 8.6 after surgery compared with before surgery in group 1. According to Foucher’s evaluation, 2 all hands were evaluated as good after surgery. Conversely, the angle of the thumb palmar abduction, pinch power, and grasp strength markedly improved from 28.9°, 3.62 kg, and 11.7 kg to 52.5°, 5.47 kg, and 14.1 kg, respectively, after surgery compared with before surgery in group 2 (Figure 5 and Tables 2 to 4). There were statistically significant differences in the angle of the thumb palmar abduction, the pinch power, and grasp strength between before and after surgery, respectively, (p < 0.01; Tables 2 to 4). The Kapandji score 25 also significantly improved from 3.6 to 8.0 after surgery compared with before surgery in group 2.
Comparison of clinical results of both the thumb palmar abduction angle before and after surgery in group 1 and 2.

NS: not significant.
a p < 0.01.
Comparisons of clinical results of pinch power before and after surgery in group 1 and 2.
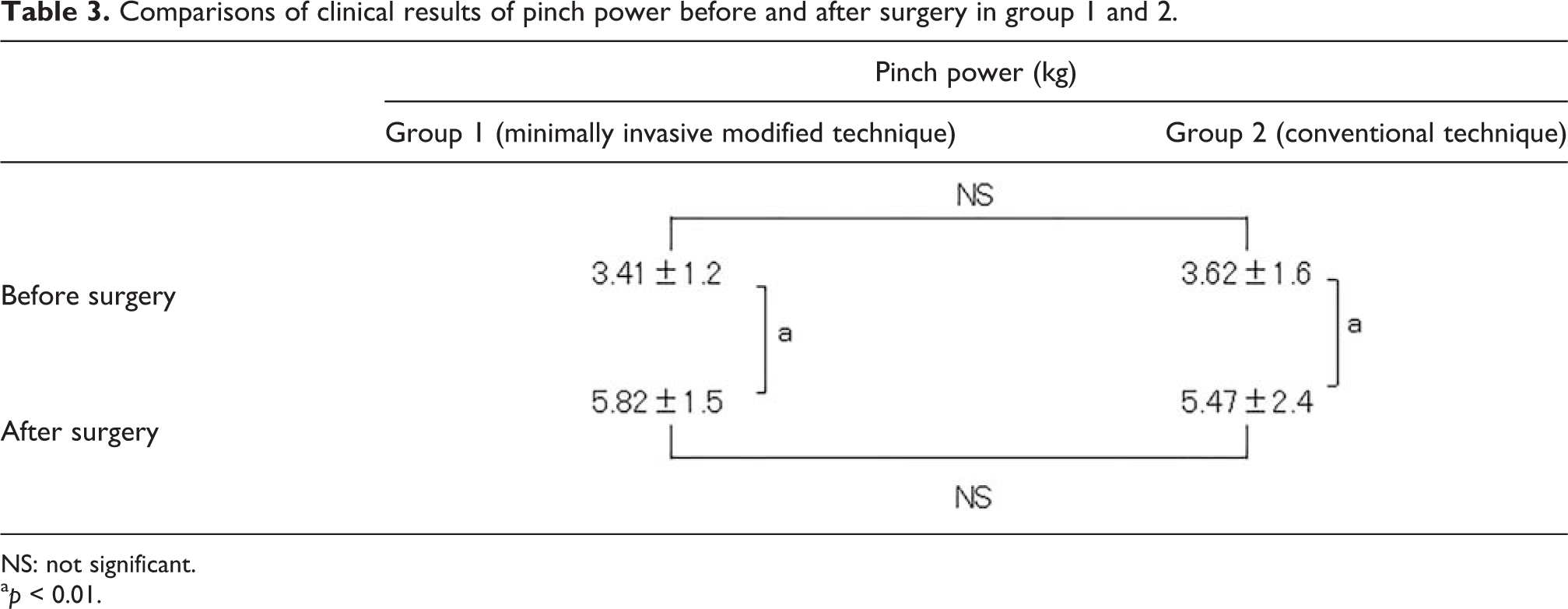
NS: not significant.
a p < 0.01.
Comparisons of clinical results of grasp strength before and after surgery in group 1 and 2.

NS: not significant.
a p < 0.01.

Maximum thumb palmar abduction in a representative case, (a) Before surgery and (b) After surgery.
Furthermore, there were no complications including infection, painful wrist scar, or injury to the palmar cutaneous branch of the median nerve in group 1. On the other hand, patients in group 2 had no infection, four painful wrist scars, one injury to the palmar cutaneous branch of the median nerve, and nine bowstrings of the transferred tendon. Bowstring of the transferred tendon, which occurs frequently and prominently in the conventional Camitz procedure, was not observed in group 1. All patients in group 1 were satisfied with their results including the cosmetic outcome. The frequency of the complications after surgery in group 2 was significantly higher compared to group 1. However, there was also no recurrence of the loss of thumb opposition with its useful recovery in all hands after surgery.
Discussion
For patients with advanced CTS with thenar muscle atrophy, carpal tunnel release alone is considered to obtain poor response and require long-term nerve recovery. 1 –12 However, the indication of concurrent opposition transfer with carpal tunnel release for severe CTS has remained controversial. 3,5,9
Some authors have reported that relatively good results can be achieved after carpal tunnel release alone and have not recommended concurrent opposition transfer. 25,26 Park and Kim also reported that clinical recovery of thenar muscle atrophy was obtained in more than 95% of cases 6 months after carpal tunnel release. 26
Conversely, many articles have reported that recovery of the thumb opposition by carpal tunnel release alone may not be expected sufficiently in patients with severe CTS, especially elderly patients. 1 –12 Littler and Li have reported that recovery of thenar muscle atrophy could not be predicted even after carpal tunnel release. 6 Similarly, Thurston and Lam described that only around 50% of cases improved greatly or returned to normal daily activities after carpal tunnel release alone. 27 Especially, they related that the majority (86%) of cases did not recover thenar muscle bulk. 27 Moreover, several reports related that after carpal tunnel release alone, return of the thumb opposition took many months to years, and satisfactory outcomes were unlikely, particularly in elderly CTS patients with severe thenar muscle atrophy. 2,3,9
Therefore, a single-stage procedure, combining opponesplasty and carpal tunnel release has been recommended as the most reliable treatment method for the loss of thumb opposition in patients with severe CTS. 2,3,7
Currently, many opponespalsty procedures have been reported to restore thumb opposition using flexor pollicis longus, 18 flexor digitorum superficialis, 13 extensor carpi ulnaris, 16 extensor digiti minimi, 17 extensor indicis proprius, 14 or PL. 15
Among these opponesplasties, the Camitz opponespalsty using PL is the most frequently used tendon transfer for advanced CTS patients with significant loss of thumb opposition. 2 –12,15 Presently, the Camitz opponespalsty, which transfers the PL continued with a strip of palmar aponeurosis to the insertion of the APB, is a standard procedure with simultaneous carpal tunnel release. 2 –12
Several authors have reported good clinical results with the Camitz opponesplasty. 2 –12 Terrono et al. reported 94% patient satisfaction in thumb function improvements with the Camitz opponensplasty. 11 Similarly, Kang et al. demonstrated an average score of 92.4% improvement in Kapandji tip opposition compared with the unaffected side. 4 Foucher et al. reported that Camitz opponensplasty with simultaneous carpal tunnel release afforded 90.7% good results for a long time. 2 Hattori et al. described that the recovery of the thumb opposition function at the first 3 months after surgery depended only on the transferred tendon in most patients. 3
In the current study, both the minimally invasive modified Camitz opponensplasty combined with open carpal tunnel release and the conventional Camitz opponespalsty were performed for all severe patients with higher functional demands requiring early opposition recovery for work or activities of daily living. Subsequently, the angle of the thumb palmar abduction, the pinch power, grip strength, and the Kapandji score significantly improved after surgery compared with before surgery. These results were similar to those of abovementioned reports.
As advantages of the Camitz opponensplasty over other procedures, the PL used as a transferred tendon can be harvested without obvious functional deficit. 1,5,8 –10 The PL muscle works in cooperation with the APB, meaning no specific rehabilitation is required after surgery, 2,5,8 and its substantial length enables attachment to the ideal APB insertion. 2,5,12 Moreover, this procedure can be easily accomplished through the same skin incision as that used for the carpal tunnel release. 1,5,9 Additionally, in this Camitz opponensplasty, the transferred tendon does not disturb the original physiological movement of the thumb including the opposition movement even after the recovery of the thenar muscle atrophy postoperatively. 7 Therefore, the procedure plays a role in maintaining the thumb opposition until the recovery of thenar muscle strength as an “internal splint” in those who subsequently recovered at an early stage. 7
However, there have been reported some disadvantages with the conventional Camitz opponespalsty. The conventional Camitz procedure requires a large longitudinal incision beginning from proximal to the distal palmar crease and extending proximally beyond the proximal wrist crease in line with the ring finger. 2 –4,6 –12 Several complications have been considered to attribute to this large incision in the palm and wrist. 1,3,10,11,19 This procedure involves extensive soft tissue dissection increasing the risk of iatrogenic injury to the palmar cutaneous branch of the median nerve 1 –3,9 –11,19 and a painful scar on the wrist. Some authors reported that the incidence of the painful scar on the extended incision straddling the wrist crease in this procedure ranges from 19% to 61%. 28,29 This lengthier incision may increase painful scar, compared with a minimally invasive procedure. 30,31 In the current study, there were four painful wrist scars in group 2. Recently, to address this shortcoming in the conventional Camitz procedure (group 2), a minimally invasive palmar incision with no incision to the wrist crease or the forearm (group 1) has been used.
Moreover, the prominent bowstringing of the transferred tendon has been widely noted as one of the main shortcomings. 1 –3,5,10,19 Foucher et al. reported that most of the insufficient results were loss of mechanical advantage of the transfer due to bowstringing at wrist level. 2 In this study, there were nine bowstrings of the transferred tendon in group 2. We assumed that this shortcoming occurred because the transferred tendon shifts too radially of the wrist under the skin. In the current study, this problem was overcome by passing the transferred tendon under the APB fascia using the small palmar incision without straddling the wrist crease in group 1.
There has been reported absence of the PL in approximately 15% of hands of the normal population. 2,8,12 In such cases, other opponensplasties other than the Camitz method should be considered. Accordingly, a preoperative evaluation to confirm the presence of the PL is required.
In addition, the movement of the thumb opposition has been considered as a combination consisted of palmar abduction, pronation, and adduction. 2,8,12 The conventional Camitz opponensplasty is beneficial for palmar abduction, and brings the elevation of the thumb metacarpal in a plane that is perpendicular to the palm. 5,9,11,12 Conversely, this opponesplasty supplies little benefit to thumb flexion and pronation 4,5,7,9,11 because of the inadequate line of pulling of the transferred tendon, and does not completely replace the complex function of accurate opposition of the thumb 5,9,11,12 . For improvement of this weakness, some authors 3 –5,9 reported the modifications of Camitz opponensplasty using flexor retinaculum as a pulley to further improve the thumb opposition. They described that various ways of using different additional pulleys to improve the line of pull of transferred PL tendon shifted too radial to ideal axis for opposition. 3 –5,9 In the current study, the modified procedure by passing the transferred tendon under the APB fascia without a pulley was performed to prevent the transferred tendon both shifting radial to the ideal axis for opposition and bowstringing. Consequently, the mean Kapandji score significantly improved after surgery compared with before surgery. All patients were satisfied with the restoration of the thumb opposition and cosmetic outcome.
Furthermore, various techniques regarding the attachment of transferred tendon to the thumb have been reported to restore the thumb opposition more precisely. Riordan 32 and Tsuge 33 attached transferred tendon to extensor pollicis longus on the thumb MP joint, Bunnel 13 attached transferred tendon to the dorsoulnar side of the base of the thumb proximal phalanx, and Brand 34 attached transferred tendon to the ulnar side of the thumb MP joint. However, it is difficult to restore thumb opposition precisely in any procedure. Therefore, in this study, the transferred PL tendon was attached only to the insertion of the APB without suturing to the radial side of the thumb. Subsequently, not only the harvested palmar aponeurosis could be shorter but also the incision could be smaller than the conventional Camitz procedure.
This study had several limitations. First, our study had a relatively small patient group. A larger group of patients may provide more detailed conclusions to our findings. Second, the data of this study was collected in a retrospective manner. Finally, a weakness of this study was that there is a lack of long-term studies comparing the clinical results of the current modified Camitz procedure with those of the conventional one. Future researches will address the long-term comparison between these two procedures in severe CTS patients with thenar muscle atrophy.
Conclusions
The current study demonstrated good clinical results of a modified Camitz opponensplasty combined with open carpal tunnel release in severe CTS patients with thenar muscle atrophy. Especially, this modified Camitz opponensplasty using a minimally invasive incision without straddling the wrist crease was a simple and effective procedure that could decrease the risk of damage to the palmar cutaneous branch of the median nerve and prevent painful scar around the wrist crease. Additionally, this technique by passing the transferred PL tendon under the APB fascia can be useful not only to provide immediate significant improvement of thumb opposition function but also to prevent the bowstringing of the transferred PL.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.