
Abstract
BACKGROUND:
Plank exercise is one of the most popular methods of exercise for strengthening the trunk muscles. However, many individuals might have some difficulty performing this exercise.
OBJECTIVE:
This study aimed to identify trunk muscle activation with postural changes and the use of dynamic cushion during a traditional plank exercise in order to propose a set of exercise levels according to exercise performance ability.
METHODS:
Seven participants were asked to perform the traditional plank exercise (TPE), a modified plank exercise (MPE), an unstable traditional plank exercise (UTPE), and an unstable modified plank exercise (UMPE). The UTPE and UMPE use a dynamic cushion to simulate an unstable surface. Surface EMG of the ractus abdominis (RA), external oblique (EO) and erector spinae (ES) was recorded while participants were engaged in these exercises. The plank exercises were performed for ten seconds with a ten-minute break between each posture.
RESULTS:
Comparing the measurement results from the four postures, significant differences were observed in the RA and EO (
CONCLUSION:
The results of this study may be used as a basis to arrange the order of exercise, based on the level of muscle activation appropriate for the participant’s exercising ability. Individuals who have difficulty performing the TPE, may first perform the MPE and the UMPE.
Introduction
“Core” is a term that refers to the muscles located in the pelvic area and the trunk that provide stability to the spinal column [1, 2]. The core muscles deliver force across extremities during physical movement as well as play an important role in resisting perturbations in the spine. Rehabilitation exercises, such as the coordinative exercise, strengthening of the core muscles aimed at building an ideal abdominal wall, drastically reduces the incidence of low back injuries and improves exercise performance and trunk stability [3, 4].
Common methods of strengthening the core muscles include neuromuscular electrical stimulation and spinal column stability training [5, 6]. Neuromuscular electrical stimulation is a method used for producing contraction in the muscles involved in lumbar stabilization. Spinal column stability training is a representative core strengthening method that is becoming widely used in personal sports activity, rehabilitation, and general fitness owing to its strong necessity. In particular, core-strengthening exercise is preferred to prevent injuries that can occur while performing certain movements in various sports [6]. Researchers have noted in previous studies that irritation or injuries of the spine tissue can occur from everyday strenuous work [7]. Therefore, in order to prevent these injuries, it is important to stabilize the trunk through core strengthening exercise [7]. In addition, improved trunk stability through spinal column stabilization training not only has a positive effect on activities of daily living, but also lead to the alleviation of low back pain [8], improvement in leg function after total hip replacement or total knee replacement [9], and overall performance improvement among athletes [10].
Among the various spinal column stabilization-training exercises, sit-ups, crunches, and planks effectively strengthen the core muscles without time and space restrictions. Traditional plank exercises (TPE), in particular, are known to effectively enhance the strength and endurance of the core muscle tissue for the purpose of muscle strengthening and rehabilitation [7]. In addition, devices producing body instability such as Swiss Ball, TRX, and BOSU Ball are being adopted in recent core muscle strengthening exercises [11, 12]. The benefit of using these devices is that they require greater muscle activation to maintain postural balance control [11]. Ronald et al., confirmed that compared to the traditional method of TPE, TPE performed on an unstable surface using Swiss Ball and TRX revealed greater and more significant electromyography measurements. Thus, the study suggested that people who intend to experience greater muscle activation could use instability devices as a progressive muscle strengthening method [13]. However, the study failed to propose a progressive exercise protocol that allows people with different physical levels easy access to TPE. In addition, in previous studies, the effects of TPE were reported; however, to the best of our knowledge, no study to date has identified muscle activation with postural changes. Thus, the purpose of this study was to identify trunk muscle activation with postural changes and the use of dynamic cushion during TPE in order to propose a set of exercise levels that are applicable to a wide population.
Methods
Participants
This was a cross-sectional study. The purpose and methods of the study were posted in the school bulletin to recruit potential participants. Twenty volunteers were recruited and screened according to the following criteria: healthy adults between 20 and 29 old ages (with no resistance exercise experience within 6 months), absence of back or lower extremity problems such as spinal disk herniation, no history of previous spine operations, and the ability to maintain a seated posture for one minute or longer. Volunteers with congenital back deformities or orthopedic or neurological problems were excluded. In total, 13 volunteers were excluded and seven individuals participated in the study. There were 6 males and 1 female participants with an average age of 226 (2.23) years, weight 68.3 (12.23) kg, height 174.6 (7.53) cm.
All participants provided signed informed consent after receiving an explanation of the study purpose and procedures. The study was approved by the Kyungnam University Institutional Review Board.
Procedure
General characteristics (sex, age, weight, and height) of the participants were collected through a brief interview Trunk muscle activity was measured using surface electromyography (sEMG). Maximal voluntary isometric contraction (MVIC) was recorded for four muscles; the external oblique (EO), rectus abdominis (RA), and erector spinae muscles (ES) on both sides of the body. Recording electrode locations were based on the SENIAM recommendations [14]. Electrode pads were attached approximately 3 cm above the iliac crest for EO, 3 cm lateral to the navel for RA, and 5 cm lateral to L4 for ES. Skin regions were shaved and cleaned with alcohol swabs before attachment. Activity of each muscle was collected for 10 seconds, in three trials, with a two-minute break between trials. MVIC was calculated based on 5 seconds of collected data (between 3 and 8 seconds). After a 10 minute break, trunk muscle activities of the EO, RA, and ES on both sides of the body were collected in four postures. The participants were instructed to assume the four positions in any order. Each posture was maintained for 10 seconds, and 10 minute break was given between postures to reduce the influence of the preceding posture on muscle activity. The participants had rest periods with their comfortable posture such as lying down. sEMG signals in each muscle were collected for 10 seconds while maintaining each posture. The data was collected as the mean of the 3rd and 8th second for each posture and then used for statistical comparisons.
Plank exercise
TPE [15] was performed for 10 seconds by maintaining a push-up posture with the elbows bent at 90
The unstable plank exercise (UTPE) was performed for 10 seconds, following the same posture of the basic TPE but with a 33 cm diameter dynamic cushion placed under the elbows and the toes [16] (Fig. 1A and B).
The Modified plank exercise (MPE) was performed for 10 seconds modifying the basic TPE posture by placing the knees on the ground and lifting up the toes from the ground [17]. Unstable modified plank exercise (UMPE) was performed for 10 seconds following the MPE posture but with a dynamic cushion placed under the elbows and the knees [18] (Fig. 1C and D).
Electromyography
The sEMG (Tringo™ Wireless, Delsys, USA) was used to record the activities of the EO, RA, and ES. Data were processed using standard filtering and rectifying methods. The sampling rate was 2000 Hz, and a 60 Hz high-pass filter and a 10 Hz low-pass filter were applied (all filters, zero-lag 4th order Butterworth). For normalization of the data, the root mean square (RMS) value of the raw EMG data was calculated. The EMG data of each muscle was normalized by calculating the RMS of the five seconds MVIC of the muscle. The EMG data as the mean of the 3rd and 8th second collected during the sitting postures were also normalized by calculating the RMS, and then expressed as a percentage of the MVIC value.
A traditional plank exercise (A), an unstable plank exercise (B), a modified plank exercise (C), and an unstable modified plank exercise (D).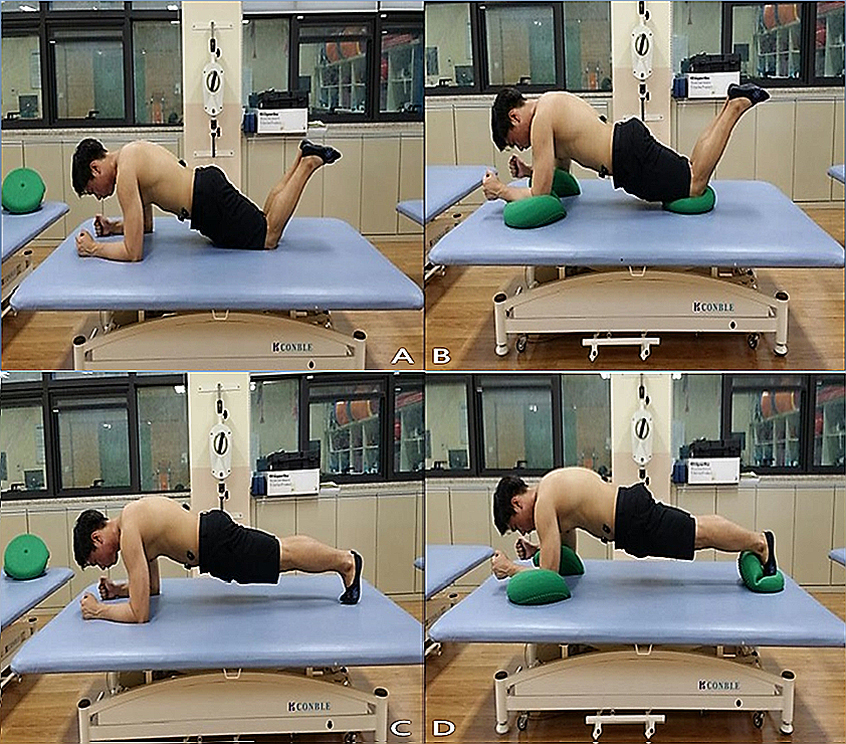
For the statistical analysis we used the SPSS 18.0 software (SPSS, Inc., USA). The general characteristics of the participants were analyzed using descriptive statistics. One-way analysis of variance was used to compare trunk muscle activities between the four different postures, and Tukey’s post-hoc test was conducted. The level of statistical significance was set at
The muscle activity of the trunk muscle according to the four exercise (% MVIC)
The muscle activity of the trunk muscle according to the four exercise (% MVIC)
Values are shown as mean (standard deviation). Significant differences between TPE and MPE were presented as
Comparison of the results from four postures revealed significant differences in the RA and EO (
Discussion
In the present study, muscle activation from UTPE indicated significant difference in RA and EO (
Lehman et al. [19] conducted a study examining the difference of trunk muscle activation during TPE depending on the use of stability ball. The study results indicated greater muscle activation in RA and EO among the research participants who used an instability device [19]. Ronald et al. also conducted a study on the trunk muscle activation comparing the use of different types of instability devices such as Swiss Ball and TRX, and conclusively reported that trunk muscle activation differs according to the type of instability device [13]. However, when the group that performed TPE on a stable surface was compared to the group that performed the exercise using an instability device, higher muscle activation in RA, EO, and ES was observed in the latter group. On the contrary, the results from the present study reveal the highest muscle activation from UTPE in RA and EO, although the difference was not statistically significant when compared to other types of exercises.
In a study by Czaprowski et al. [16], trunk muscle activation during TPE under three different conditions – a stable surface, BOSU Ball, and Swiss Ball – were compared. The highest muscle activation was observed during TPE using the Swiss Ball when compared to TPE on a stable surface and TPE using a BOSU ball. However, no significant difference was observed when the muscle activation was compared between the group that performed the exercise on a stable surface and the group that performed the exercise using the BOSU Ball. This result corroborates with the data from the present study, which also revealed that there is no significant difference in trunk muscle activation between TPE on a stable surface and TPE on a dynamic cushion. A conceivable explanation for this result obtained in the current study is that the dynamic cushion used in the study was limited in providing sufficient instability.
In the present study, significant difference in trunk muscle activation was observed from UTPE than from MPE and UMPE (
In terms of limitations to the study, worth noting is that in spite of proper preparation for recording the EMG a 10–15% margin of error can occur as in every EMG study. In addition, the number of the participants was too small to generalize the study results, and the muscle activation measurements were restricted to the RA, EO, and ES to the exclusion of the other trunk muscles. Thus, a future study should be conducted with large numbers of participants, and the trunk muscles and the effects of various deep muscles should be considered as well. Furthermore, to present a more effective level of exercise, a highquality clinical study applying the plank after classifying participants according to exercise performance ability is required
In conclusion, the present study aimed to identify trunk muscle activation with postural changes and the use of dynamic cushion during a traditional plank exercise Through this study, it was found that muscle activations in the RA and EO during performance of UTPE were greater than in MPE and UMPE. The results may be used as a basis to arrange the order of exercise, based on the level of muscle activation appropriate for the participant’s exercising ability. MPE may be recommended to people who are new to TPE or have trouble performing TPE the right way as well as to those who have difficulty performing the TPE due to muscle weakness. If such individuals can perform MPE with correct posture and by using the correct muscles, they should be able to perform the TPE as the next step. In the meantime, an element of instability may be incorporated into the exercise by using a dynamic cushion in areas such as the toes or the elbows in order to provide the individual with a greater challenge.
Conflict of interest
The authors declare no conflict of interest.