
Abstract
BACKGROUND:
There are controversies regarding the optimal number of trials and intervals during required for testing of maximal handgrip strength.
OBJECTIVES:
To verify the minimum optimal number of trials (two versus three consecutive trials) and inter-effort interval (15, 30, 45 and 60-s) during the measurement of maximal handgrip strength.
METHODS:
One hundred healthy subjects, 51 males and 49 females, were enrolled. During the measurement of maximal handgrip strength, two consecutive trials were hypothesized to be the minimum necessary. We compared the maximal handgrip strengths between two and three consecutive trials at four different intervals (15, 30, 45, and 60-s).
RESULTS:
Irrespective of hand dominance, maximal handgrip strength was best measured with three consecutive trials rather than two at each interval (all
CONCLUSIONS:
Three consecutive trials with a 60-s interval might be the minimum needed for optimal measurement of maximal handgrip strength.
Introduction
Maximal handgrip strength is the maximal static strength generated by the proximal and middle phalanges of the hands [1]. It has been accepted as a reflection of general muscle strength as well as upper extremity strength and is used as a parameter reflecting general health [2, 3, 4]. Sarcopenia can be easily diagnosed with the measurement of handgrip strength [5]. It can also be a predictor of mortality, fragility, risk of falls and functional decline [6, 7, 8, 9, 10]. It can also be used as an indicator of disease activity in rheumatoid arthritis patients and as a nutritional index [11].
Due to the above characteristics of handgrip strength, some large-scale epidemiologic studies have investigated the measurement of handgrip strength [12, 13, 14]. However, handgrip strength is affected by several factors and measurement reliability could be a matter of concern. The handle position of the dynamometer [15], upper body posture [16], grip span [17], the amount of verbal instructions given by the examiner [18], time of day and muscle warm-up [19] are considered to influence test results. Also, the number and interval between trials might affect the results of handgrip strength, especially in a large-scale epidemiologic study due to the burden on examiners. After the American Society of Hand Therapists (ASHT) introduced the widely accepted concept of repetition and interval between trials, i.e. three trials with a 60-s interval, several literatures on hand grip strength have adopted this method [20, 21, 22, 23]. However, several epidemiologic studies have been performed with fewer than three trials and a less than the 60-s interval [24, 25, 26].
To reduce the burden of epidemiologic studies, we hypothesized that less than three consecutive trials with a less than 60-s interval might be appropriate and acceptable. Thus, the aim of this study was to identify the minimum optimal number of grip trials and the interval between each during the measurement of maximal handgrip strength. To this end, we compared maximal handgrip strength obtained in two compared to three consecutive trials.
Method
This study was approved by the Institutional Review Board of Myongji Hospital, and all subjects signed written informed consent before participating in the study.
Subjects
A total of 107 subjects (52 males [height; mean 169.4 (SD 8.5), weight; mean 64.1 (SD 11.8)], 55 Females [height; mean 159.6 (SD 7.6), weight; mean 57.1 (SD 9.1)], mean age: 31.9 years, range 23–49 years), medical personnel, were assessed for their eligibility for inclusion in this study. Every subject in this study was involved in a medium level of occupational demand according to the five categories of the Dictionary of Occupational Titles which are sedentary, light, medium, heavy and very heavy [27]. Exclusion criteria were osteoarthritis, rheumatoid arthritis (
The pathway to determine the minimum optimal number of trials and interval.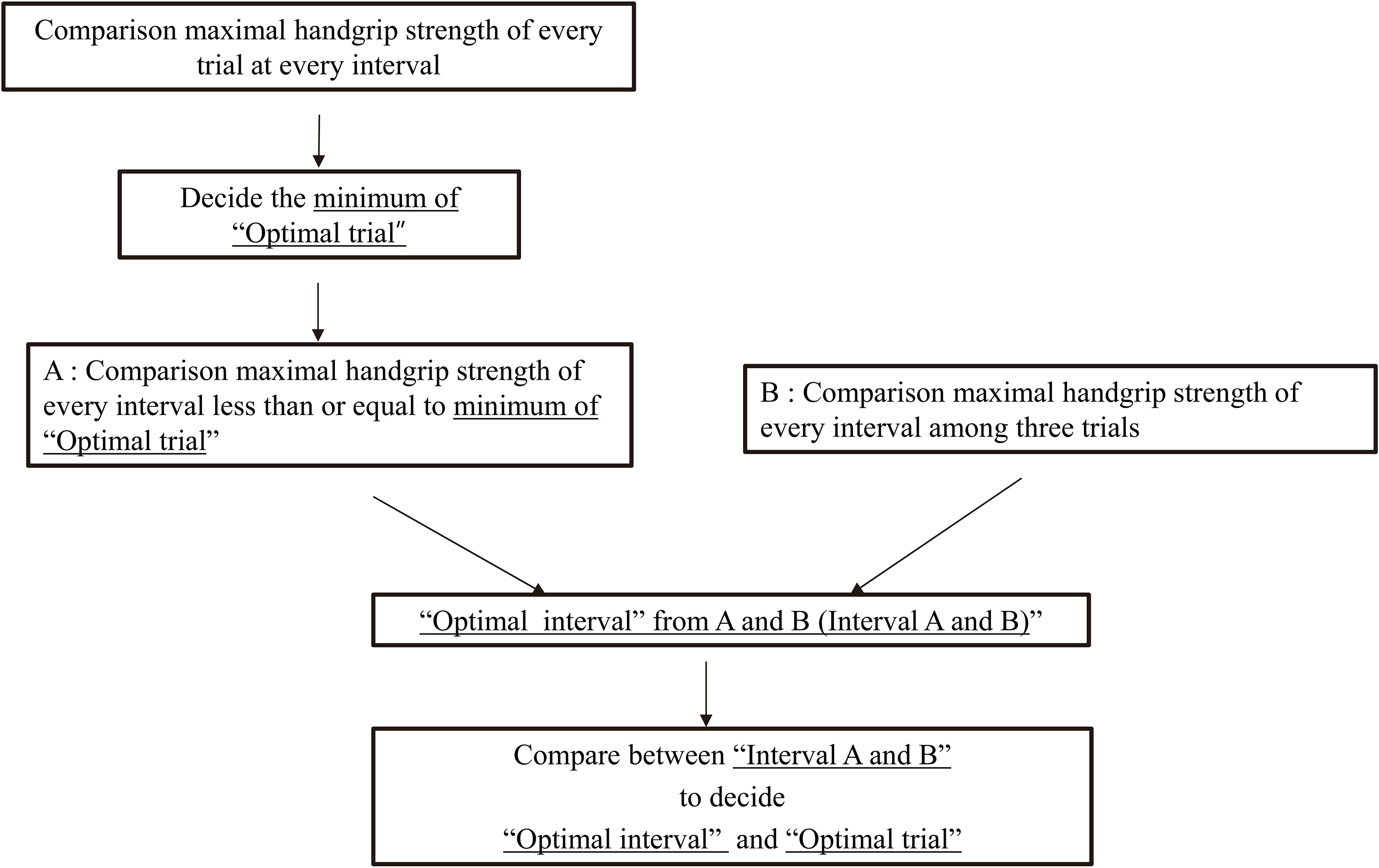
Comparison of maximal hand grip strength between two consecutive and three consecutive trials at each interval (15, 30, 45, and 60-s) in the dominant hand.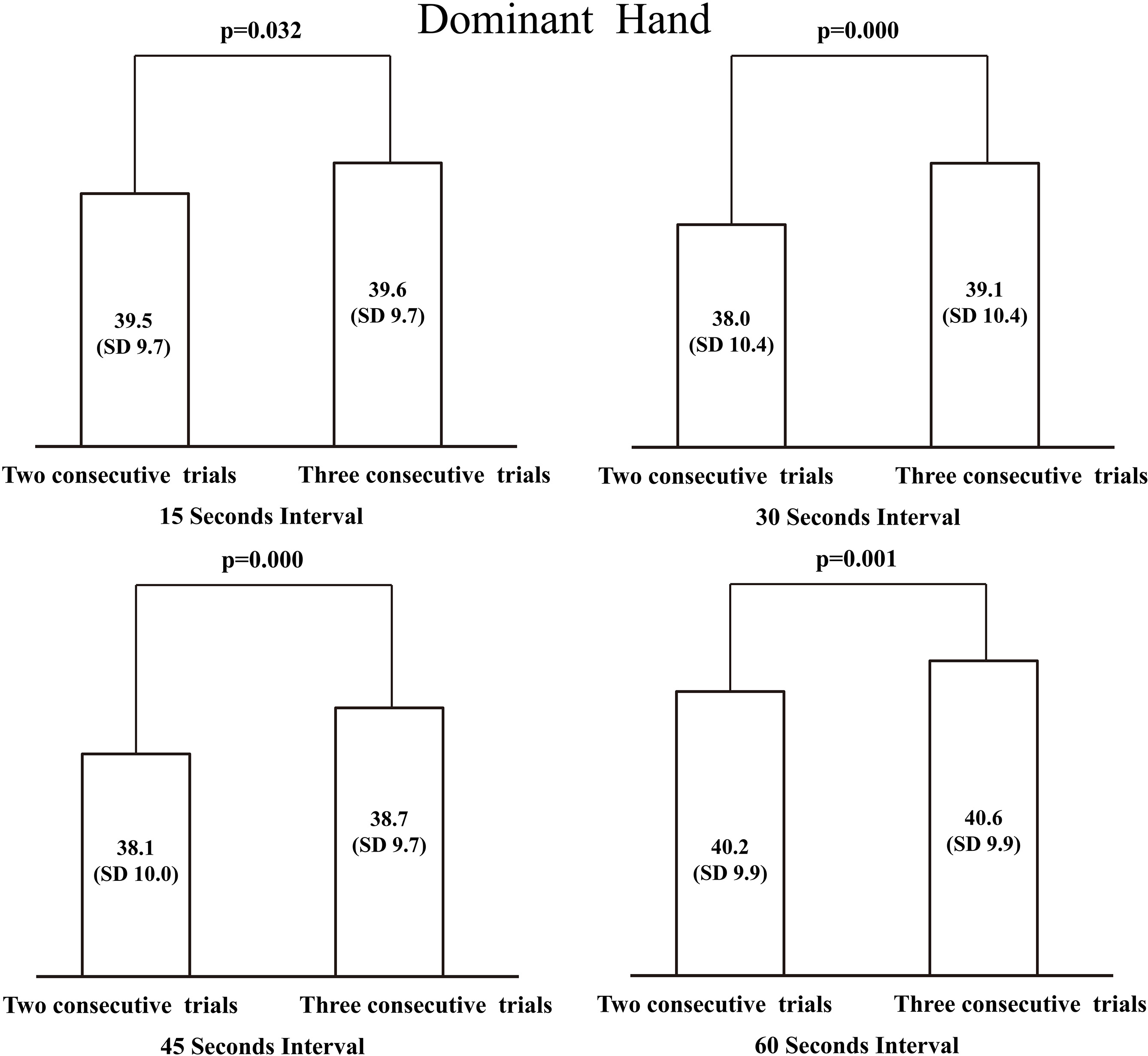
Maximal handgrip strength was measured with a Takei digital handgrip dynamometer (Takei T.K.K 5401, Takei Scientific Instruments Co. Ltd. Niigata, Japan). The reliability of the Takei dynamometer has been demonstrated previously [28, 29]. Handgrip strength was recorded in kilograms (kgf). The handgrip span on the dynamometer was adjusted according to each subject’s hand span, which ranged from 6 to 8 cm during the measurements. The subject was seated on a chair and the position of the upper extremity to be assessed was as follows: the shoulder was in adduction, the elbow was flexed to 90 degrees, the forearm was in neutral supination/pronation, and the wrist was in neutral to 30 degrees of volar flexion as well as in zero to 30 degrees of ulnar deviation. Subjects were instructed to maintain voluntary grip for 4 seconds. Therefore, the nature of grip strength in this study was considered to be static rather than dynamic.
Maximal handgrip strength for the minimum optimal number of trials (three consecutive trials) at 60-s compared to other intervals (15, 30 and 45-s intervals) in the dominant hand.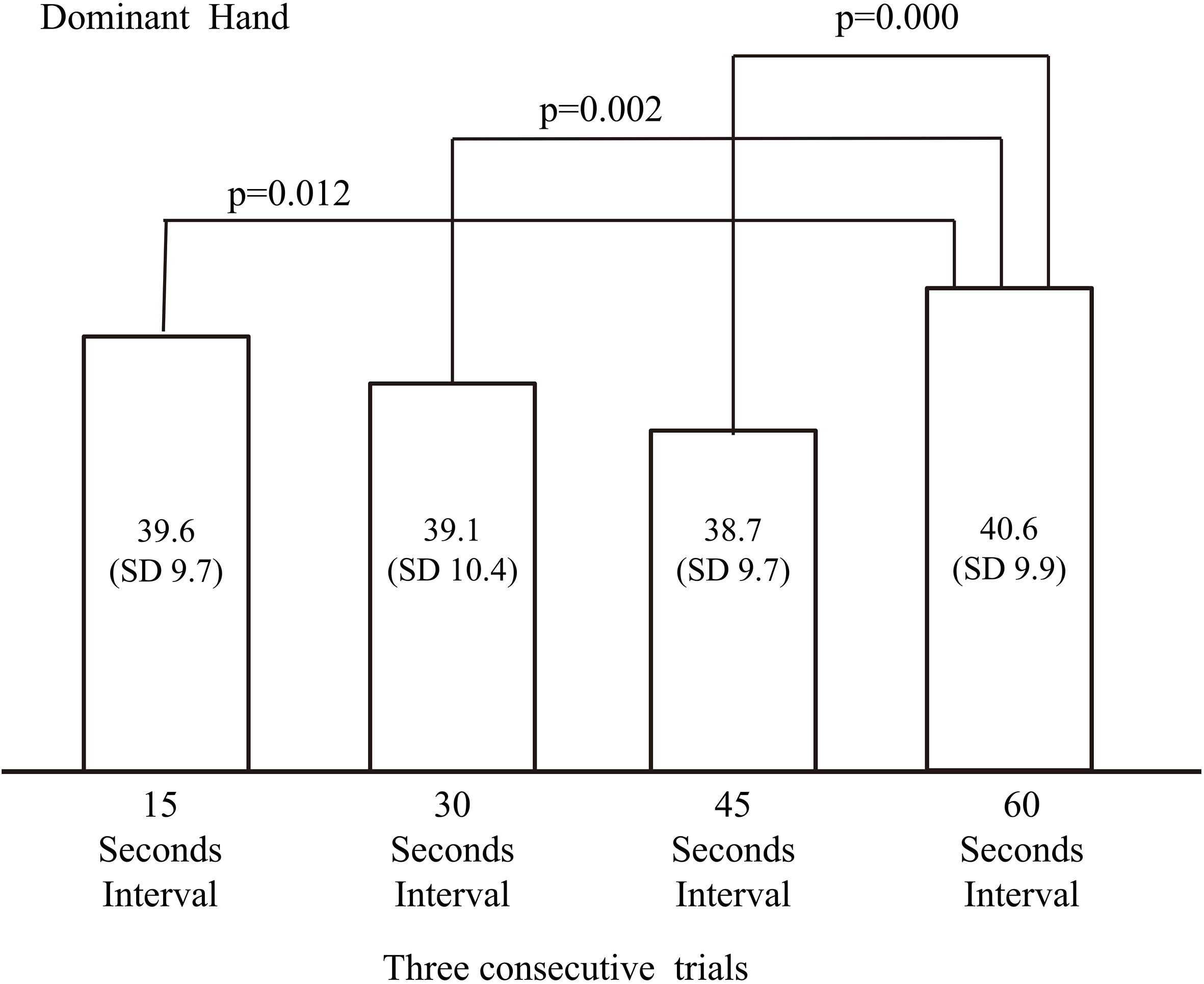
Distribution of subjects with maximal handgrip strength according to trials with a 60-s interval (4A: Dominant hand, 4B: Non-dominant hand).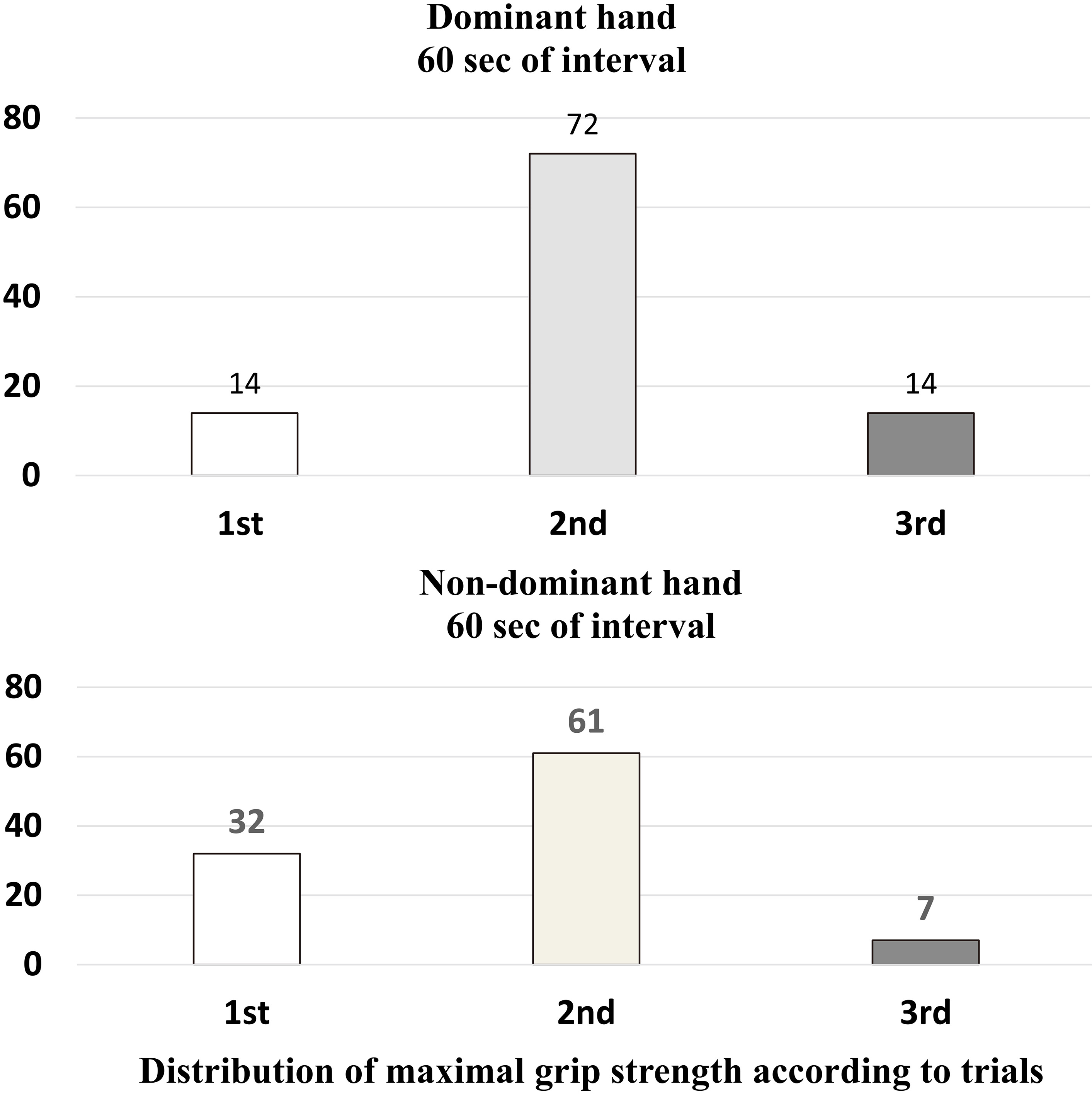
To verify the minimum optimal interval between trials, 15, 30, 45 and 60-s intervals between grips were measured. Thus, for each interval, three consecutive trials of the measurement were performed. One rest day was allowed between each time interval. We performed measurements between 17:00 and 19:00 hours to exclude the possibility of diurnal measurement variation. We assessed the dominant hand first and then the non-dominant hand in that order, and true hand dominancy was re-evaluated after measurements to rule out the possibility of the 10% rule of hand dominance [30]. The minimum optimal number of trials for each interval was determined by comparing maximal handgrip strength in two and three consecutive trials. Then the values for the minimum optimal number of trials at each interval were compared to one another (Fig. 1).
Sample size calculation
A pilot study with 15 subjects (male: 8) showed a difference of 2 kgf in mean grip strength with a standard deviation of 7 kgf. Considering the type I error as 0.05 and the type II error as 20%, the sample size was calculated as 97. We added 10% to the number of subjects (10) to compensate for the loss of data. One hundred seven subjects were scheduled to be enrolled in this study.
Statistical analyses
All statistical analyses were performed using the SPSS software package version 18.0 (SPSS, Chicago, IL, USA). The main hypothesis of this study was that two consecutive trials with a 15-s interval would be the minimum necessary to obtain maximal handgrip strength. We compared the maximal handgrip strength between two and three consecutive trials at four different intervals (15, 30, 45, and 60-s) using paired t-tests. After determining the minimum optimal number of trials at each interval, the comparisons between values for each interval were evaluated with paired t-tests. We also performed the subgroup analysis with the gender to prove the basic hypothesis of this study that gender could not affect the result of the study. Paired t-tests were also used to demonstrate this hypothesis regarding the gender subgroup analysis. A
Results
Dominant hand
Maximal handgrip strength during three consecutive trials at each interval were higher than the first two consecutive trials (15-s; 39.5 (SD 9.7) kgf vs 39.6 (SD 9.7) kgf,
Non-dominant hand
Maximal handgrip strength during three consecutive trials at each interval were higher than two consecutive trials (15-s; 34.4 (SD 8.8) kgf vs 34.6 (SD 8.7) kgf,
Subgroup analysis with the gender
We observed that the gender factor in this study did not affect the main result of a minimum optimal number of trials and intervals, supporting previous findings by Watanabe et al. [22]. The minimum optimal number of trials was determined to be three consecutive trials at 60-s intervals in each gender’s dominant hands (all
Subgroup analysis according to the gender comparing handgrip strength between two consecutive trials and three consecutive trials with every interval (15, 30, 45 and 60-s)
Subgroup analysis according to the gender comparing handgrip strength between two consecutive trials and three consecutive trials with every interval (15, 30, 45 and 60-s)
SD: Standard deviation. Dom – dominant, Nondom – nondominant, The maximal handgrip strength was measured at 60-s interval and revealed to be superior to other intervals (
Comparison of maximal hand grip strength between two and three consecutive trials at each interval (15, 30, 45, and 60-s) in the non-dominant hand.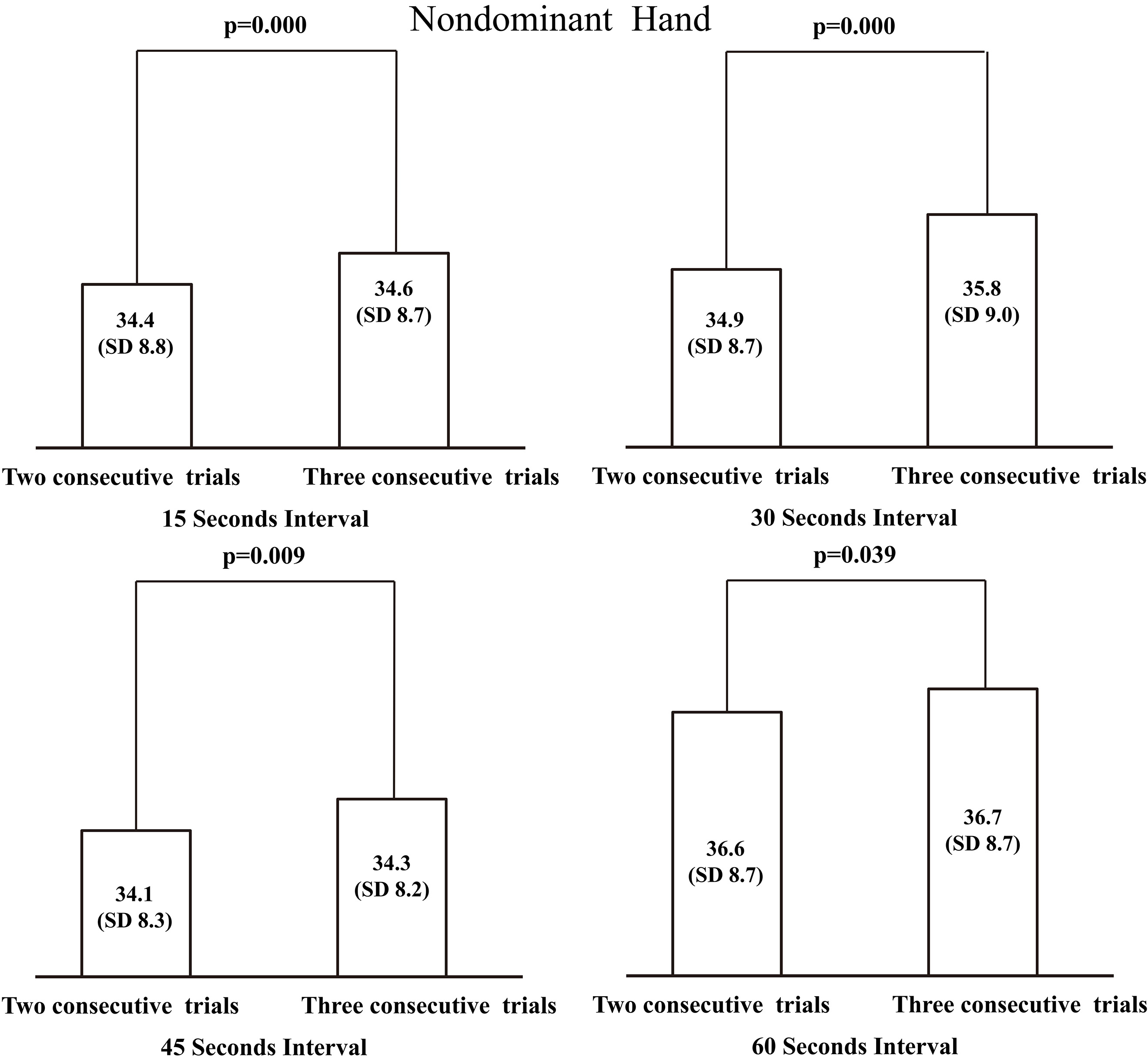
Maximal handgrip strength for the minimum optimal number of trials (three consecutive trials) at 60-s compared to other intervals (15, 30 and 45-s intervals) in the non-dominant hand.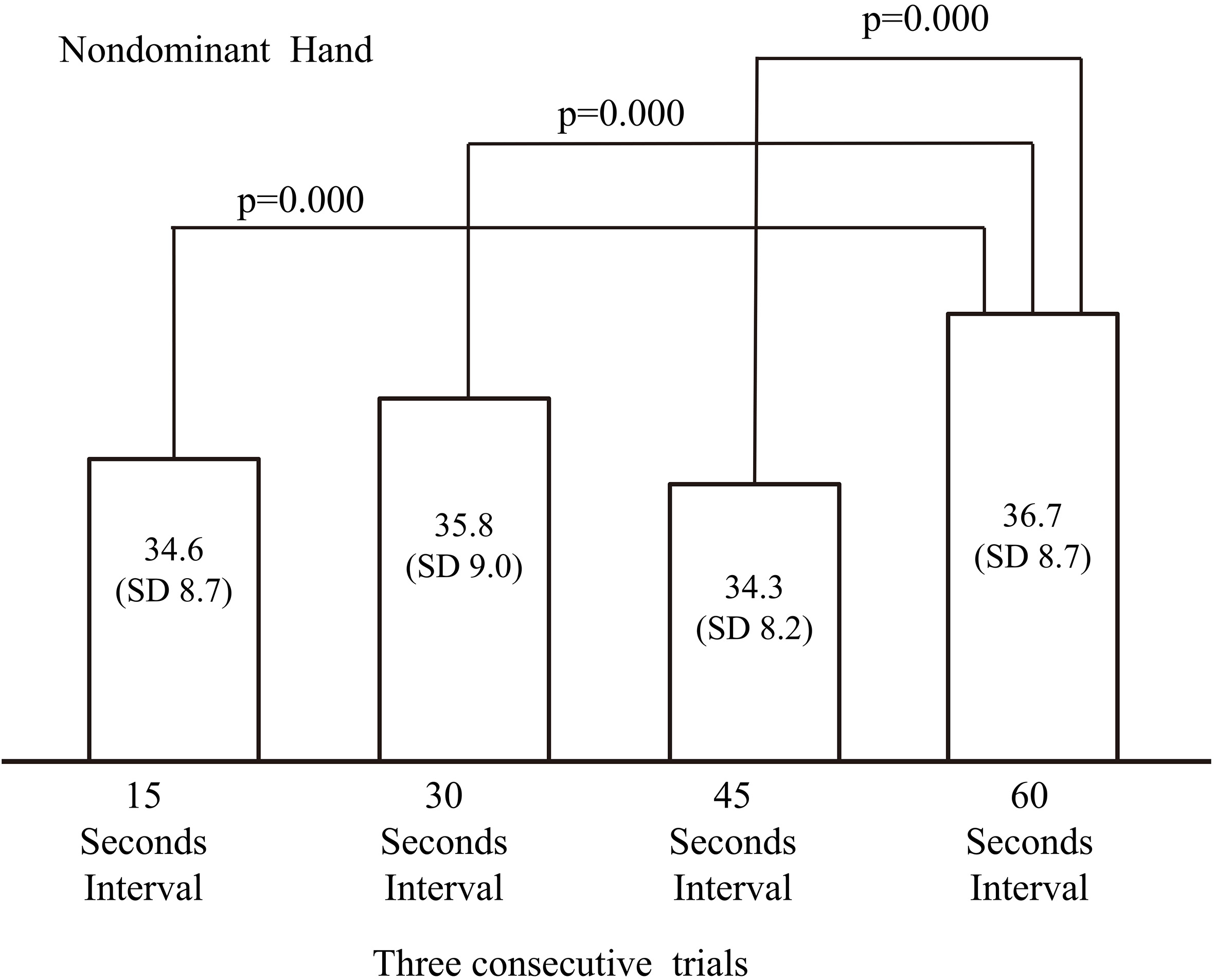
According to the current study results, three consecutive trials with a 60-s interval should be performed to identify maximal handgrip strength. This result could be applied in population-based studies regardless of hand dominancy. We observed that 7% to 14% of subjects by hand dominance showed maximal handgrip strength in the third trial, and this might result in the need for three rather than two consecutive trials.
The measurement of handgrip strength as one of the assessment tools for the national health index might be important to develop future nationwide health policy [6, 8, 31, 32]. However, there still are some debates about the optimum number of consecutive trials among several epidemiologic studies [2, 22, 24, 25, 33, 34]. In fact, the hand grip strength in subjects above 19 years of age has been measured biennially since 1989 for the Korean National Fitness Assessment (KNFA) [12]. However, this measurement was performed on two consecutive occasions with no rest period between trials. According to the NHANES (National Health Assessment and Nutrition Examination Survey) in the United States of America, the annual measurements of handgrip strength in subjects above six years of age have been performed by conducting three consecutive trials with a 60-s interval between each trial [13]. A 60-s rest between trials has been known to control for the confounding effect of fatigue on results, and in some subjects maximal handgrip strength was measured in the third trial, as in our study [21]. Some of the previous studies recommended a long rest between trials [23, 35, 36, 37]. However, the measurement of handgrip strength in a large population could be time-consuming and might cause some burden on the examiners due to the large number of trials and long inter-trial intervals. Also, Trossman et al. reported that there were no differences among 15, 30, or 60-s rests between trials during the measurement of handgrip strength [21]. Therefore, trials with a small inter-trial interval could be worth performing. However, we found that three trials with a 60-s inter-trial interval showed significantly higher values of maximal handgrip strength than a fewer number of trials with a small inter-trial time interval. In this study, we aimed to compare the 45-s interval, which has not been evaluated in previous studies, with other interval lengths. We found that measurements of handgrip strength with a 45-s interval were always lower than those with a 60-s interval.
Mathiowetz [34] suggested that three attempts could lead to learning effects and adaptation. Assessment of grip strength may be the first experience for some people and may need adjustment for learning. Coordination and learning of short-term motor skills can take several minutes, which may be achieved through spatial working memory [38]. The current results likely reflect coordination and learning of short-term motor skills.
This study had several limitations. First, it is based on healthy subjects and not on patients with chronic disease or sarcopenia whose results might contribute to non-standard outcomes. Second, we did not examine the efficacy of more than three trials and a more than 60-s interval compared to three trials with a 60-s interval. Third, subjects’ level of physical activity was not meticulously controlled although a medium occupational demand was identified in every subject.
The strengths of this study were as follows: First, it was a study in a large number of subjects. Second, a 45-s rest between trials was first adopted, and it proved to be inferior to a 60-s rest. Third, we tried to rule out as many factors as possible that might affect handgrip strength. Fourth, we suggested the possibility of adaptation of short-term motor skills as well as the fatigue theory for the superiority of three trials with a 60-s interval. Finally, we emphasized the need for sufficient trials with a sufficient time interval in epidemiologic studies, which should not be influenced by timeserving.
Conclusion
For the measurement of maximal handgrip strength, 3 consecutive trials with a 60-s interval is optimal, although it is more time consuming.
Footnotes
Conflict of interest
The authors declared no conflict of interest.