
Abstract
Informal or unpaid caregivers, commonly known as family caregivers, are responsible for providing the 80% of long-term care in Europe, which constitutes a significant portion of health and social care services offered to elderly or disabled individuals. However, the demand for informal care among the elderly is expected to outnumber available supply by 2060. The increasing decline in the caregiver-to-patient ratio is expected to lead to a substantial expansion in the integration of intelligent assistance within general care. The aim of this systematic review was to thoroughly investigate the most recent advancements in AI-enabled technologies, as well as those encompassed within the broader category of assistive technology (AT), which are designed with the primary or secondary goal to assist informal carers. The review sought to identify the specific needs that these technologies fulfill in the caregiver’s activities related to the care of older individuals, the identification of caregivers’ needs domains that are currently neglected by the existing AI-supporting technologies and ATs, as well as shedding light on the informal caregiver groups that are primarily targeted by those currently available. Three databases (Scopus, IEEE Xplore, ACM Digital Libraries) were searched. The search yielded 1002 articles, with 24 articles that met the inclusion and exclusion criteria. Our results showed that AI-powered technologies significantly facilitate ambient assisted living (AAL) applications, wherein the integration of home sensors serves to improve remote monitoring for informal caregivers. Additionally, AI solutions contribute to improve care coordination between formal and informal caregivers, that could lead to advanced telehealth assistance. However, limited research on assistive technologies like robots and mHealth apps suggests further exploration. Future AI-based solutions and assistive technologies (ATs) may benefit from a more targeted approach to appeasing specific user groups based on their informal care type. Potential areas for future research also include the integration of novel methodological approaches to improve the screening process of conventional systematic reviews through the automation of tasks using AI-powered technologies based on active learning approach.
Introduction
Background
The significance of informal care is expected to increase in the coming years owing to demographic shifts, advancements in healthcare, policies regarding long-term care, and cost-reduction pressures that prioritize community-based care alternatives over institutionalization, whenever feasible [20]. Informal or unpaid caregivers, commonly known as family caregivers, are responsible for providing the 80% of long-term care (LTC) in Europe, which constitutes a significant portion of health and social care services offered to elderly or disabled individuals [36]. The demand for informal care among the elderly is expected to outnumber available supply by 2060, with a shortage of around 20,000 carers in the Netherlands, 400,000 in Germany, and over a million caregivers in Spain [79]. These countries were chosen as representatives for each cluster identified in the ANCIEN study, which categorized European Union Member States into four clusters based on their LTC systems [46]. The potential shortage of supply in meeting demand can be attributed to demographic patterns, specifically the increasing proportion of elderly individuals, particularly those in the most advanced age groups, at a faster rate than younger cohorts [78]. In addition to changes in demographics, socio-structural changes such as declining fertility rates, increased mobility, and greater female labor market participation have led to a decrease in the availability of potential caregivers in many countries, although the extent of this decline varies [19, 41]. The predicted decline in the number of informal caregivers is creating a “care gap” [78] that, when combined with the increasing complexity of the population’s care needs, will pose significant challenges to the future sustainability of global healthcare and social care systems [103].
The increasing decline in the caregiver-to-patient ratio is expected to lead to a substantial expansion in the integration of intelligent assistance within general care [39]. Artificial intelligence (AI)-enhanced interventions are increasingly being developed to support the health and capacity of older people receiving LTC, with the goals of expanding the reach of care provision, increasing its efficiency, and reducing caregiver burden [17, 55]. These technologies can improve workforce sustainability by offering additional assistance to caregivers and addressing service inequity in remote areas with limited access to LTC and high demand [55]. In recent years, there has been an emergence of newer forms of assistive technologies (ATs) that incorporate elements of AI [61]. Assistive technology [9], intelligent assistive technology [57], innovative assistive technology [91], are some of the terms used in the literature to describe the technology used to support care-dependent individuals [4]. AT is an umbrella term [9] which refers to devices or systems that enable individuals to perform tasks they would otherwise be unable to do, or enhance the ease and safety of task performance [59]. Technological interventions have the potential to provide family caregivers with various tools and resources to address their caregiving responsibilities [11] and AT serves as a viable approach to facilitate the process of caregiving [6]. However, the potential of technology aids to enhance the caring experience is hindered by the limited implementation and adoption of these technologies in practical and real-world settings [11, 52].
Informal caregivers and their needs
There is a lack of consensus in both scientific and grey literature over the precise meaning of informal caregiving [92].
While the World Health Organization (WHO) does not offer a formal definition of the term informal caregiver [92], the Organisation for Economic Co-operation and Development (OECD) defines informal carers as “people providing any help to older family members, friends and people in their social network, living inside or outside their household, who require help with everyday tasks” [68], or those who “may provide care to friends or family members, or may do so as part of non-contractual voluntary work” [67]. Only family members, friends, or unpaid volunteers who offer regular assistance to care recipients and do not get cash or other benefits other than those intended to support caring activities are considered informal caregivers in the OECD reporting purposes [92]. Nevertheless, it is worth noting that further publications from the OECD emphasize that informal carers “may also be undeclared or illegal caregivers who receive a salary or compensation from the care recipient, but do not have an official contract with them and are not registered with relevant social security offices” [67]. This phenomenon reflects a growing global trend wherein private families employ care workers, predominantly migrants, to assist them in the daily care of their dependent family members [92].
The United Nations Economic Commission for Europe (UNECE) notes that different definitions of informal carers are provided in national and regional legislation, and highlights the overlapping nature of this term with that of “family caregiver” [93]. Certain conceptualizations of informal carers may fail to include the presence of remunerated, yet non-professional carers who offer caregiving services within private households [93]. Accordingly, UNECE defines informal care as “all non-professional care provided – by choice or by default – by family members (next of kin), friends, neighbours or other persons caring for people with long-term care needs at all ages, usually in private households” [93], but categorizes informal care relationships into distinct groups: (a) working-age adults who provide care for older parents, family members, neighbours, or friends; (b) individuals of retirement age or older who care for their partners, family members, neighbours, or friends; (c) young individuals who care for their parents, grandparents, or other family members; and (d) paid non-professional caregivers who either substitute or supplement the care provided by the family [93].
While informal care often remains uncompensated, there is a discernible rise in the presence of remunerated informal caregivers who are replacing or complementing the informal care given by relatives [93]. The composition of this group predominantly consists of women who have migrated either permanently or temporarily, with or without qualifications, and are remunerated under several regulations [93].
Studies differ in their approaches to measuring the types of assistance caregivers provide [83]. Van Durme et al. [98] conducted a literature review and identified many indicators that researchers utilize to denote the significance of informal carers. The majority of the articles they retrieved refer to carers in terms of the relationship they have with the individuals they provide care for, such as spouse (e.g., [1, 47]), sibling and adult child (e.g., [1]), distant relatives (e.g. grandchildren, daughter/son-in-law, niece/nephew or cousins [2]), friends (e.g., [2, 60]), neighbours (e.g., [2]) and, in the broader sense, family members (e.g., [3, 60]) or relatives (e.g., [53]). Likewise, the nature of the aid supplied was found being commonly utilized as a criterion for denoting informal caretakers.
The provision of informal care involves a network of helpers who offer assistance to an elderly person, with a primary carer being the central figure and secondary helpers providing indirect support to the primary carer [75]. In the past, some studies have attempted to quantify the size of the informal care network. For example, Stone and colleagues [90] distinguished among types of carers based on their level of responsibility and the presence or absence of additional helpers: (1) specifically, carers were classified as primary carers only if they reported being primarily responsible for the care of the disabled individual and did not have any other helpers; (2) if they were one of several unpaid caregivers providing care, they were classified as primary caregivers with informal help; (3) those who provided care with the assistance of both unpaid and paid helpers were classified as primary caregivers with informal and formal help; (4) finally, caregivers who did not have primary responsibility for the care of the disabled person were classified as secondary caregivers. On the contrary, Penrod and colleagues [75] distinguished among types of caregivers based on the type of assistance (care, money, decisions) provided: (1) secondary helpers, including those who were not immediate family of the primary caregiver, such as a cousin or a non-family member, who assist the primary caregiver with direct care to the elderly rather than providing financial assistance or help with the major decisions about care; (2) primary caregivers who give help about personal care, household maintenance, and management tasks that involve overseeing and administering financial matters [75]. Similarly, Dilworth-Anderson and co-workers [23] distinguished three different type of caregivers by their level of responsibility and caregiving tasks: (1) primary caregivers are those who exhibit the highest degree of caregiving responsibility, execute the greatest number of caregiving tasks, are either unaided or receive support from additional caregivers; (2) the individual responsible for the primary care of a dependent identified secondary caregivers as individuals who perform comparable duties to those of the primary caregiver, albeit with a lesser degree of accountability. As a result, secondary caregivers are those who are not involved in decision-making responsibilities pertaining to the support and care of the recipient, and their role is limited to providing care in collaboration with primary caregivers; (3) tertiary caregivers are typically recognized by the primary caregiver and collaborate in providing care. The caregivers in question are primarily tasked with executing specific duties, such as running errands, tending to the garden, or managing financial obligations, and are not typically involved in the decision-making process regarding the care recipient. Certain tertiary caregivers offer care to independent elderly individuals in the absence of additional caregivers, typically those who are highly functional. Similar to primary caregivers, the identification of tertiary caregivers is carried out by the care recipients or their proxies. Most recently, the work by D’Amen and colleagues [28] provided a classification of family caregivers, distinguishing between primary caregivers, secondary caregivers, tertiary caregivers and auxiliary caregivers. Specifically, auxiliary caregivers were defined as those who offer supplementary aid to primary caregivers in order to enhance the quality of care provided, offer companionship to care recipients, such as grandparents, and strive to address their emotional needs while engaging in social activities with them [10, 80].
This study will use the work by D’Amen and colleagues [28] as a reference point.
Objectives
The aim of this study is to provide as wide as possible state-of-the-art on the AI-based technologies and ATs deployed in assisting informal caregivers with their caregiving duties and personal needs. The goal is to gain an understanding of the needs for support related to caregiving activities and personal assistance for informal caregivers, which are addressed via the utilization of AI-based technologies and ATs. This study aims at contributing valuable insights towards the identification of caregivers’ needs domains that are currently neglected by the existing AI-supporting technologies and ATs, as well as shedding light on the informal caregiver groups that are primarily targeted by those currently available.
The remainder of this paper is structured as follows: Section 2 outlines the methodology that was employed in this study; Section 3 presents the results of the study, while Section 4 provides a summary of the key findings, discusses their significance, and proposes potential avenues for further research. Section 5 and Section 6 encompass the limitations of this study and set the stage for advancements performing systematic reviews with AI-assisted screening systems using active learning. Section 7 provides a set of closing remarks.
Method
This section presents the methodology used in the study. This study conducted a systematic literature review (SLR). SLR is a research methodology that involves the systematic collection, identification, and critical analysis of existing research works using a structured procedure [74]. The objective of this study is to critically evaluate key aspects of existing information pertaining to a certain research question, with the aim of identifying potential avenues for further investigation [15]. Considering the purpose of the present study, a SLR is deemed a suitable research methodology. There are several approaches for performing an SLR within the domain of computer science research (e.g. [70, 76]). In our study, the principles laid out in Moher et al. [64] were adhered to (e.g. [22, 63]). The steps involved in the development of the SLR methodology are outlined in the following sections.
Research questions
The primary research question of this review is: “What is the state-of-the-art on the artificial intelligence (AI)-based technologies or assistive technology deployed in assisting informal caregivers in an ageing society?”. This main question can be subdivided into the subsequent research questions:
What are the existing AI-based technologies or assistive technologies developed to support informal caregivers with their caregiving duties and personal needs?
What are the activity support needs of informal carers and the personal support needs of those caregivers that are addressed by current AI-based technologies or assistive technologies?
What types of informal carers are addressed by current AI-based technologies or assistive technologies?
Search strategy
The SLR was conducted in Scopus, IEEE Xplore, and ACM Digital Library databases. These databases were chosen due to their extensive collection of primary research pertaining to the subject of computer science [94].
A pilot search was conducted in Scopus database based on the following preliminary set of keywords: “artificial intelligence”, “AI”, “assistive technology”, “caregiver”. The earlier set of keywords was combined into a search string using the Boolean operator “AND” with the exception of the alternative term “AI”, which was joined using the Boolean operator “OR”. Following the exploratory search, adjustments were made to refine the search terms. The original set of keywords was broadened to encompass additional terms related to the category of care recipients, as identified in multiple literature sources. The classification of four informal caregiver categories, as outlined in the work by D’amen et al. [28], was employed in this study. Due to the number of results generated by the refined combination of terms, no supplementary terms or variations in terminology were necessary.
Search strings were identical for Scopus, IEEE Xplore, and ACM Digital Library, except for variations in syntax required by each database. Filters by title, abstract and keywords were applied to the search query. The initial search was conducted in June 2023 and subsequently replicated to include newly indexed until early July 2023. The search strings used to query the digital sources are shown in Table 1.
Search query
Search query
A set of inclusion and exclusion criteria were specified to filter the articles based on the objective and the research questions of this review. The studies identified by the search strategy have been selected based on whether they met all of the inclusion criteria outlined below:
Caregivers were informal carers or unpaid voluntary helpers;
The article describes or evaluates an AI-based technology or assistive technology developed with the primary or secondary goal to assist informal carers in fulfilling their caregiving duties and personal needs, mentioned in the referenced literature (i.e. [8]);
On the contrary, articles were not included whether they met any of the following exclusion criteria:
Targeted caregivers were professionals;
The AI-based technology or assistive technology was not expressively tailor-made for caregiving;
Articles were not in English;
Articles were reviews, commentaries, abstract, theoretical frameworks.
Study selection
Two authors worked independently to apply the selection criteria to all papers obtained through the search process in a three-phased approach.
First, the titles and abstracts of the entire set of papers were screened for duplicates. Second, a preliminary screening phase was conducted to identify papers for full text screening. This phase involved manually reviewing the abstracts of the retrieved papers. Third, both authors thoroughly examined the whole texts of the remaining papers in order to validate their relevance to the research questions. A cross-check of the selection process results was conducted to ensure the accuracy of the selection process. Discrepancies on the selected articles were discussed by the authors until a consensus was found. The web-based tool Rayyan [72] has been used to support the duplicate selection process and to streamline the subsequent screening and selection process for relevant studies.
Quality appraisal
The studies included in this review were evaluated for quality. The following seven quality questions were extracted from the works by Zhou et al. [104] and Shakeel et al. [87]:
Is there a clear statement defining the objective and goal of the work?
Is there an adequate description of the context in which the research was carried out?
Is there an adequate description justifying the choice of the research method?
Is the research method appropriate to address the defined goal?
Do the researchers discuss any problems (limitations, threats) with the validity (reliability) of their results?
Has sufficient data been presented to support the findings?
Is the study of value for research or practice?
The use of a quality checklist is consistent with the ones developed in other studies on similar topic (e.g. [99]). In accordance with the research conducted by Shakeel et al. [87], the aforementioned criteria for evaluating quality comprise the four main areas of concern identified by Dybå and Dingsøyr [27]. Questions Q1 and Q2 have been utilized to address the domain of Reporting that pertains to the assessment of the quality of reporting about the rationale, objectives, and contextual background of a research study. Questions Q3 and Q4 have addressed the aspect of Rigor, which pertains to the robustness and comprehensiveness of the research methods used to establish the trustworthiness of data gathering instruments and analytical processes. This ensures the reliability of the study findings. The evaluation of a study’s methodological rigor to determine the validity and significance of its findings is encompassed by the Credibility domain, which has been examined through questions Q5 and Q6. Additionally, the scientific significance of papers, falling under the Relevance domain, has been assessed through question Q7.
Two authors conducted the analysis of each chosen paper in order to evaluate its quality. Disagreements were discussed by the authors until a common decision was reached. A comprehensive score has been obtained by computing the average of the points assigned to each quality questions as indicated earlier [65]. A value of 1 has been assigned to a positive response, 0.5 to a partially positive response, and 0 to a negative response [65, 87]. As suggested in previous research (e.g. [26]), a specific criterion was established to determine whether a publication should be included or excluded from the final set of evaluated papers. Only criterion Q7 was utilized, as the focus of the present review is not merely on empirical studies to answer the research questions in Section 2.1.
Data extraction
Data were extracted manually by two authors independently and the results were collected and classified by a single author. The data that was retrieved proved to be pertinent to the research questions and encompassed three distinct domains: 1) general information about the publication; 2) specific information about the intended use of the supporting technology; 3) specific information about informal caregivers and caregiver-recipient dyads. Details of the data extraction form are shown in Table 2.
Data extraction
Data extraction
After extracting the information from all the papers included in the analysis, descriptive statistics were employed to provide a concise summary of the overall findings. Excel (Microsoft) was used to perform data analysis.
A total of 1002 papers were identified through searching the three databases. After the preliminary screening for duplicate, 961 papers were manually screened by abstract and title, resulting in 231 papers eligible for full text screening. After full text screening, the total number of papers included in the analysis were 24.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart [64] of the selection process based on inclusion and exclusion criteria is presented in Fig. 1. The following sections details the articles’ characteristics after running through the selection process, the quality appraisal of the selected studies and the research questions using the 24 included studies that are stated in Tables 3 and 4.
Table 3 summarizes the studies included in this systematic literature review on the basis of the data extraction format described in the Section 2.6
Table 3 summarizes the studies included in this systematic literature review on the basis of the data extraction format described in the Section 2.6
Table 4 summarizes the studies included in this systematic literature review on the basis of the data extraction format described in the Section 2.6
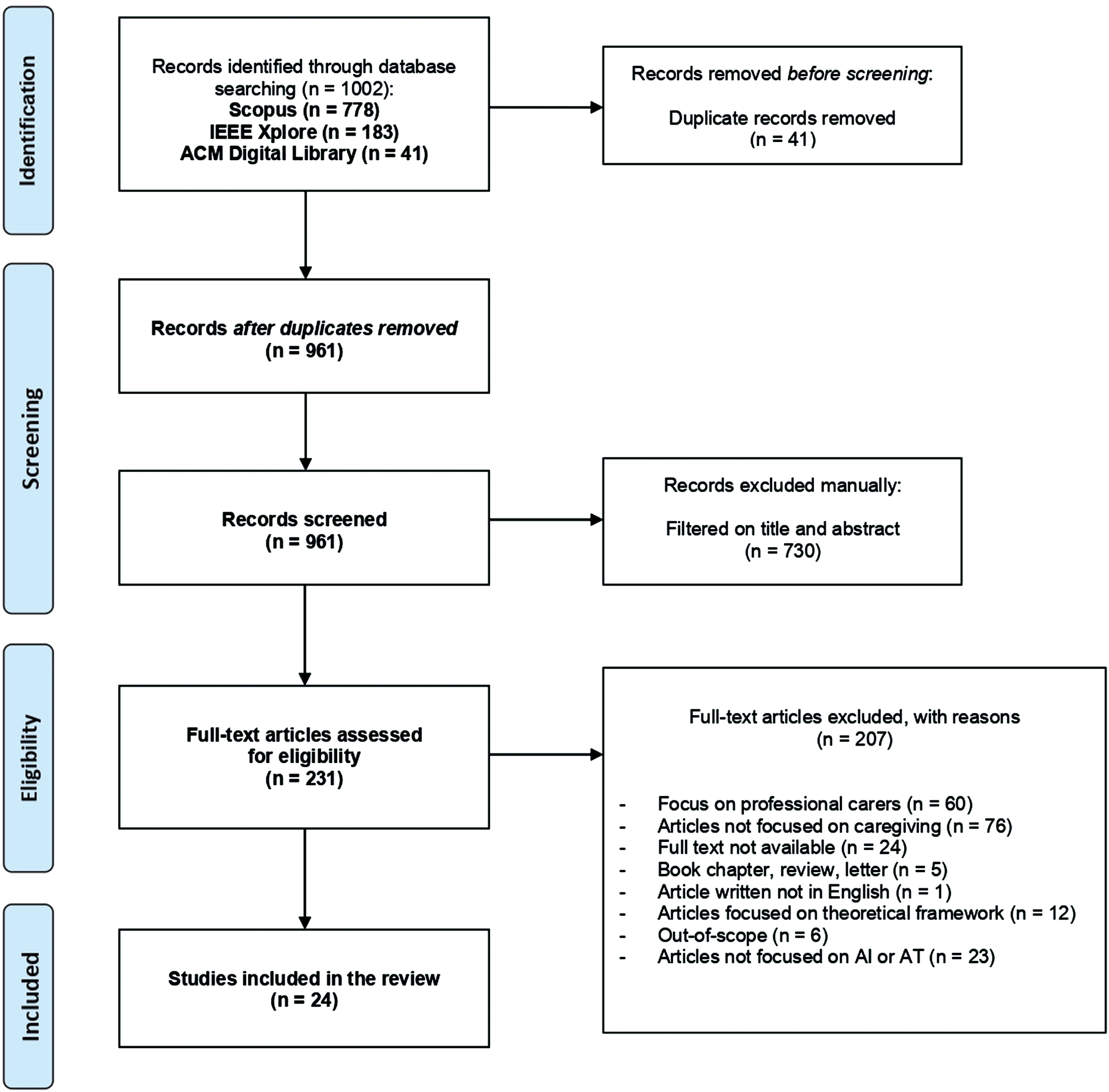
The flow chart shows the selection procedure of the included papers based on the PRISMA guidelines.
More than 58% of the selected papers are affiliated with authors from Europe. However, USA researchers contributed to 20.8% of the papers included in the study, making them the most active contributors. Italian researchers ranked second, with 16.7% of the articles (Fig. 2).
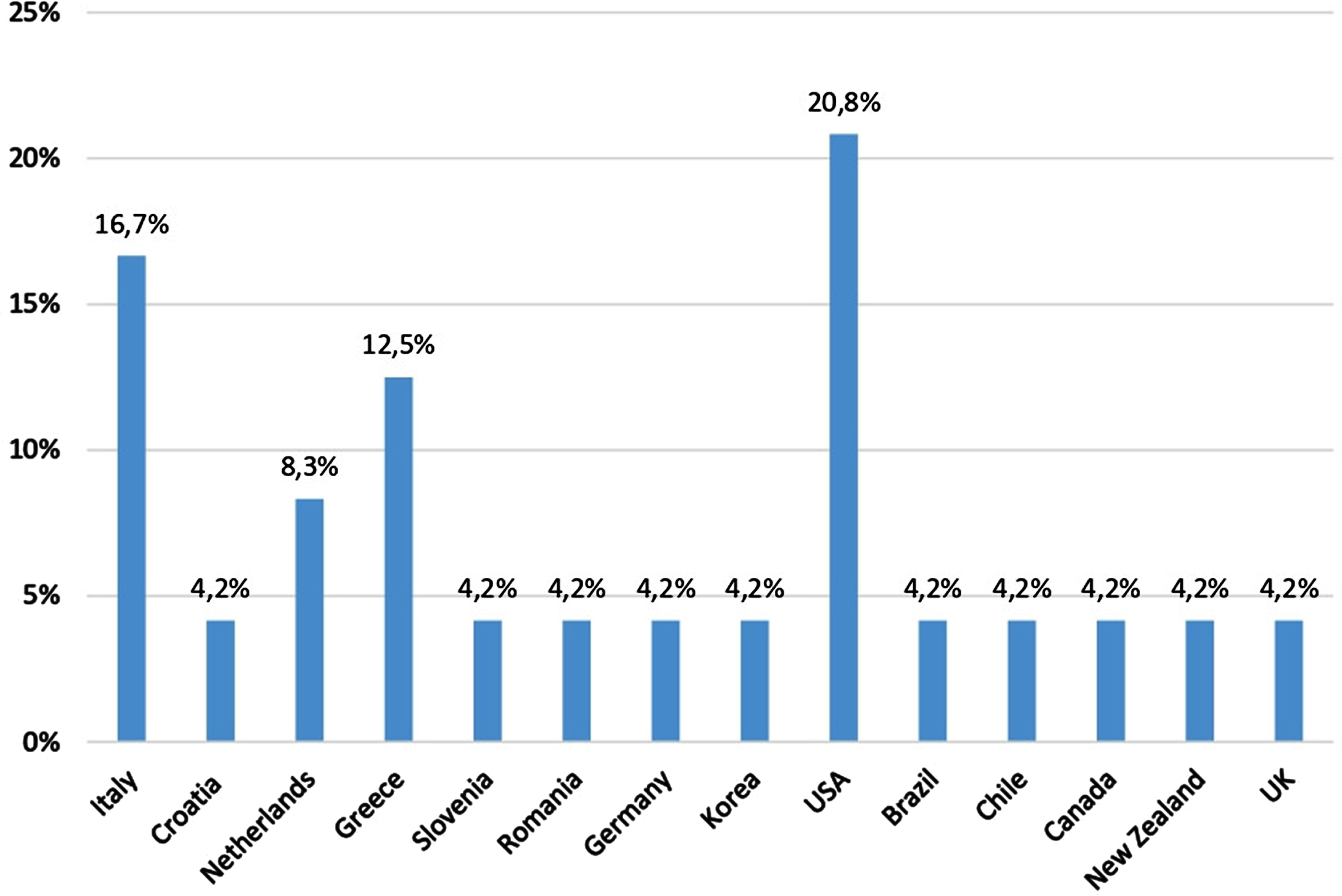
Distribution of the selected papers by country. Information refers to the affiliation of the first author.
The publications chosen for this study span the years 2013 to 2022, as shown by their respective publication dates. A considerable quantity of articles is situated inside the time span encompassing the years 2017 to 2018, as well as between the years 2020 and 2021. The highest amount of articles picked is observed within the most recent biennial interval (2020-2021), which comprises 37.5% of the total. Only 7 papers are journal articles, while the remaining 17 are conference papers. With the exception of the journal article [50], the selected conference papers primarily consist of proof-of-concept studies (53%) and to a lesser extent from concept design articles (29%) (Fig. 3).
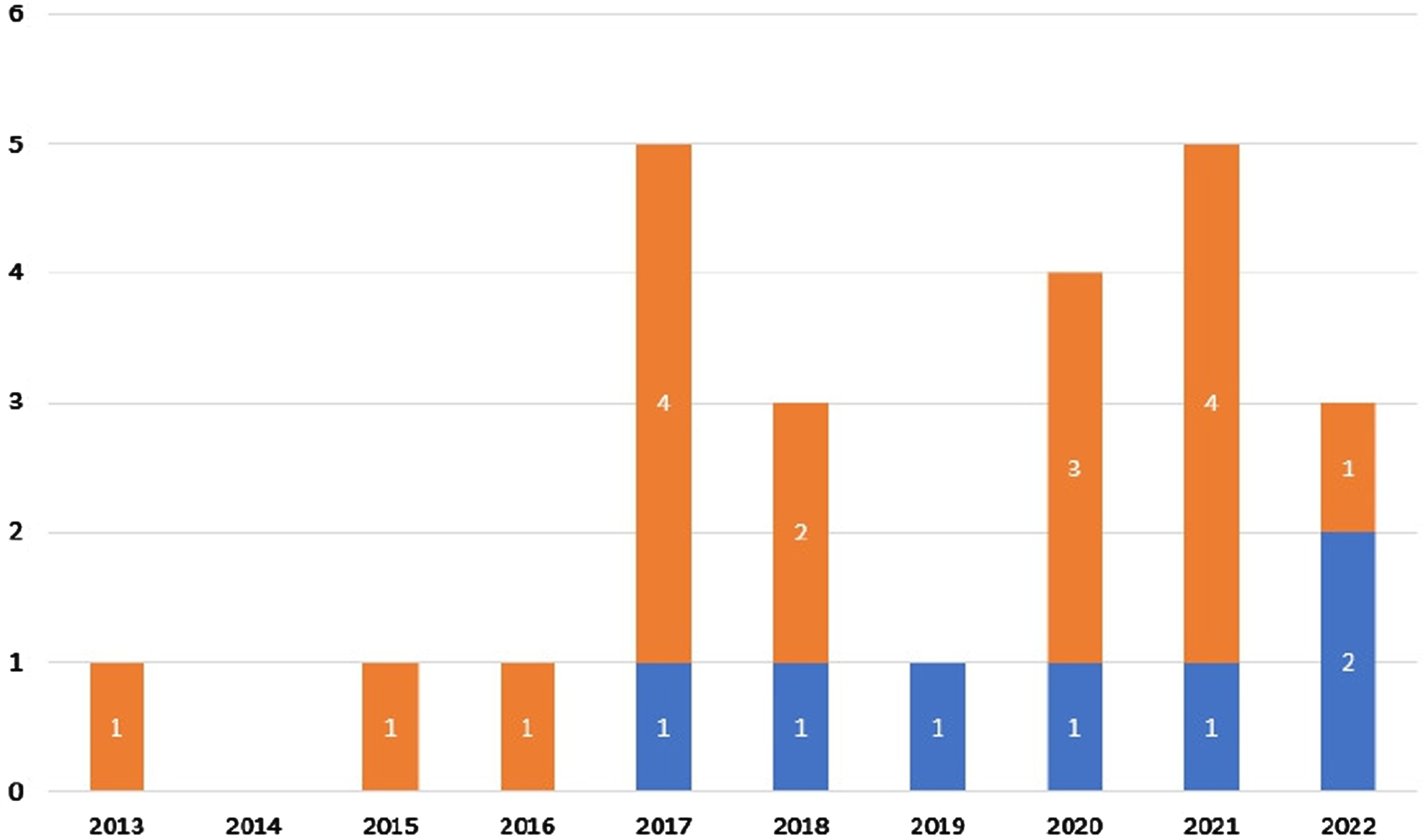
The stacked barplots show the included studies across different years of publication. Blue studies are journal papers, whereas orange studies are conference papers.
According to the quality appraisal methodology outlined in the Section 2.5, all the selected studies met the quality requirement Q7 and were included in the final review. Conference papers that only consisted of concept design studies, with no inclusion of usability tests, were excluded from the quality appraisal process due to a lack of quality assessment requirements [42–44, 89]. In what follow, a summary of the results obtained from the implementation of the scoring system on the remaining articles is presented.
Overall, the average quality scores of journal papers were higher than those of conference papers (Fig. 4). The questions that exhibited the most significant discrepancies were those related to the issues with the reliability of the findings derived from the research and the limits that were mentioned (questions Q5), as well as the absence of data presentation substantiating the findings (question Q6) (Fig. 5). The presentation of data supporting the findings was not consistently included as part of the 3 out of 12 conference articles [82, 95]. One article [13] failed to include an explanation of the limitations and issues pertaining to the validity of the findings. The study conducted by Leo et al. [49] did not satisfy any of the criteria Q5 and Q6, as it was a presentation of a proof-of-concept study that will undergo further testing.
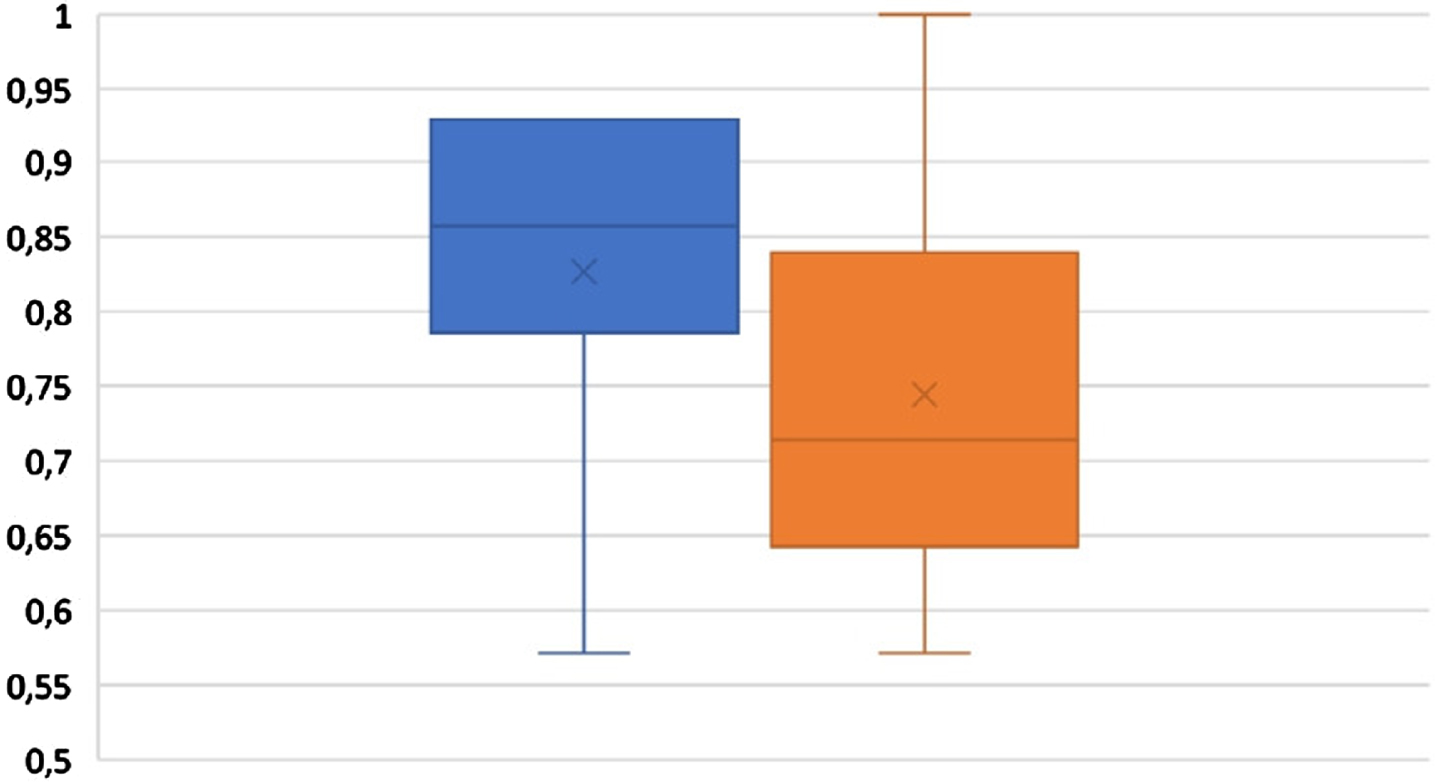
The boxplots show the distribution of quality scores by publication type. The blue boxplot represents journal publications, whereas the orange boxplot represents conference papers.
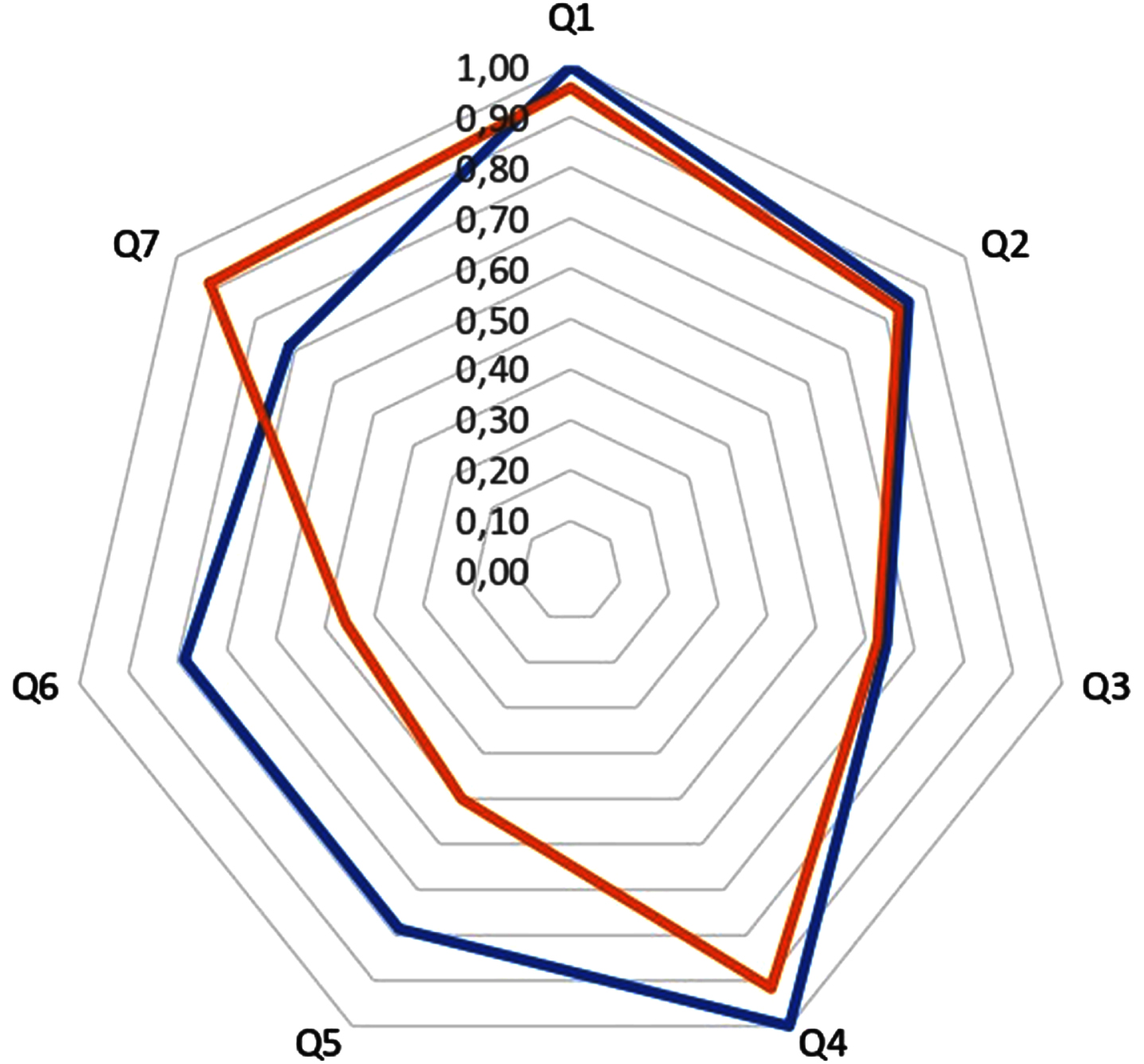
The radar chart shows the global quality scores per question. The blue line represents journal publications, whereas the orange line represents conference papers.
RQ1. What are the existing AI-based technologies or assistive technologies developed to support informal caregivers with their caregiving duties and personal needs?
Artificial Intelligence
The largest proportion of the reviewed studies (11 out of 24) concerned AI-based technologies supporting non-professional helpers in fulfilling the care needs of the elderly they cared for. Of these, seven studies describe the use of conversational agents (CAs) [7, 95], three studies integrate ambient assisted living solutions (AAL) [13, 37], one study extends the functionality of platforms for the management and coordination of informal care [43].
Regarding the use of CAs, in two studies CAs were integrated with a web app, serving as a back-end component that provides caregivers with awareness about scheduled caring activities and reminders for performing them [7], or using Machine Learning (ML) techniques that compute predictions, through counterfactual explanations, to suggest to caregivers rules able to detecting anomalous situations based on CA-collected elderly behavioural data [95]. Commercially available virtual home assistants, such as the Amazon Echo, were evaluated as aids for informal caregivers in the context of aging in place [30] or integrated with in-home sensor system to easily access personalized health information of seniors informal carers care for [73]. In one study an interactive medication assistant system was designed within the Google Home Hub [58]. A voice-enabled intelligent assistant was developed that utilized Amazon’s existing cloud-based voice service, Alexa, as a speech-to-text and text-to-speech conversation system in order to provide personalized advice to caregivers in carrying out caretasks [50].
Regarding the studies on AI-based technologies and AAL, AAL devices, such as wearable devices [13] or smart-home sensors [33] were integrated with ML algorithms to enhance the precision of identifying the optimal informal caregiver for dispatching alarm signals during emergency occurrences [37] or in case of behavioural anomalies for elderly living alone [13, 33], except for the work by Kondylakis et al. [43].
Sensors technology
A subset of seven articles included in the review examined the application of sensor-based technology in easing the duties of informal caregivers of older adults living alone. These articles explored various AAL applications including: the provision of assistance for tele-health services [89]; a cloud-based platform for AAL services provision [44] and customization of the remote assistance application [18]; the incorporation of fuzzy models to identify abnormalities in the behavioral patterns of co-resident caregivers [54]; a multilayered system (including sensors) to promote care networks [82]; and the utilization of wearable SOS devices to monitor any deviations from the established routines of the elderly [24] whose data were stored and get accessed by smartphone [105].
Robotics
Four studies explored the utilization of assistive robots (ARs) [100] or socially assistive robots (SARs) [42, 86] as supporting technologies to facilitate informal caregiving. Only two studies out of four proposed an integrated robotic solution with other assistive technologies, such as home automation equipment [42, 86], wearable health monitors and personal smart devices [42]. Two out of four studies proposed an application of SAR with a wireless sensor network to provide real-time updates on the whereabouts of elderly individuals being followed [48] or to communicate with back end cloud services to access and store fall detected events and monitored health data [42]. In contrast, Wang et al. [100] presented a tele-operated robot, without delving into the combination of sensor or AI-based technologies.
mHealth applications
Two articles examine AT solutions that employ mobile health (mHealth) applications (apps) to assist informal caregivers in performing activities of daily living (ADLs) through the use of visual mapping software applications [34], and investigate the implementation of a digital storytelling app [21].
RQ2. What are the activity support needs of informal carers and the personal support needs of those caregivers that are addressed by current AI-based technologies or assistive technologies?
Informal caregivers activity support needs
Half of the articles reviewed (12 out of 24) focus on examining applications that provide assistance to informal caregivers in duties exclusively related to the supervision and social support of the elderly.
AAL technologies mainly pertain to remotely monitoring the health status of the elderly [24, 89] and tracing the occupancy patterns of the elderly in their residential environment to the automated detection of hazards (e.g. falls) or alterations in their routines [24, 105]. In one paper, an AAL system allows informal carers to oversee the actions performed by the professional caregiver associated with the elderly person in an effort to share and coordinate care responsibilities [44]. Additionally, only the work by Chesta et al. [18] expands the goal of remote surveillance of seniors, allowing informal caregivers to trig also customized care actions to their beloved depending on the seniors’ contextual information, personal preferences, motivations, abilities, and needs, collected within AAL domain.
CA-based solutions primarily encompass a dynamic approach to monitoring the elderly. Informal carers are supported by care intervention rule-equipped CA to determine suitable monitoring strategies for their loved one’s behavior and attitude [95]. Alternatively, voice-based CA can be used to deliver personalized health messages and receive alerts regarding falls [73]. It is worth noting that only in the work by Valtolina et al. [95] CA has been intended also to give companionship to the elderly through gamification, entertainment, and conversing and exchanging tales. In contrast, the incorporation of ML methods into AAL systems mainly offers monitoring solutions that are designed to notify informal caregivers in the event of life-threatening emergencies involving elderly individuals [13, 37]. However, ML techniques integrated with AAL systems also enable the monitoring of home conditions and in-home elderly activities, allowing for the customization of recommended rules and notification preferences [33].
One SAR application focuses on automating the monitoring of elderly individuals’ activities, detecting falls, and addressing emergencies with the purpose to reduce caregiver workload [48]. An mHealth application that assists informal caregivers in engaging in recreational activities with the older adults by promoting communication and conversation through the use of multimedia stories [21] is the only one out of the twenty-four articles introducing technologies specifically aimed at aiding caregivers in their social support tasks for the elderly.
Six out of the twenty-four articles explore the use of applications designed to support informal carers in managing organizational tasks. Robotics and AI-embedded solutions assist caregivers in recording medical appointments and general tasks [7, 86]; reminders that assist carers in managing recurring chores for the benefit of elderly individuals [7, 30]; timely communication with healthcare professionals [7, 42]; arranging meetings with a shared scheduling calendar with physicians [43]. Nevertheless, those technologies expand the range of organizational support duties by including secondary supervisory operations, such as automated health monitoring for the elderly [42] and emergency handling [43], and secondary joint leisure activities, like entertainment (e.g. music, jokes) [30]. Only one AAL solution facilitates the coordination of informal caregivers in the allocation of planned chores using a shared calendar system [82].
Three of the twenty-four articles examine the use of applications designed to assist informal caregivers with personal and medical care responsibilities. Only one of the examined technologies was intended to assist informal caregivers in managing personal care tasks, such as the nutrition of the seniors they care for, through the use of an AI-powered voice assistant designed to manage their daily diets and acquire food and nutrition-related information [50]. Two papers discuss technologies designed to assist caregivers in providing medical care to older people by improving seniors’ cognitive skills through the creation of memory maps into a CA-based solution [49], and by relying on a conversational “check-in” system for routine medication management [58]. Two papers [34, 100] did not provide explicit details about the specific tasks that were assisted, instead referring to them broadly as activities of daily living (ADLs).
Informal caregivers personal support needs
Out of the entirety of the selected papers, one article presents an AAL system that is specifically tailored to address the caregiver’s own care needs. The role involves aiding the carer in their daily caregiving responsibilities, identifying any deviations or mistakes in their performance, and offering direction to enhance or minimize the stress associated with their work [54].
Figure 6 shows the AI-based technologies and the assistive ones (i.e. sensors technology, robotics and mHealth apps) included in the systematic review. Figure 7 shows the AI-based technologies and the assistive ones by caring duties and caregiver’s own care needs that were assisted.
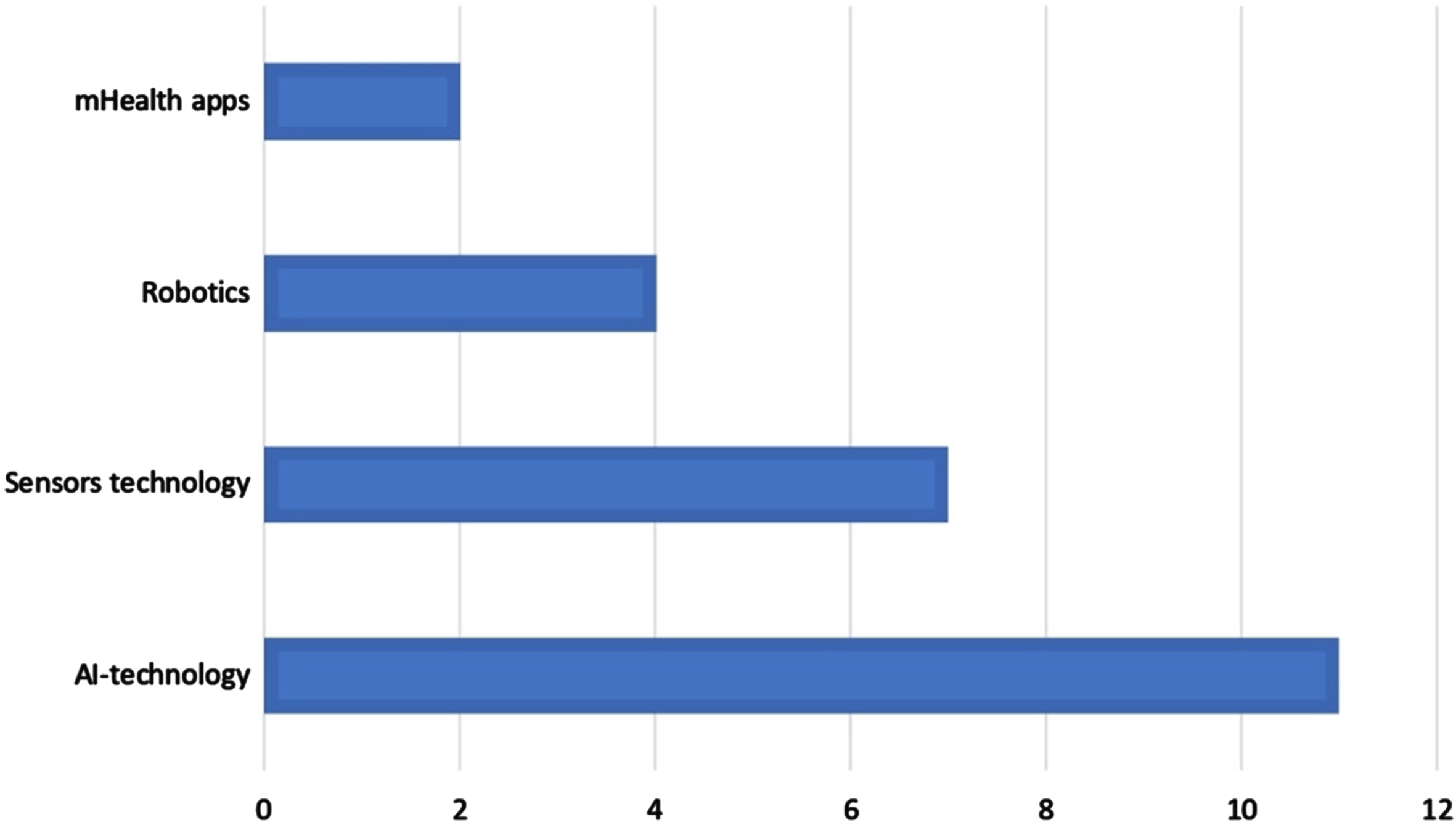
The bar chart shows the AI-based technologies and the assistive ones (i.e. sensors technology, robotics and mHealth apps) included in the systematic review. The x axis is the number of paper by technology.
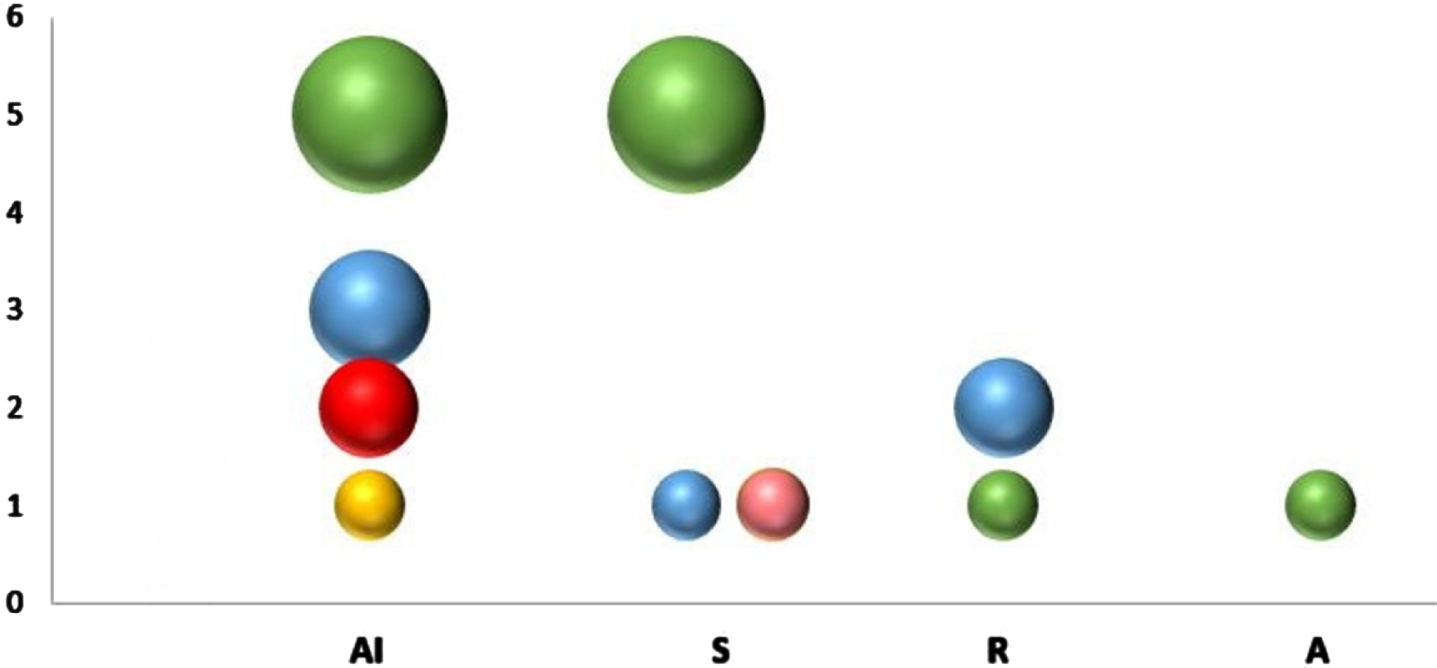
The bubble chart shows the AI-based technologies and the assistive ones by caring duties and the caregiver’s own care needs that were assisted. The y-axis indicates the number of technologies reviewed by their respective categories. The green color represents supervision and social support; the blue color represents support in organizational matters; the yellow color represents those tasked with personal care; and the red color represents medical care duties. The pink bubble represents the caregiver’s own care needs. AI: AI-based technology; S: sensor technology; R: robotics; A: mHealth apps.
RQ3. What types of informal carers are addressed by current AI-based technologies or assistive technologies?
The selected articles do not claim the type of caregiving, categorized on the basis of the amount of assistance provided, their level of responsibility, and the presence or absence of additional helpers. There is a lack of clarity in some articles on the identification of the specific individual who assumes the role of informal caregiver and is responsible for utilizing technology to fulfill their caregiving tasks. However, only a few articles refer to unpaid caregivers, often mixed in the same sample, such as partner or spouse [58, 86]; children [7]; sons [30]; daughters [30, 58]; friends [7, 37], neighbours [30, 37]; mother/mother-in-law [18]; relatives [7] and paid helpers [33]. Regarding the characteristics of carers, it is noteworthy that only 8 out of the total of 24 papers examined include specific information pertaining to the age of informal helpers. The age distribution across the articles exhibits heterogeneity, with the age range of helpers varying from 25 to 75 years old.
The papers incorporated in this review examine the AI-based technologies and assistive technologies (ATs) used in supporting informal carers in their caregiving duties for elderly individuals. Since the increasing decline in the caregiver-to-patient ratio is expected to lead to a substantial expansion in the integration of intelligent assistance within general care [39], it is crucial a thorough understanding of the needs for support related to caregiving activities and personal assistance for informal carers, which may be effectively addressed via the utilization of AI-based technologies or ATs.
Firstly, our analysis suggests that AI and sensors-powered applications serve as the predominant technology option for facilitating informal caregivers in their supervision activities. ML techniques play a crucial role in supporting assistive technologies, particularly applications of the ambient assisted living (AAL). Their primary objective is to automate the detection of hazards and anomalous patterns in the daily activities of elderly individuals in their living environment. In this vein, the sensor-based solutions provide a conducive living environment for older adults, allowing them to maintain their independence in a convenient and secure manner [89], and helping informal carers in their surveillance responsibilities through the use of remote monitoring solutions. Interestingly, these solutions were designed to accommodate a wide variety of elderly individuals who are in need of assistance from informal caregivers: those who are in good health-related status, individuals who have health-related limitations, individuals diagnosed with chronic health conditions, and individuals exhibiting mild or moderate symptoms of dementia or cognitive impairment [18, 105]. This could potentially lead to the adoption of these solutions to support a certain degree of independence for older individuals who do not need constant monitoring due to physical or cognitive limitations but still can benefit from the assistance provided by their informal caregivers. However, the articles that were retrieved only focus on monitoring indoor environments tasked with fall detection or activity recognition, similar to the findings of other reviews currently available (e.g. [81]). Future research ought to focus on the development also of assistive technologies for outdoor settings. This should involve investigating the effects of urban environments, architectural and spatial factors, and social influences on the successful implementation of these technologies [45] for older adults who live independently and their caregivers.
Secondarily, our findings indicate that AI is being utilized to facilitate shared communication platforms, enabling efficient collaboration between professional carers and unpaid family caretakers who assume the responsibility of caring for the elderly. By offering both descriptive real-time data and automatic alarms, these systems have the ability to avert acute deteriorations or major injuries that can affect the older people, thereby potentially reducing the need for expensive institutional care and promoting prompt and safe healthcare [35]. This aligns with previous research, which recognizes the advantages of AI and ML as emerging technological interventions that can benefit family carers, by enhancing autonomy and safety for elderly individuals through higher efficacy in managing and coordinating care [51]. These applications facilitate the distribution of care responsibilities, assistance with daily tasks, and prompt intervention during emergencies. However, it is likely that the ultimate goal is to achieve advanced telehealth solutions, which effectively supplement the care offered by informal caregivers with the involvement of formal caregivers and healthcare professionals. This advancement might offer notable benefits for older adults and their non-professional carers who live in geographically remote areas with limited access to healthcare services. In this context, it is worth noting that a significant gap exists in the examined studies with regards to the use of location-based technologies for the elderly residing in remote areas, as well as the resulting effects on the support rendered by carers. Indeed, our analysis underscores the dearth of applications specifically designed to address the caregiving demands of elderly individuals and their carers residing in geographically remote areas, except for the study by Zwierenberg et al. [105] who took place in the rural area of Northern Netherlands. In the context of healthcare, information such as patient locations, hospital and caregiver locations, routing and tracking of an ambulances, time-series and static environmental factors of a location, and patients’ geographic movements is important [66]. Future research ought to concentrate on the exploration of integrating emerging technologies, such as AI and Geographic Information System (GIS) [66], to facilitate smart healthcare for informal caregivers and elderly individuals residing in remote areas.
Thirdly, the results of our review indicate that both AI and sensor-based solutions enable caregivers to access to a relevant source of information. Some of the reviewed articles allow carers to get personalized health information of the elderly, hence facilitating the customization of their caregiving activities based on the individual’s particular requirements. In this context, these technologies facilitate carers in making informed decisions on the assistance they provide, a factor that has the potential to enhance their confidence in delivering caring activities [84]. Studies have indicated that the empowerment of family caregivers might be impeded by several factors, one of which is a lack of adequate prior understanding on their assistance tasks [77, 88]. Nonetheless, only the work by Lofti et al. [54] proposed a virtual carer with the purpose of providing information to informal carers in the event that an activity was performed incorrectly as well as expanding their knowledge of the tasks by incorporating e-learning content support. This is an interesting aspect, given the current emphasis that some research is placing also on AI in the training of healthcare professionals [69]. In contrast, the majority of the reviewed articles introduce virtual home assistants and CAs that facilitate the streamlining of organizational tasks, including the recording of medical appointments and general tasks. Further research is required to explore the technological advancements that may contribute to the empowerment of informal caregivers, taking into account their personal support needs.
Fourthly, our research suggests that there has been a lack of comprehensive investigation into the subjects of assistive robots, socially assistive robots, and mHealth apps in relation to their potential to aid informal carers in their caregiving duties. With regard to the robots, aged users’ unfamiliarity with the most recent innovative assistive technology, such as robotics, was found to be a barrier to their adoption in a recent study [91]. This aligns with the findings reported in several articles included in the review (e.g., [100]), despite the fact that caregivers express positive views regarding the utilization of a robotic assistant for their tasks [48, 100]. Recent literature reviews on currently available commercial mHealth apps confirmed that apps were rarely tailored to specific groups of family caregivers [8], but more likely to meet the needs of personal caregivers [8, 85]. However, it has been found in other studies that mHealth apps, which are considered assistive technology used in therapeutic treatments for certain pathological disease such as dementia, may have different applications such as the ones included in the category of reminiscence and socialization [102]. This is interesting as it suggests that the primary functionalities for elderly care and those reflecting the support requirements of the caregivers tend to be separated in mHealth apps design. Ultimately, further research should be conducted on both the assistive technologies in order to expand the range of assistance that can be provided to informal caregivers, which currently focuses on supervisory and organizational tasks (the case of the robots) and with lesser extend to social support (the case of mHealth).
From an overall perspective, although the articles included in this study provide a clear identification of AI-powered technologies and the assistive technologies that support informal caregivers in their duties, and the associated tasks they facilitate are clearly delineated, the selected articles do not explicitly address the categorization of caregiver’s types based on the level of assistance provided, the degree of responsibility assumed, and the presence or absence of additional helpers, as discussed in the referenced literature (e.g., [23, 90]). The absence of a well defined target user group, with specific features and demands directly associated with the caregiving responsibilities that informal helpers are expected to fulfill, might potentially hinder the effectiveness of using such technologies in their daily routines. Further research is warranted to investigate distinct subsets of informal caregivers, with the objective of improving in-home care for older adults through the implementation of technologically-driven interventions that provide valuable assistance to informal caregivers. Moreover, future research should expand the scope of the analysis to encompass subgroups of carers that are peculiar to the Italian context, the so called “badanti” (representing the portion of foreign paid caretakers for the elderly), which were not taken into account in this review (e.g., [62]). While informal care often remains uncompensated (e.g., [67, 92]), there is a discernible rise in the presence of remunerated informal caregivers who are replacing or complementing the informal care given by relatives [93]. The composition of this group predominantly consists of women who have migrated either permanently or temporarily, with or without qualifications, and are remunerated under several regulations [93]. This would provide a more comprehensive exploration of the topic concerning the characterization of the requirements of informal carers, specifically focusing on this particular group of helpers of family caregivers that is prevalent in Italy (e.g., [25]).
Limitations
Although the systematic reviews yielded valuable findings, certain limitations were identified. The systematic review was conducted utilizing a restricted set of databases, namely Scopus, IEEE Xplore, and ACM Digital Library and the search query employed may have been constrained by the selection of keywords. Specifically, terms pertaining to the subject matter, such as “innovative assistive technology” [91] and “ambient assisted living” [9], were not incorporated. It is possible that certain papers may have been unintentionally excluded from the systematic review. However, given the purpose of this systematic literature, our findings may guide further opportunities of research in the field of AI and informal care.
Future developments
Additional potential for growth may arise from a methodological standpoint. Systematic reviews are essential for progressing research, but they need a significant amount of time and resources [14]. Performing a systematic review is an expensive process that typically involves more than a year of effort from a group of researchers [12]. It entails manually evaluating numerous titles and abstracts, which can be difficult to do promptly and thoroughly, especially when the research topic is time-sensitive [31]. Artificial intelligence indeed is expected to play a crucial role in intelligent technology utilised in long-term care for older people [56]. As a result, there are pressing demands at both the national and international levels to identify preventive, sustainable, and cost-effective strategies that can assist carers [29].
Reviewing titles and abstracts was a crucial step in this systematic review (e.g., [16]). The assessment of the significance of studies identified in the initial search to decide whether they should be included in the systematic review has been acknowledged in the literature as the most time-consuming and demanding task [14]. Learning an algorithm for automating the screening process, selecting, and categorising study abstracts can help quickly pinpoint studies needing additional examination, particularly given the rapid expansion of scientific knowledge [14]. Active learning enables the machine learning (ML) model to enhance its predictions on unlabeled data by choosing the specific records from which to learn repeatedly [31]. The model delivers the records to a human annotator for labelling, which is subsequently utilised by the algorithm to adjust its predictions [31]. Several studies started incorporating AI-tool assisted screening system using active learning to streamline the abstract and title screening phase in the development of systematic reviews (e.g., [38, 40]). The ASReview software [96] has become increasingly popular among researchers, and its ability to lessen screening workload has been proven in past retrospective screening simulation studies [14]. By utilising text mining and an active research-in-the-loop machine learning algorithm, ASReview ranks articles according to their likelihood of meeting the inclusion criteria [97]. When combined with carefully chosen stopping criteria, it can significantly reduce the amount of papers to review, while also lowering the chance of missing any crucial studies [101]. Contrasting a conventional screening method with AI-assisted screening systems using active learning is not the focus of this section. This section simply aims to outline the methodological approach for automating the screening process using an alternate strategy that includes an active research-in-the-loop machine learning algorithm. The aim is to facilitate additional research in this study’s topic also from methodological standpoint.
Machine learning-assisted systematic review workflow
Screening of the titles and abstracts of a subset of the original dataset used in this study was conducted using the ASReview tool to simulate an AI-aided systematic review process for the screening stage. Following the guidelines by van de Schoot et al. [96], the abstract and title screening phase with AI-assisted screening system using active learning was organized into three steps: preparing data, selection of prior knowledge and running the trained model.
The original dataset extracted from Scopus (778 articles) was selected. Prior to uploading the dataset to the AI-aided system for screening prioritisation, it was necessary to check for deduplication in order to begin filtering abstracts and titles using the AI tool. No duplicates were found using EndNote (version 2.4). The dataset with no further deduplication required was uploaded to ASReview.
A machine learning classifier was trained to forecast study relevance (represented by labels) from a feature space consisting of a representation of the text containing the records using prior knowledge [96]. Since the systematic review was already performed, the reviewers have fully understanding on the background knowledge on the topic. However, since the dataset was extracted without updating the search by the original search string, it might be appropriate to create a simulating scenario where the reviewer select some key records to include and to exclude without screening random articles to identify the relevant or irrelevant ones. The algorithm was trained with a collection of labelled instances, including three relevant papers and three irrelevant papers as selected prior knowledge.
Subsequently, the active learning model was established through the configuration of the balance strategy, feature extraction approach, classifier, and query strategy. The feature extraction strategy utilised in the default option was frequency-inverse document frequency (TF-IDF), the classifier employed was naive Bayes, the query strategy utilised certainty-based sampling, and the dynamic resampling technique was used to address the unbalanced nature of the data. The default option was chosen due to its better performance in past experimental settings across multiple datasets as well as its low computational time [96], making it suitable for our purpose of getting preliminary insightful on the potential advantages of semi-automating the traditional systematic literature review. Running the model, a preliminary list of unlabeled articles sorted by their likelihood of relevance, with the top-ranked articles being the most probable to be relevant [97] was obtained. Upon reviewing the article against the inclusion criteria, the updated classification of the abstracts (whether they are relevant or irrelevant) was incorporated into existing knowledge, and the ranking was adjusted accordingly using all available information [71]. The unlabeled articles were continuously updated as each top-rated article was reviewed by the author [71] until a specified stopping rule was met. A built-in mechanism to stop screening is missing in the ASReview tool [71]. Nevertheless, literature provides multiple halting conditions [71]: sampling criteria, where the stopping rule is the achievement of a predefined threshold of the top-ranked articles screened in the active learning cycle, such as 10% (e.g., [101]); heuristic criteria, where reaching a pre-defined number of consecutive irrelevant articles, such as 50 consecutive irrelevant articles (e.g., [97]) or 100 consecutive irrelevant articles (e.g., [71]) is the stopping rule. The halting condition of 100 consecutive irrelevant articles was chosen for the simulation scenario. The stopping criterion was met when 244 articles were labeled by getting a reasonable proportion of articles eligible for full-text screening with a time-saving benefit.
Albeit not being comprehensive and lacking generalizability also due to the absence of performance metrics, the simulation scenario provides a preliminary indication of the potential for integrating AI tools based on active learning to boost the efficiency in the abstract selection process. This sets the stage for advancements that could involve implementing new methodological techniques to enhance the screening process of traditional systematic reviews by automating tasks with AI-based technologies utilising an active learning strategy.
Conclusions
The aim of this systematic review was to thoroughly investigate the most recent advancements in AI-enabled technologies, as well as those encompassed within the broader category of assistive technology, which are designed with the primary or secondary goal to assist informal carers. The review sought to identify the specific needs that these technologies fulfill in the activities related to the care of older individuals. Our findings indicate that AI-powered technologies play a significant role in facilitating ambient assisted living applications, wherein the integration of home sensors and wearable devices predominantly serves to improve the remote monitoring needs of informal caregivers. In addition, AI-powered solutions contribute to improve care coordination between formal and informal caregivers: this could result in advanced telehealth assistance and pave the way for additional research on the integration of emerging technologies to facilitate intelligent healthcare solutions in remote areas. The subset of the remaining assistive technologies, such as robots and mHealth apps, were limited suggesting that those technology need to be further explored in the supporting tasks they can provide. While AI and sensor-based solutions have been found to provide caregivers with valuable information for making informed decisions in their duty of care, a limited number of studies have explored the specific personal support needs that may strengthen the potential empowerment of informal caregivers. Since there appears to be insufficient focus on appeasing specific user groups based on the type of informal care they provide, future AI-based solutions and assistive technologies may benefit from a more targeted approach to design. Potential areas for future research include the integration of novel methodological approaches to improve the screening process of conventional systematic reviews through the automation of tasks using AI-powered technologies based on active learning approach.
Footnotes
Acknowledgments
We thank Davide Donato Russo for his contribution to the development of the first part of the research. We thank Maria Teresa Ambrosio for her contribution to the discussion regarding the definitions of caregiving.
This publication was produced with the co-funding of European Union – Next Generation EU, in the context of the National Recovery and Resilience Plan, PE8 “Conseguenze e sfide dell’invecchiamento”, Project Age-It (AGE – IT – A Novel Public-private Alliance to Generate Socioeconomic, Biomedical and Technological Solutions for an Inclusive Italian Ageing Society – Ageing Well in an Ageing Society) – AGE-IT-PE00000015 – CUP: H43C22000840006.